Background: Developmental Venous Anomaly (DVA) is the most common cerebral vascular variation, frequently detected incidentally on Neuroimaging and can be associated with other pathologies. DVA is often benign and asymptomatic, however, it may rupture and cause intracerebral hemorrhage. This report presents a case of ruptured DVA successfully managed conservatively.
Case: A 15-year-old female presented with a five-day history of severe headache associated with photophobia, vomiting, and left-sided paralysis. Computer-Tomography (CT) showed intracerebral haemorrhage. On examination he was found to have photophobia, normal muscle power, and intact cranial nerves. CT and CT angiography, Magnetic Resonance Image (MRI), and MRV scans showed left cerebellar DVA with anomalous posterior fossa cerebellar draining veins managed conservatively.
Conclusion: DVA is often benign, requiring no interventions. When interventions are to be done, for instance, in the case of haemorrhage, DVA should be kept intact to avoid serious complications.
Developmental venous anomaly, Caput medusae, Venous angioma, Cerebral vascular malformation, Cavernoma
Developmental Venous Anomaly (DVA), is a congenital variation that is typically drain normal venous blood of the brain. DVA accounts for 55% of all cerebral vascular malformations, typical appearance of caput medusae sign on the radiographical image such as MRI is pathonomic. It is classically has two component, multiple collection of veins that emptying into a single trunk, either a deep ependymal vein or a dural sinus, giving a palm tree appearance on the MRI. As such it drains normal brain in a normally functional arterial territory, the normal venous pathway of the same territory however is absent [1]. It is believed that DVAs result from a focal arrest of normal parenchymal vein development or an obstruction of the medullary veins as a compensatory venous system [2]. Most DVA are asymptomatic and discovered incidentally. However, and as a result of the availability of CT scan and MRI an increasing number of published report of a symptomatic DVA in form of intracerebral hemorrhage, with numerous reports associated the DVA to stroke and epilepsy [3,4]. Histological findings reporting a dilated veins with thick walls and normal feeding arteries or capillaries, other histological finding includes hemosiderin deposits, and chronic flow impairment in the surrounding white matter [2,4]. On both a CT scan and MRI, DVA appears as a leash of vessels draining towards a central vein. A linear or curved enhancing structure, a big draining vein with multiple, small, radially oriented branches “caput medusa”, is seen on contrast CT scan [4]. Up to 9.6% of cases may show signs of dystrophic calcifications, mostly in the basal ganglia and thalami. Dilated medullary veins forming a transcortical or subependymal collector vein is an angiography pathognomonic finding. The causes of ruptured of the DVA has been proposed and that include, mechanical compression, alteration on the follow dynamic, local thrombosis or idiopathic.
DVA management leans toward no treatment, as most authors consider it as an abnormally located normal vein that drain normal subcortical brain tissue [2,3]. Nonetheless, severe complications, including intracerebral hemorrhage and venous ischemia might necessitate reconsidering our management approach to this anomaly.
A 15-year-old female presented with severe headache and sudden left-sided weakness 5 days prior to consultation, which started while she was praying and lost control of her left side. She fell down and was then transferred to the hospital where she was admitted to the Intensive Care Unit (ICU) after a CT scan showed intracerebral haemorrhage. Her mother reported the preservation of consciousness throughout, with few episodes of drowsiness.
Her headache was associated with photophobia and difficulty opening her eyes with vomiting 2-3 times a day. She also complained of mild numbness in the left side of her face, which started after she fell the first time, not associated with a seizure, no difficulty swallowing, no dysarthria, no loss of consciousness, and no weakness.
Her physical examination showed that she was vitally stable and that her pupils were bilaterally reactive. She was alert and oriented with the Glasgow Coma Scale (GCS) of 15/15 but had difficulty opening her eyes due to photophobia; otherwise, she was opening her eyes spontaneously, obeying commands, and verbalizing well. She recognized her family and was oriented to time, place, and person. Her cranial nerves were intact, and both upper and lower limb muscle power was full (5/5) bilaterally. Other systems were normal.
Imaging investigations done included CT, CT angiography, MRI, and MRV scans showing multiple variable left cerebellar DVA with anomalous posterior fossa cerebellar draining veins, slightly engorged without thrombosis or stenosis (Figure 1).
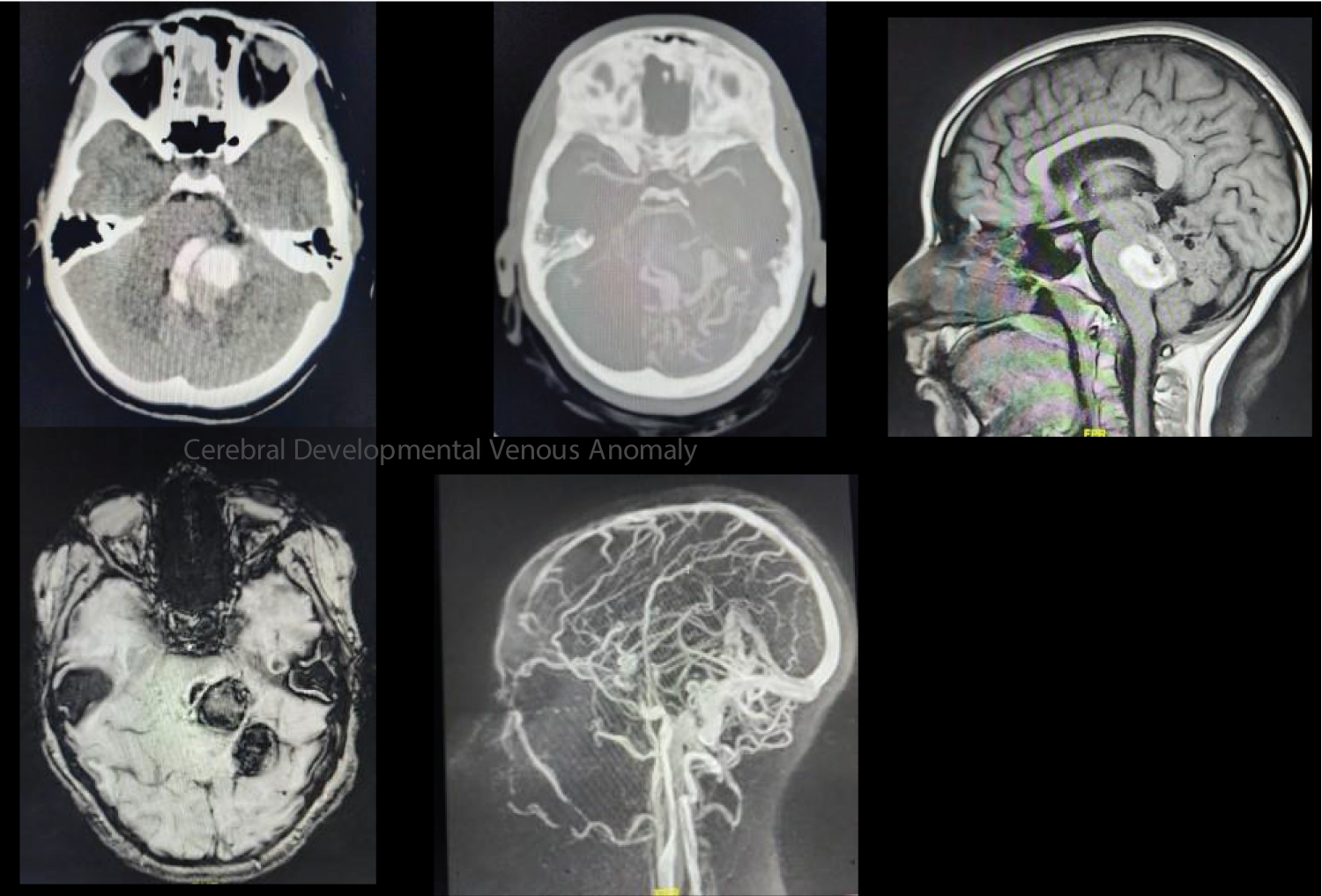 Figure 1: Multiple variables left cerebellar DVA with anomalous posterior fossa cerebellar draining veins.
View Figure 1
Figure 1: Multiple variables left cerebellar DVA with anomalous posterior fossa cerebellar draining veins.
View Figure 1
The patient was treated with observative measures without surgical interventions.
The most common accepted classification of the neurovascular malformation in the literature is due to McCormick classification, who classified cerebrovascular malformations into four main categories, including Cavernous Malformation (CM), Arteriovenous Malformation (AVM), Venous angioma, and capillary telangiectasia [1]. The term “developmental venous anomaly” was proposed first by Lasjaunias, et al. to replace all other terminology used to describe the same malformation, including McCormick entity “the venous angioma” and now is wildly agreeing up on by most expert [2]. Due to its high rate of incidental finding and low rate of complications many consider the DVA as a variation of normally vein located in abnormal location in the brain that specified to arterial territory missing the typical normal venous draining system. Though DVA has been considered rare anomaly, the introduction of the MRI to the medical filed has increase both the incident rate and our understanding to its anatomy and associated other lesions.
The development of DVA was described by many authors as an arrest of the fetus subcortical venous system as a result of a local environmental insult. Mullan, et al. associated the DVA development to the pial AVM, where an abnormal occlusion of veins draining the cortical venous plexus to the dural venous plexus occlude lead to the formation of a DVA [3]. Most of the DVAs are supratentorial estimated in about 80% and rest are located in the infratentorial [5]. Pereira, et al. proposed multiple pathomechanisms that led to the symptoms associated with DVA which they included 1) Mechanical obstruction of the DVA, 2) Flow-related, which can led to venous hypertension, and hemorrhagic as a result to increased outflow or it can lead to thrombosis if decreased outflow take place, and 3) Idiopathic symptomatic DVAs with no clear or found cause of the associated complications.
DVAs are proven to be associated with cavernous malformations (CM) in 13-40% of cases, thought to be the primary cause of most hemorrhagic cases [3]. Contrary to the DVA, which has the histological characteristics of normal veins, the CM contains abnormally enlarged capillaries with a higher risk for rupture [5]. A higher risk of a hypercoagulable state with DVA was also reported to be associated with contraceptives and protein S deficiency [6].
However, during the surgical intervention to treat hemorrhage, DVA resection must be avoided to prevent venous infarctions. The resection might cause venous congestion, CM, varices, and stenosis. Alternatively, perfusion investigations that evaluate venous congestion may be done to determine future risk factors for developing symptomatic DVAs. DVA is treated as sinus thrombosis with anticoagulant medication [4] since thrombosis in the DVA might result in hemorrhagic venous infarction [6].
There have been numerous incidences of head trauma leading to ischemic stroke, and DVAs were suggested as risk factors. In these cases, infants and children are the most affected. Ischemic stroke most frequently occurs in the internal capsule and the basal ganglia [7,8]. Though the majority of trauma-related ischemic strokes with DVA as a trigger affect newborns under the age of one, Kargl, et al. [7] recorded one in an adolescent with basal ganglia and parahippocampus ischemic stroke. DVA’s lack of elastic coating makes them more susceptible to outside forces. When coupled with immature cerebral vessels in adolescence, the likelihood of stroke and hemorrhage is high, which might have exposed our patient to the DVA rupture in her teenage years.
Additionally, a trauma in young patients results in a shear force that ruptures small vessels and causes thrombosis [4,6].
In conclusion, though DVA is mostly benign, they occasionally manifest with life-threatening complications needing interventions. DVA are malformations associated with other anomalies disrupting the venous drainage system. Regardless of the treatment, DVA must be kept intact, and other treatment modalities, though mostly observational, should be tailored to the DVA pathomechanism and complications for each patient.
None.
None.
None.