Shunt malfunction is a life-threatening cause of altered mental status and ventriculomegaly in patients with shunted hydrocephalus. While shunt malfunction should be highest on the differential for such patients, there may be additional toxic/metabolic derangements that are contributing to their presentation that should not be overlooked. Here we present the case of a 41-year-old woman with shunt dependent hydrocephalus presenting with altered mental status and ventriculomegaly on intracranial imaging. When the patient continued to have intermittent altered mental status and ventriculomegaly despite cerebrospinal fluid drainage, careful review of laboratory findings found that imaging findings and symptoms correlated with periods of severe hypernatremia. This case report highlights the need to distinguish encephalopathy secondary to metabolic abnormalities from shunt malfunction, and need to potentially treat with urgent, non-surgical therapies in patients presenting with metabolic abnormalities that could mimic shunt malfunction.
Ventriculomegaly, Ventriculoperitoneal shunt, Hydrocephalus, Hypernatremia
Hydrocephalus is a pathologic accumulation of cerebrospinal fluid (CSF) within the ventricular system which can lead to elevated intracranial pressure (ICP), altered mental status, and ventriculomegaly on intracranial imaging. Treatment is dependent on underlying pathology, including resection of obstructive lesions, third ventriculostomy in the case of aqueductal stenosis or fourth ventricular pathology, or shunting in cases when the cause of obstruction or failed CSF absorption cannot be eliminated [1-9]. Shunt malfunction can lead to rapid accumulation of CSF with elevated ICP, altered mental status, and ultimately brain herniation and death [6,7]. While shunt malfunction should be highest on the differential for a patient with shunted hydrocephalus presenting with altered mental status and ventriculomegaly, patients with hydrocephalus may have additional comorbidities which may contribute to their presentation. Here we present a case of a patient presenting with altered mental status and ventriculomegaly on CT scan who was originally assumed to have shunt malfunction but was instead found to have a functioning ventriculoperitoneal shunt (VPS) with findings caused by episodic hypernatremia and resultant “ventriculomegaly”.
A 41-year-old female with history of infectious meningitis and long-standing VPS requirement presented to the emergency department in a coma. She had a complex shunt history due to the previous bacterial meningitis with severe resulting adhesions and cervicothoracic syringomyelia requiring posterior fossa decompression adhesionolysis and duraplasty and ultimately a syringopleural shunt placement, in addition to multiple VPS revisions. CT head obtained on arrival showed ventriculomegaly compared to stability imaging (Figure 1A and Figure 1B). At this time she also had significant laboratory abnormalities including hypernatremia (Na + 158 MMOL/L), lactic acidosis (2.23 MMOL/L), acute renal failure (creatinine 1.38 MG/DL), impaired liver function (INR 2.38), and a urine drug screen positive for methamphetamines, barbiturates, benzodiazepines, and buprenorphine. Due to the significant metabolic and hematologic abnormalities, immediate operative intervention with ventriculoperitoneal shunt revision was contraindicated and an external ventricular drain (EVD) was placed for cerebrospinal fluid (CSF) diversion. The patient’s neurological exam did not improve with external CSF drainage, but began to improve after normalization of laboratory values as she was treated for hypernatremia, thrombocytopenia, and hypotension believed to be secondary to dehydration after drug overdose. During this time the external ventricular drain had minimal output at 5 cm above the EAC, and transduced intracranial pressures remained less than 10 cm H 2 O, even after clamping for 72 hours. A nuclear medicine study was performed which showed that the shunt catheter was patent from the ventricles to the abdomen with rapid ventricular drainage. Additionally, patient developed a thin left subdural hematoma consistent with over drainage of CSF. CT head was obtained 3 and 5 days after clamping which showed normalization of ventricular size back to her baseline (Figure 1C) and the patient had regained normal neurologic function. With this preponderance of data, we concluded that ventriculoperitoneal shunt was functioning appropriately and did not proceed with shunt revision. The external ventricular drain was removed, and the patient was transferred to the neurosurgical floor. Two days after transfer to the floor she was once again found altered; lethargic, nonverbal, and withdrawing only to noxious stimuli. CT head again showed enlarged ventricles (Figure 1C), and labs were obtained showing Na + of 167 MMOL/L. Large volume shunt tap (30 cc) was performed with low opening pressure, good flow, and no improvement in mental status. She was transferred back to the neuro ICU and was reinitiated on treatment for hypernatremia from diabetes insipidus. With resolution of hypernatremia two days later (Na + to 145 MMOL/L), the patient’s mental status returned to baseline, and the ventriculomegaly once again resolved on CT head (Figure 1D). Throughout the hospital course, the patient’s mental status waxed and waned, correlating with Na + level and ventricular size. Ultimately, the patient was stabilized on a standardized dose of nasal vasopressin for treatment of diabetes insipidus with the assistance of endocrinology, and remained at her neurological baseline without shunt revision.
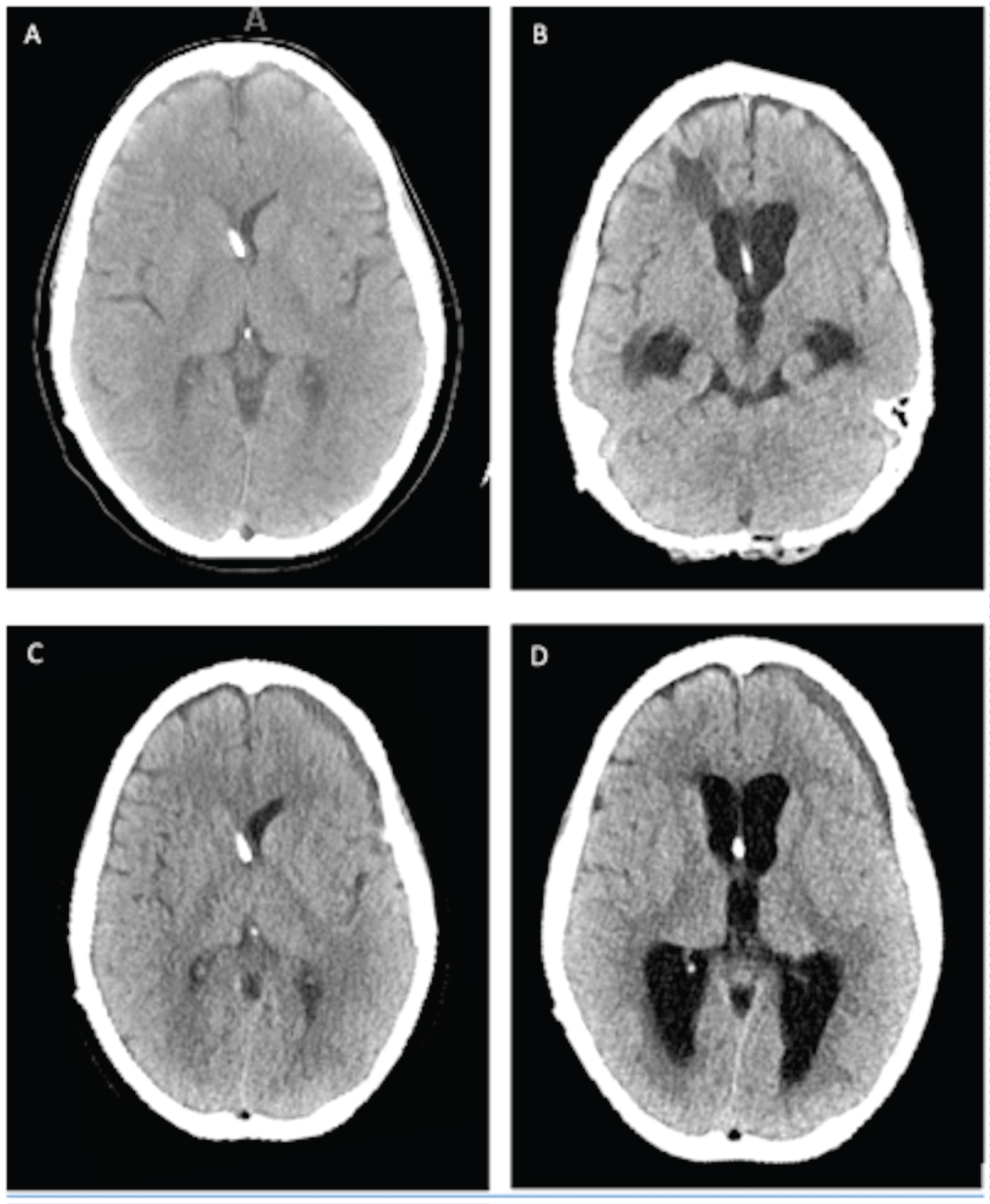 Figure 1: A) Patient's baseline CT head at time shunt was known to be functional; B) Patient's CT head on time of arrival, with Na+ 158 MMOL/L; C) CT head 4 days later, after initiation of treatment for diabetes insipidus, with Na+ 145 MMOL/L; D) CT head following recurrent altered mental status, with Na+ 167 MMOL/L.
View Figure 1
Figure 1: A) Patient's baseline CT head at time shunt was known to be functional; B) Patient's CT head on time of arrival, with Na+ 158 MMOL/L; C) CT head 4 days later, after initiation of treatment for diabetes insipidus, with Na+ 145 MMOL/L; D) CT head following recurrent altered mental status, with Na+ 167 MMOL/L.
View Figure 1
Shunt malfunction is a life-threatening event in patients with shunt dependent hydrocephalus that must be quickly recognized and treated. This report underscores the importance of performing a complete medical work-up to ensure that alternative diagnoses, including serum electrolyte abnormality, is not overlooked. Full shunt evaluation in complicated medical cases may require measurement of intracranial pressure and shunt function through shunt tap, external ventricular drain monitoring, lumbar puncture or nuclear medicine studies.
Three previous case reports have been published in which hypernatremia has been found to be the cause of transient ventriculomegaly in a patient with VPS without shunt malfunction. The first case, describes a 3-year-old girl with history of myelomeningocele and hydrocephalus requiring VPS placement, complicated by shaken baby syndrome, who presented with severe dehydration secondary to antibiotic-induced diarrhea. The patient was severely hypernatremic to 180 mmol/L with CT head showing ventricular enlargement compared to baseline. In this case shunt tap was performed with low opening pressure and good flow, prompting the treating physicians to manage the patient’s condition non-operatively. Following normalization of serum sodium, the patient’s neurological function returned to baseline, with normalization of ventricular size on CT scan [4]. Another report records a patient with altered mental status and ventriculomegaly following withdrawal of scheduled vasopressin therapy prior to chemotherapy for metastatic suprasellar germinoma. After dry shunt tap this patient was taken to surgery with assumption of shunt malfunction, but intraoperatively the patient was found to have a functional proximal and distal shunt. Intraoperative laboratory values showed severe hypernatremia, and the patient returned to baseline neurological status after improvement in hypernatremia [3]. In the third case, a 4-year-old boy with history of diffuse neuroectodermal neoplasm, diabetes insipidus, and shunted hydrocephalus presented with generalized tonic-clonic seizures. He had normal intracranial imaging on arrival with Na + of 146 mEq/L. MRI brain was planned to further evaluate his tumor burden, but during this time he became unresponsive with enlarged ventricles. He underwent emergent shunt revision and the shunt was found to be functioning well, however intraoperative and post-operative labs showed a significant elevation in Na + to 160-167 mEq/L. Again, following normalization of serum sodium, the patient’s mental status improved, and ventricular size returned to normal.
Similarly, our patient had fluctuating Na + levels due to diabetes insipidus, which correlated with ventricular size. Ventriculomegaly was demonstrated during times of extreme hypernatremia, and baseline ventricular size during normonatremic periods over multiple time points, with corresponding neurological fluctuations. We hypothesize that large swings in patient’s Na + levels can override normal Na + homeostasis and lead to cellular dehydration and rehydration, dependent on the movement of water across cell membranes [8]. This Na + dependent change in ventricular size has additionally been documented in patients without history of VPS for hydrocephalus. In one such case, a patient ingested large quantity of soy sauce in a suicide attempt, causing shrinkage of the brain parenchyma with significantly enlarged subdural spaces in the setting of acute hypernatremia, which resolved after hypernatremia normalized [9]. Because physicians are so sensitive to changes in ventricular size in those with shunted hydrocephalus, electrolyte abnormalities as the cause of presentation with altered mental status and ventriculomegaly may originally be overlooked, leading to unnecessary operative interventions.
In a patient with VPS and multiple medical comorbidities there may be alternative causes to ventriculomegaly and altered mental status, and it is important to elucidate encephalopathy secondary to metabolic abnormalities that could mimic shunt malfunction in order to treat the patient with urgent non-surgical therapies. The use of shunt tap and nuclear medicine scan to evaluate shunt flow may be explored as an alternative to surgical shunt evaluation if there is high suspicion of encephalopathy due to electrolyte abnormality.
IRB approval and informed consent from patient’s legal guardian was obtained prior to submission of this manuscript.
No sources of funding to disclose.