Introduction: Lumbar interbody fusion is a common procedure for addressing spinal pathologies, involving the joining of adjacent vertebrae to stabilize and alleviate pain. The evolution of interbody cages has led to the development of expandable designs that allow customization of cage size during surgery to fit each patient's anatomy.
Case series: This case series presents eight patients with radiating lower back pain, walking claudication, and signs of nerve irritation. The chosen surgical technique was transforaminal lumbar interbody fusion (TLIF), utilizing expandable RISE® interbody cages. Significant improvements were observed in the postoperative period compared to preoperative values in all cases, as indicated by the Visual Analogue Scale for Pain (VAS) and the Oswestry Disability Index (ODI) for Low Back Pain.
Discussion: Previous studies have shown that the position and characteristics of cages, along with surgical technique, influence clinical outcomes. Precise selection of interbody cages and appropriate surgical technique are crucial for optimal results in spinal surgery.
Conclusion: With ongoing technological and medical advancements, the field of spinal surgery is expected to continue evolving with advanced prosthetics aimed at enhancing patients' quality of life. Continuous research and multidisciplinary collaboration are essential to conclusively establish the benefits of these advanced techniques in spinal surgery.
Transforaminal lumbar interbody fusion, Degenerative disc disease, Low back pain
Lumbar interbody fusion is a commonly utilized surgical procedure in treating various spinal column pathologies [1]. This procedure involves the joining of two adjacent vertebrae to promote stability and alleviate pain [2]. Among the key tools widely used in spinal surgery are the interbody cages, which have evolved over time to enhance lumbar interbody fusion outcomes [3].
In 1988, Bagby and Kuslick observed a high rate of lumbar interbody fusion that provided increased spinal stability, support between vertebrae, and improved intervertebral space height [4]. In the 1990s, conventional metallic interbody fusion cages, such as titanium ones, were introduced to the market and have been used in surgical practice up to the present [5]. Despite the diversity of available interbody cages, it can be generally mentioned that they serve the function of providing a supportive structure maintaining the necessary space between vertebrae while the bone graft grows and fuses with the natural bone [3,6].
Despite their benefits, the design of interbody cages in spinal surgery is not exempt from the precision characteristic of neurosurgery. Proper selection of cage size, precise placement, and successful integration of the bone graft are critical considerations. Furthermore, there is concern that rigid and semi-rigid cages may cause additional load on adjacent vertebrae, potentially leading to long-term issues [7]. Therefore, the evolution of cages towards expandable designs addresses some of these issues by allowing adaptation and reducing stress on the spine [8].
Expandable cages signify a significant advancement in the evolution of interbody cages as they offer the ability to customize their size during surgery to fit a patient's specific anatomy. By combining flexible and structural components, they provide support to the anterior column and facilitate arthrodesis [9]. By allowing a higher degree of customization, these cages can reduce the risk of injuries to nearby structures, decrease device-related complications, and improve bone graft integration, while still maintaining the necessary intervertebral space for successful fusion [10]. Presented for the first time is a case series utilizing the expandable titanium interbody cage RISE ® (Globus Medical Inc, Audubon, PA) through transforaminal lumbar interbody fusion (TLIF) in Peru.
In the presented case series, all cases exhibit a common pattern of radiating lower back pain, walking claudication, and signs of nerve irritation on physical examination. Signs such as Lasegue, Bragard, and Dandy, along with paravertebral muscle contractures, axial pain, and signs of spinal instability, are prominent features in each case. Both pre- and post-operative assessments were conducted using the Visual Analogue Scale for Pain and the Oswestry Disability Index (Table 1). The chosen surgical procedure for these cases was transforaminal lumbar interbody fusion (TLIF), involving the use of an expandable titanium interbody cage RISE ® (Globus Medical Inc, Audubon, PA), designed to maintain vertebral height and space (Figure 1, Figure 2 and Figure 3), facilitating bone graft growth and promoting vertebral fusion.
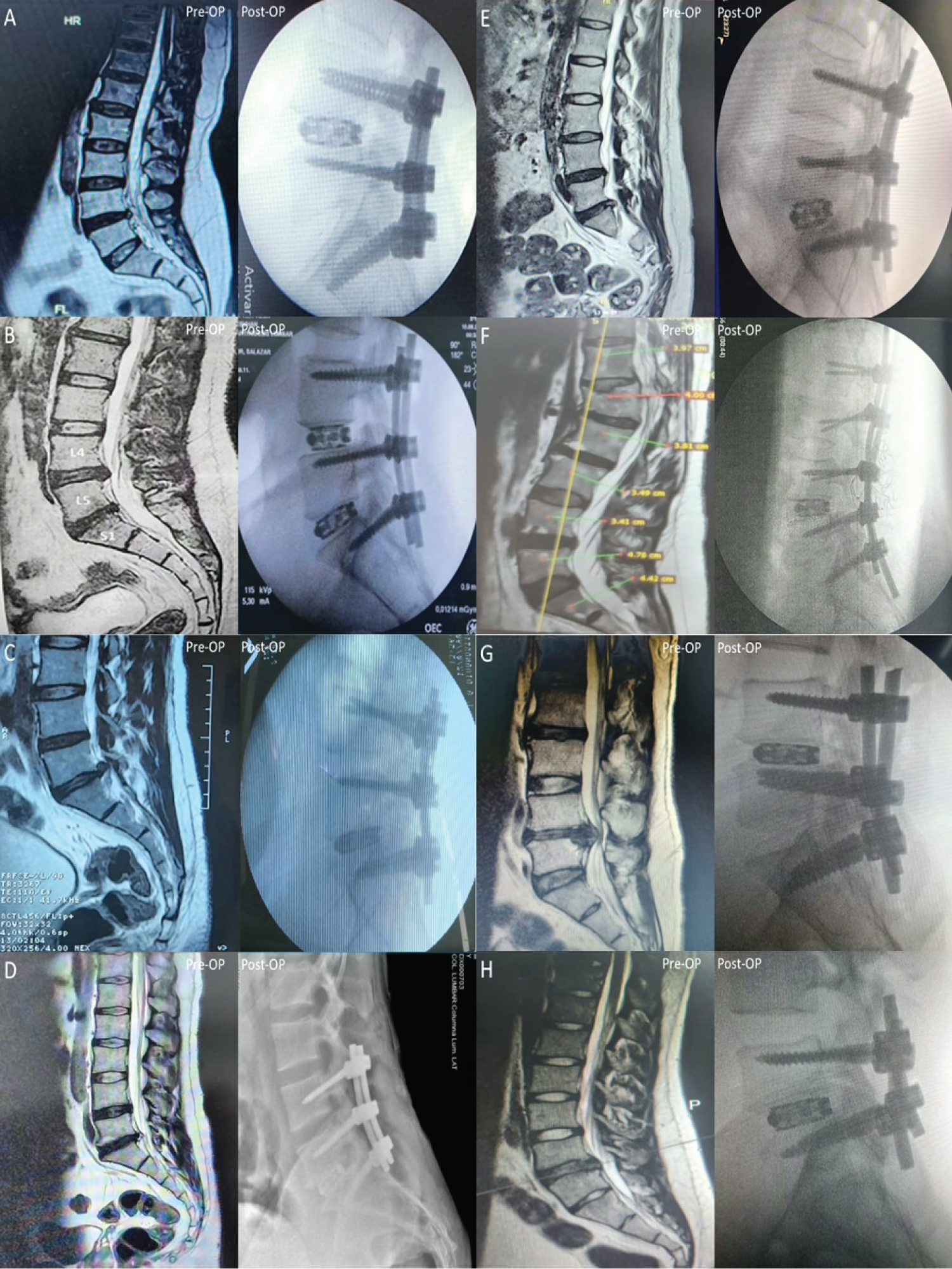 Figure 1: Comparison between preoperative and postoperative images of the case series of disc replacement via TLIF in the lumbosacral spine using expandable RISE® cages. Preoperative images depict the presence of disc herniations at different levels: L4-L5 segment (1A, 1F, 1G, 1H), L4-L5 and L5-S1 segments (1B), and L5-S1 segment (1C, 1D, 1E) with deformation of the dural sac. Postoperative images display disc replacement performed using RISE® expandable cages of varying sizes: 09 mm (1A, 1C, 1G), 10 mm (1D, 1F), 11 mm (1B, 1H), and 12 mm (1E) at the corresponding levels of the selected disc herniation, tailored to the patient's specific anatomy and needs.
View Figure 1
Figure 1: Comparison between preoperative and postoperative images of the case series of disc replacement via TLIF in the lumbosacral spine using expandable RISE® cages. Preoperative images depict the presence of disc herniations at different levels: L4-L5 segment (1A, 1F, 1G, 1H), L4-L5 and L5-S1 segments (1B), and L5-S1 segment (1C, 1D, 1E) with deformation of the dural sac. Postoperative images display disc replacement performed using RISE® expandable cages of varying sizes: 09 mm (1A, 1C, 1G), 10 mm (1D, 1F), 11 mm (1B, 1H), and 12 mm (1E) at the corresponding levels of the selected disc herniation, tailored to the patient's specific anatomy and needs.
View Figure 1
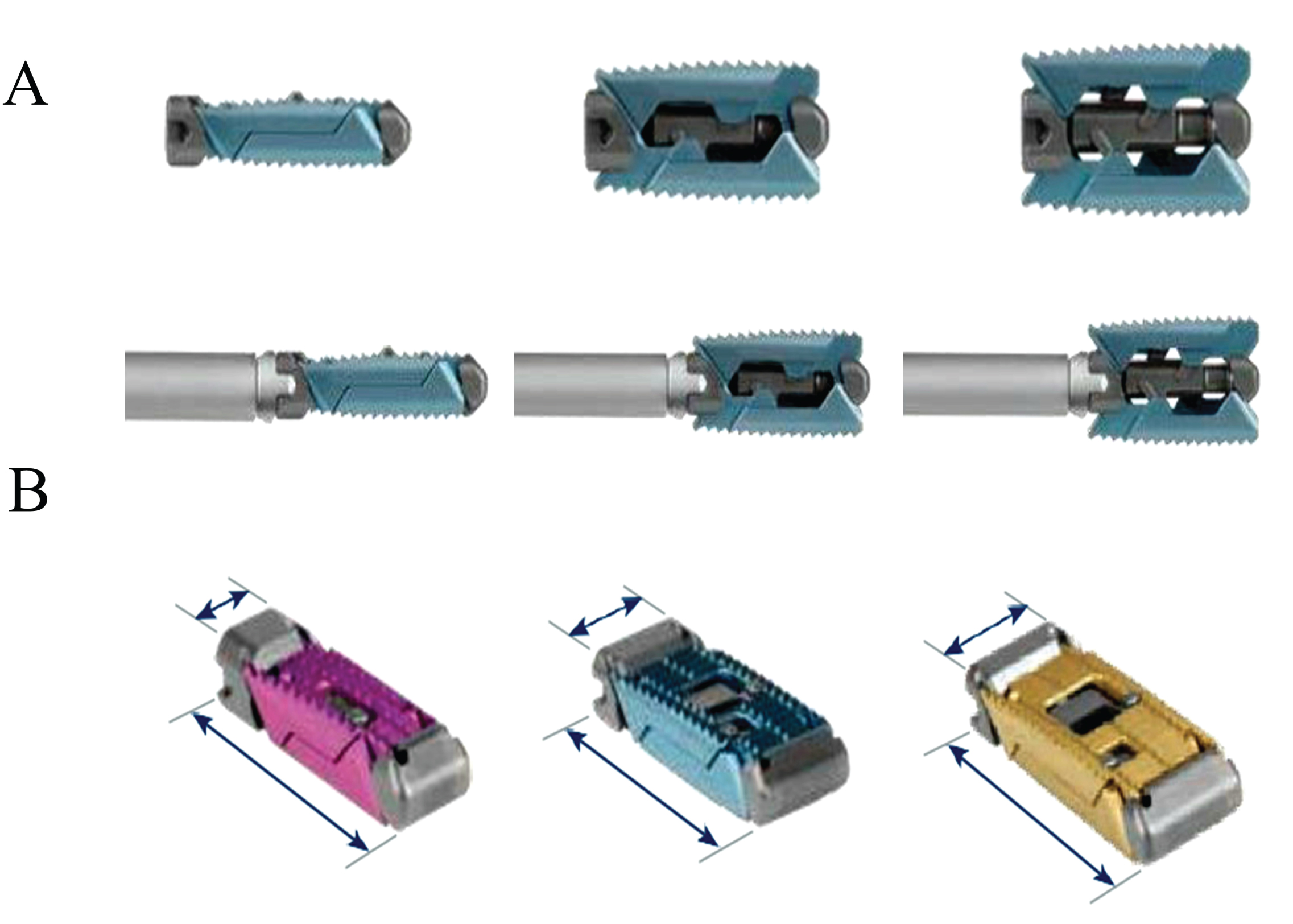 Figure 2: RISE®: Expandable Intervertebral Spacer. A. Lateral view of the expandable RISE® spacer cage, showing its progression from closed to partially open and fully open. B. The titanium-made RISE® intervertebral spacer is specifically designed for posterior approaches in the vertebral column. It provides continuous expansion options to restore the natural disc height. It is available in various dimensions: 8 mm cage (8 × 22 mm), 10 mm cage (10 × 22 mm, 10 × 26 mm, 10 × 30 mm), and 12 mm cage (12 × 26 mm, 12 × 30 mm).
View Figure 2
Figure 2: RISE®: Expandable Intervertebral Spacer. A. Lateral view of the expandable RISE® spacer cage, showing its progression from closed to partially open and fully open. B. The titanium-made RISE® intervertebral spacer is specifically designed for posterior approaches in the vertebral column. It provides continuous expansion options to restore the natural disc height. It is available in various dimensions: 8 mm cage (8 × 22 mm), 10 mm cage (10 × 22 mm, 10 × 26 mm, 10 × 30 mm), and 12 mm cage (12 × 26 mm, 12 × 30 mm).
View Figure 2
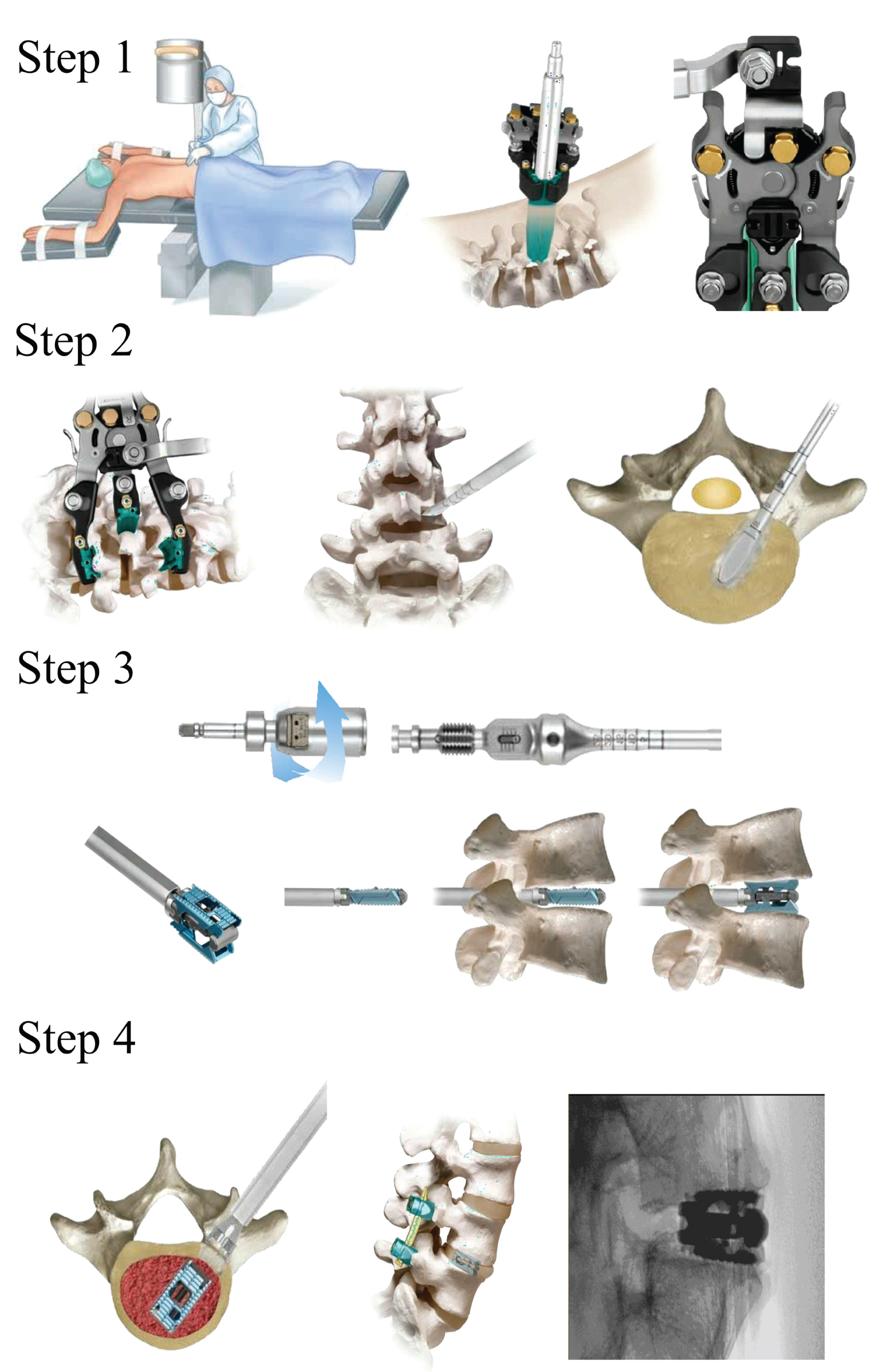 Figure 3: Surgical Technique with RISE® for TLIF Procedures in the Lumbar Spine. Step 1. Transforaminal Approach and Retraction. For the RISE® TLIF procedure, all patients are placed in a prone position. The incision, varying between 4 and 4.5 cm lateral to the midline, should follow the disc trajectory. Dissection is performed between the multifidus and long muscles until reaching the facet joint. The MARS™ 3V retractor, with its lightweight aluminum components, facilitates access to challenging disc spaces, ensuring radiolucency for clear imaging during the procedure. Once properly placed, the cannulas are removed, and fluoroscopy can be employed to verify the procedure. Step 2. Transforaminal Access and Discectomy. An instrument is used to remove the inferior facet of the cephalic vertebrae and the superior facet of the caudal vertebrae at the corresponding levels, creating a functional transforaminal access window to the disc. Subsequently, disc material is removed with a gouge. A small trial is inserted into the disc space to prepare the endplate, gradually increasing its size as needed, with caution to avoid damage. Step 3. Distraction and Implant Sizing. Following space preparation, before placing the cage, a trial is inserted to determine the required extension. Positioned as a blade, the cage is guided into place using fluoroscopy or radiography and expanded to the final size chosen by the operator. The adjustable trial assembly is utilized, adjusting the disc height using the RISE® cage, locking the removable portion of the instrument. Step 4. Final Positioning. The implant position is verified via fluoroscopy before disconnecting it from the instrument. Once the desired position is achieved, the implant introducer is disengaged by first removing the implant driver and turning the knob counterclockwise. If a change in position is required, the implant must be fully retracted. For extraction, the implant height is reduced by turning the implant driver with a torque limiter counterclockwise. Forceps or other surgical instruments can be used to grasp and remove the implant. RISE® represents an innovative solution for lumbar intervertebral fusion procedures. Its titanium construction and posterior approach design suggest exceptional durability and adaptability.
View Figure 3
Figure 3: Surgical Technique with RISE® for TLIF Procedures in the Lumbar Spine. Step 1. Transforaminal Approach and Retraction. For the RISE® TLIF procedure, all patients are placed in a prone position. The incision, varying between 4 and 4.5 cm lateral to the midline, should follow the disc trajectory. Dissection is performed between the multifidus and long muscles until reaching the facet joint. The MARS™ 3V retractor, with its lightweight aluminum components, facilitates access to challenging disc spaces, ensuring radiolucency for clear imaging during the procedure. Once properly placed, the cannulas are removed, and fluoroscopy can be employed to verify the procedure. Step 2. Transforaminal Access and Discectomy. An instrument is used to remove the inferior facet of the cephalic vertebrae and the superior facet of the caudal vertebrae at the corresponding levels, creating a functional transforaminal access window to the disc. Subsequently, disc material is removed with a gouge. A small trial is inserted into the disc space to prepare the endplate, gradually increasing its size as needed, with caution to avoid damage. Step 3. Distraction and Implant Sizing. Following space preparation, before placing the cage, a trial is inserted to determine the required extension. Positioned as a blade, the cage is guided into place using fluoroscopy or radiography and expanded to the final size chosen by the operator. The adjustable trial assembly is utilized, adjusting the disc height using the RISE® cage, locking the removable portion of the instrument. Step 4. Final Positioning. The implant position is verified via fluoroscopy before disconnecting it from the instrument. Once the desired position is achieved, the implant introducer is disengaged by first removing the implant driver and turning the knob counterclockwise. If a change in position is required, the implant must be fully retracted. For extraction, the implant height is reduced by turning the implant driver with a torque limiter counterclockwise. Forceps or other surgical instruments can be used to grasp and remove the implant. RISE® represents an innovative solution for lumbar intervertebral fusion procedures. Its titanium construction and posterior approach design suggest exceptional durability and adaptability.
View Figure 3
Table 1: Preoperative and postoperative evaluation of the case series assessed using the visual analogue scale for pain and the oswestry disability index for low back pain. View Table 1
A 48-year-old male with a history of severe lower back pain following a work-related accident involving lifting excessive weight. The pain radiated to his right lower limb, causing walking claudication, discomfort while sitting, and standing. Physical examination revealed positive right Lasegue and Bragard signs. Palpation indicated muscular contracture in the lumbar paravertebral region. Intense pain during passive movements of flexion, extension, and lateral bending of the spine, positive Dandy sign at levels L4 and L5, and walking claudication on heels.
A 39-year-old male presented with chronic lower back pain radiating to his lower limbs, walking claudication, and an inability to find a comfortable sitting or standing position. Physical examination revealed bilateral positive Lasegue and Bragard signs. Paravertebral muscle contracture was observed upon palpation. Positive Dandy sign at levels L4 and L5, intense pain during both passive and active movements, and walking claudication were noted.
A 39-year-old male complained of lower back pain radiating down his right lower limb. Additionally, he experienced walking claudication at a distance of 3 meters. During the physical examination, positive right Lasegue and Bragard signs were noted. Upon palpation, right paravertebral muscle contracture was observed. Positive Dandy sign at levels L4 and L5, along with pain during flexion and extension movements of the spine, were identified.
A 35-year-old male presented with lower back pain extending to his left lower limb and walking claudication at a distance of 3 meters. Physical examination revealed positive left Lasegue and Bragard signs. Paravertebral muscle contracture was detected upon palpation. Positive Dandy sign at levels L4 and L5, accompanied by pain during flexion and extension movements of the spine, were observed.
A 35-year-old female reported lower back pain radiating to her left lower limb and walking claudication covering a distance of 3 meters. During the physical examination, positive left Lasegue and Bragard signs were evident. Palpation revealed paravertebral muscle contracture in the lumbar region. Positive Dandy sign at levels L4 and L5, along with pain during flexion and extension movements of the spine, were reported.
A 56-year-old man presented with intense axial lower back pain radiating to his lower limbs and walking claudication. Physical examination revealed bilateral positive Lasegue and Bragard signs. Paravertebral muscle contracture was evident upon palpation. Positive Dandy sign at levels L2, L3, L4, and L5, along with pain during flexion and extension movements of the spine, were observed.
A 38-year-old man reported intense axial lower back pain radiating to his lower extremities and experiencing claudication after walking just 1 meter. Additionally, he had severe loss of strength in his left foot. Physical examination revealed bilateral positive Lasegue and Bragard signs, paravertebral muscle contracture, and a positive Dandy sign at levels L2, L3, L4, and L5.
A 24-year-old patient presented with intense axial lower back pain, radiating to the lower limbs, predominantly on the left side. Additionally, experienced claudication after walking just 1 meter and mild loss of strength in the left foot. Physical examination showed left-sided positive Lasegue and Bragard signs, paravertebral muscle contracture, positive Dandy sign at the L5-S1 level, pain during flexion and extension of the spine, and mild paresis in the left foot.
Precise surgical technique and careful selection of interbody cages contribute to enhancing clinical outcomes in spine surgery. In a retrospective study, Landham, et al. (2017) determined that the position and characteristics of the cages, along with surgical technique, correlated with improved spinal curvature and clinical outcomes in single-level posterior lumbar interbody fusion [11]. Zhang, et al. (2023) evidenced, in a retrospective study, that preoperative understanding of spinal anatomy, type and positioning of expandable interbody cages, and the surgical technique employed significantly impacted the correction of lordosis following minimally invasive transforaminal lumbar interbody fusion (TLIF) surgery [12]. Both studies demonstrate that neurosurgeons must consider a comprehensive approach balancing various factors to optimize clinical outcomes in spine surgery.
The technique of lumbar intervertebral fusion (TLIF) in treating various spinal column pathologies presents both advantages and challenges in selecting biological implants. Literature reports that pseudarthrosis after LIF occurs in 5.5-20% of cases [13,14]. LIF relies on osteobiological agents to promote bone regeneration and improve spinal fusion; hence, they should be chosen based on individual pathology, patient anatomy, and the surgeon's familiarity with available options [15,16]. Additionally, in recent decades, alternative approaches have been developed and employed, enhancing surgical outcomes of LIF through collaborative efforts among spine surgeons, bone biologists, and engineers [14]. Studies are needed to examine how osteobiological agents and alternative spine approaches enhance fusion rates.
The use of expandable cages in lumbar intervertebral fusion is associated with favorable clinical and radiological outcomes in spine surgery. Recently, Lin, et al. (2022) published a meta-analysis reporting that the utilization of expandable cages in TLIF is linked to favorable postoperative results compared to rigid cages. Although differences in anterior disc height restoration and foraminal height were statistically significant at the final follow-up for expandable cages, it was also observed that posterior disc height and segmental lordosis, while not statistically significant, exhibited beneficial outcomes in cases involving expandable cages. Furthermore, it was highlighted that expandable cages enhance functional outcomes and demonstrate superior disc height and improvement in foraminal height. However, the study's evidence level was low due to the retrospective nature of all included investigations, the heterogeneity of the studied cohort, among other limitations [17]. Hence, it emphasizes the need to standardize institutional studies internationally with the aim of raising the quality level in future works that statistically demonstrate the advantages of expandable cages.
The presented cases demonstrate the critical importance of meticulous selection concerning the size, positioning, and type of intersomatic cage, aiming to achieve successful outcomes both clinically and radiologically. Expandable intersomatic cages, such as the RISE ® titanium cage developed by Globus Medical Inc., have proven to be an effective approach in addressing various challenges associated with lumbar intervertebral fusion in spine surgery.
The ability to adjust the cage size during surgery, in accordance with the patient's specific anatomy, provides neurosurgeons with a more personalized approach and, consequently, greater adaptability. This approach reduces device-associated risks and enhances long-term functional outcomes.
Continued device research, interdisciplinary collaboration, and acquiring robust data are fundamental to establishing the benefits and effectiveness of these advanced techniques in spine surgery. As technology and scientific literature continue to advance, significant improvements in spine surgery and the quality of life for patients undergoing these procedures are likely to persist.
None.
None.
Yataco-Wilcas, Christian Alexander: Conceptualization, Methodology, Validation, Formal analysis, Investigation, Resources, Writing - original draft, Visualization, Project administration; Diaz-Llanes, Bruno Eduardo: Resources, Supervision, Writing - review & editing; Coasaca-Tito, Yosimar: Methodology, Validation, Writing - review & editing; Lengua-Vega, Luis Alberto: Methodology, Resources, Supervision, Validation; Salazar-Campos, Cristian Eugenio: Methodology, Resources, Supervision, Validation, Writing - review & editing.