Neuromuscular choristoma (NMC) is a rare benign tumor involving nests of myocytes and neural elements that primarily affects peripheral nerves, and much less commonly can present intracranially, involving cranial nerves. It has previously been called a hamartoma or benign triton tumor. Patients typically present in the first two decades of life with cranial nerve palsies and generalized neurologic symptoms.
A 31-year-old woman presented with three days of progressive debilitating diplopia and retro-orbital pain. Imaging revealed a cystic enhancing lesion with intralesional hemorrhage near the right cavernous sinus extending into the posterior orbit through the superior orbital fissure, with scalloping of the adjacent sphenoid bone. Resection was performed through a pterional craniotomy. Pathology revealed cystic structures with portions of smooth muscle and fibrous neural elements, consistent with neuromuscular choristoma.
A literature review of choristoma (and other names for the same pathology) revealed 22 previously reported cases. The average age at diagnosis was 25 years. There were no sex differences. About half of cases arose from the vestibulocochlear nerve and were mistaken for vestibular schwannoma. Most patients had progressive symptoms over an average of 4 years. Our case demonstrated rapid progression, likely attributable to intralesional hemorrhage. Imaging findings can differ but include smooth bony scalloping on CT due to slow growth as well as heterogeneous enhancement and presence of cystic components on MRI. Ultimately, diagnosis relies on tissue examination.
We report the first described case of NMC with intralesional hemorrhage, causing acute onset of symptoms, adding to the existing literature of this rare nerve tumor mimic for which there is currently a lack of breadth of descriptive cases. NMC is a benign lesion with typically slow growth patterns usually found in relationship with cranial nerves of which surgeons should be aware as it can be safely managed with maximal subtotal resection and serial imaging to salvage neural function.
Neuromuscular choristoma, Cranial nerves, Hamartoma, Benign triton tumor
Choristoma is a rare pathology involving organized nests of cells in an abnormal location. There have been multiple historic names for this tumor, including rhabdomyoma [1], benign triton tumor [2], neuromuscular choristoma [3], and neuromuscular Hamartoma [4] among others. Neuromuscular choristoma (NMC) is a rare class of choristoma composed of striated or smooth muscle mixed with neural elements and other tissues that primarily involves peripheral nerves but has been reported to arise within the cranium affecting cranial nerves [5]. One recent comprehensive literature review showed a total of 22 described cases of NMC involving cranial nerves [5].
All previously reported NMC's have been described as arising from or affecting a single cranial nerve including the vestibulocochlear, facial, trigeminal, oculomotor, and optic nerves (in descending order) [5]. Symptoms are usually caused by mass effect on the nerve of origin, typically resulting in cranial nerve palsies. Symptom progression virtually always corresponds with a slow-growing tumor, and most patients present with many years of worsening symptoms. The most rapid reported progression was the first described case of NMC, in which a 2-year-old boy presented with one month of fussiness [6].
Intracranial neuromuscular choristoma is an important nerve tumor mimic, and there is a lack of breadth of descriptive cases of this type of tumor. Here, we describe a case of NMC involving the oculomotor, trochlear, and ophthalmic branch of the trigeminal nerves in a woman with visual changes and pain over the course of three days. To our knowledge, this is the most rapidly progressive described case of NMC and likely represents the first report of hemorrhage into a choristoma.
A 31-year-old female with past medical history of a reportedly benign right-sided brain tumor incidentally discovered 12 years prior who presented with several days of diplopia and pain behind her right eye. The diplopia and severe headache progressed rapidly, and the patient could no longer drive or work within three days of onset. On exam, she exhibited a right partial cranial nerve three and six palsy, with right sided proptosis, a dilated and minimally reactive pupil, and extremely limited extraocular movements in all directions. She also had facial numbness in the right V1 distribution.
Of note, 12 years prior, the patient was involved in a car accident and a CT head and MRI brain reportedly showed a benign right-sided brain tumor, asymptomatic at the time. She was lost to follow-up due to lack of insurance. Outside images were unable to be obtained for review, however the report demonstrated similar size measurements.
On presentation, CT imaging demonstrated a multicystic osseous lesion arising from the right sphenoid wing and extending into the right orbit with hyperdense components ventrally consistent with hemorrhage and smooth scalloping and thinning of the sphenoid bone and anterior clinoid process. MRI brain demonstrated a 3.8 × 1.8 × 2.7 cm cystic lesion with peripheral enhancement centered in the right superior orbital fissure with widening of the fissure (Figure 1). The lesion was predominantly T2 hyperintense, although there were some areas of T2 hypointensity and T1 hyperintensity consistent with subacute hemorrhage. Based on imaging, the differential diagnosis included a vena lymphatic malformation, schwannoma, and less likely dermoid tumor, and direct cranial nerve involvement was not anticipated.
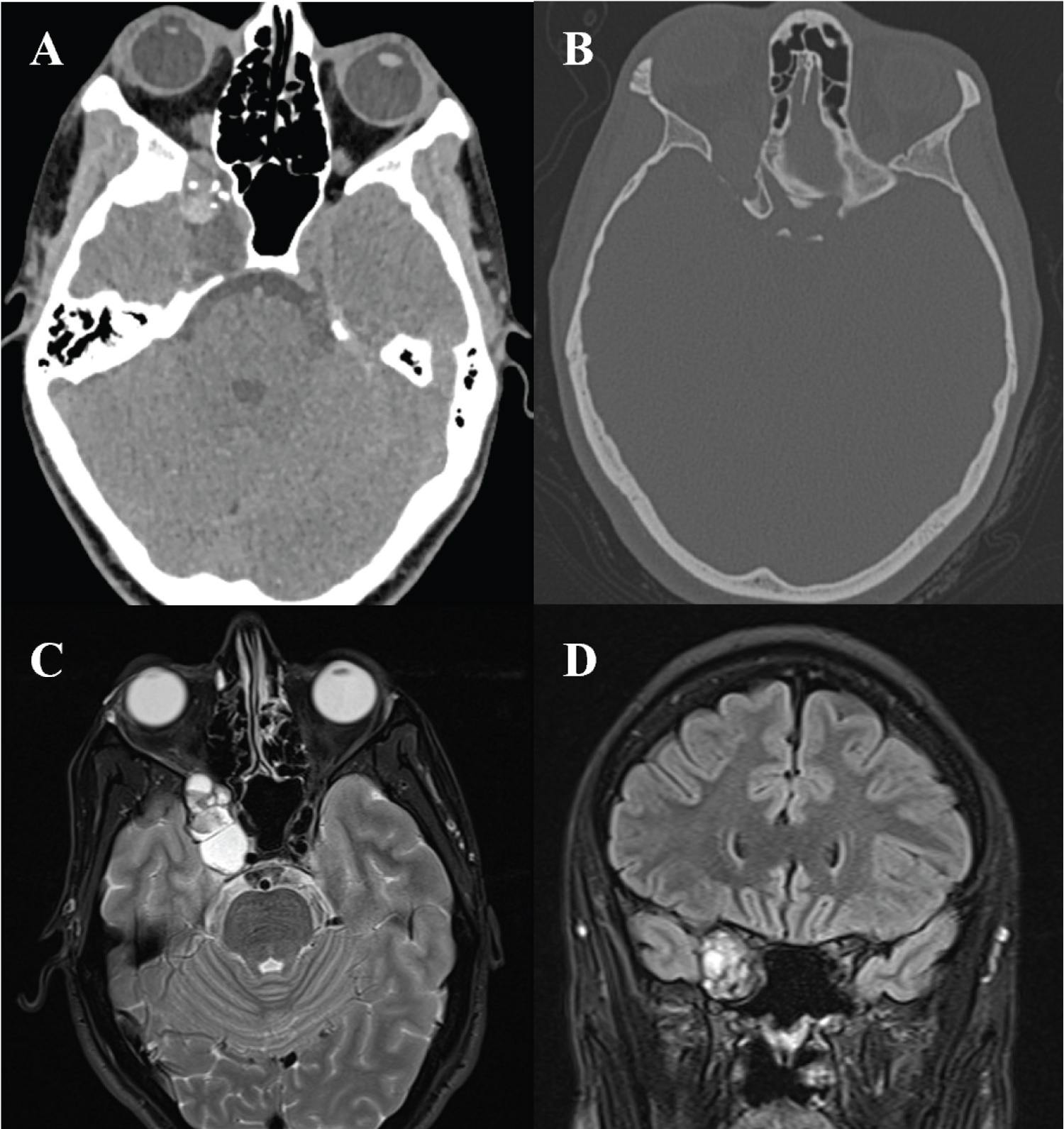 Figure 1: A) Axial non-contrast CT demonstrating the mixed density lesion centered within the orbital apex with hyperdense components posteriorly likely representing hemorrhage and scattered calcification; B) Axial CT bone window demonstrating smooth bony remodeling and expansion; C-D) T2-weighted axial; C) Coronal; D) MRI demonstrating a 3.8 × 1.8 × 2.7 cm hyperintense cystic mass centered within and causing widening of the superior orbital fissure, extending through the annulus of Zinn and into the right posterior orbit.
View Figure 1
Figure 1: A) Axial non-contrast CT demonstrating the mixed density lesion centered within the orbital apex with hyperdense components posteriorly likely representing hemorrhage and scattered calcification; B) Axial CT bone window demonstrating smooth bony remodeling and expansion; C-D) T2-weighted axial; C) Coronal; D) MRI demonstrating a 3.8 × 1.8 × 2.7 cm hyperintense cystic mass centered within and causing widening of the superior orbital fissure, extending through the annulus of Zinn and into the right posterior orbit.
View Figure 1
The patient underwent right pterional craniotomy for resection of the lesion. Intraoperatively, the lesion was found to be completely extradural and spanned the orbit, annulus of Zinn, superior orbital fissure and anterior middle fossa. The lesion was intimately involved with cranial nerves III, IV, and V1 within the lateral superior orbital fissure. Multiple cysts were drained including one that was hemorrhagic. A near total resection was achieved except for a small amount of residual at the annulus of Zinn. Pathology revealed small cystic structures lined by bland mucinous and respiratory-type epithelium as well as portions of smooth muscle, adipose tissue, fibrous tissue, nerve tissue with fibrosis.
The patient was discharged home on the second postoperative day, at which time her exam demonstrated equal and reactive pupils, slight improvement in right eye extraocular movements, and normal facial sensation.
To our knowledge, this is the most rapidly progressive case of NMC described to date, which demonstrates the potential for intralesional hemorrhage, not previously described. Although the lesion had likely been found incidentally 12 years prior, the patient never experienced symptoms until her swift deterioration within days. Our case adds to a paucity of reports on intracranial choristoma, complicated by inconsistent terminology. These lesions were called rhabdomyomas due to an abundance of striated muscle cells, then later "benign triton tumors," stemming from the Triton salamander's ability to regrow muscle tissue through local neural signaling. We performed a comprehensive search for intracranial choristoma, rhabdomyoma, and benign triton tumor and found the term "neuromuscular choristoma" most consistently used since 2007 (Table 1) [7-24]. The pathogenesis of neuromuscular choristoma is unclear, particularly for those occurring intracranially. Two theories include neoplasm or developmental malformation [5]. The neoplastic theory is supported by neuroectodermal precursors and glial cells can self-induce differentiation to mesodermal mature skeletal muscle cells [25]. Alternatively, mesenchymal precursors may be trapped in a nerve sheath as it extends peripherally [26].
Table 1: Reported cases of intracranial neuromuscular choristoma, adapted from Coli, et al [5]. View Table 1
The average age at diagnosis of NMC was 25.8 years (range 2 to 68), without sex predilection. This tumor is most often associated with certain cranial nerves; most commonly the eighth cranial nerve, followed by the fifth, seventh, third and second nerves. Given involvement of the superior orbital fissure, the tumor in our case was intimately involved with multiple cranial nerves (III, IV, V1) which had not been described before. Symptoms often progress over months to years. Our review showed an average duration of 4.1 years with our case as the most rapidly progressive due to intralesional hemorrhage. Diagnosis of choristoma remains difficult. Imaging characteristics appear to be highly heterogenous, although many enhance with contrast, albeit in an inconsistent pattern [11]. As in our case, there is often benign expansion of the surrounding bony structures with smooth scalloping due to slow growth. The characteristic microscopic appearance is nests and fascicles of well-differentiated striated or smooth muscle with intermixed neural fibers in a perimysium sheath [2,26].
Because of the scarcity of reported cases, the standard of care for intracranial choristoma is yet to be established. The decision to resects the lesion should be based on clinical symptoms, and the degree of resection should be determined based upon careful analysis of intracranial imaging with respect to the surrounding structures. Gross total resection is generally considered curative but may not be achievable without cranial nerve sacrifice. In the reported cases above, subtotal resection generally has excellent patient outcomes. Although long term follow-up is inconsistent, none have reported tumor regrowth. In general, NMC should be treated as a benign lesion with subtotal resection as needed to save neurologic function, with the potential for excellent outcome.
NMC is a rare benign tumor that is important to include in differential diagnoses of cranial nerve lesions. Symptoms are usually slowly progressive and related to mass effect of the associated cranial nerve. Imaging characteristics include a heterogeneously enhancing lesion in close proximity to cranial nerves, often associated with cystic components and smooth bony remodeling. We describe the first reported case of intralesional hemorrhage within a NMC leading to rapid symptom progression. While rare, knowledge of this tumor is critical to prevent sacrifice of function to achieve total resection, given its benign and indolent nature.
There are no conflicts of interest or financial disclosures to disclose.
All authors have contributed equally.