The Persistent Primitive Trigeminal Artery (PPTA) is an example of persistent carotid-vertebrobasilar anastomoses, in which the basilar artery and its branches are primarily supplied by an anastomotic arterial branch originating from the cavernous segment of the Internal Carotid Artery (ICA). Such a structure constitutes the largest of fetal carotid-basilar anastomotic arteries and usually involutes after the development of the Posterior Communicating Artery (P-com). The persistence of the Trigeminal artery may be associated with other vascular anomalies, including aneurysms, arteriovenous malformations, and carotid-cavernous fistulas. We present in this study a case of persistent trigeminal artery associated with an aneurysm. Knowledge of the anatomical and angiographic characteristics of this persistent embryonic arterial channel is of utmost importance in making therapeutic decisions.
Persistent primitive trigeminal artery, Vertebrobasilar anastomosis, Aneurysm of the cavernous carotid artery
During fetal craniocerebral circulation development, four types of transient segmental connections appear between the carotid system and the rhombencephalic circulation. With the exception of the extracranial pro-atlantal intersegmental arteries, these vessels are named according to the cranial nerves they accompany [1].
Usually, these vessels disappear as the P-com arteries develop. If a segmental anastomosis fails to obliterate and persists into adulthood, it is then called a carotid-basilar anastomosis. The Trigeminal arteries are the most cephalic of the transient embryonic connections that link the fetal carotids to the paired longitudinal dorsal arteries, precursors of the vertebrobasilar system. The involution of such an artery leads to the formation of Persistent Primitive Trigeminal Artery (PPTA), predisposing to vascular pathologies such as arteriovenous malformations, aneurysms, and carotid-cavernous fistulas. Therefore, anatomical knowledge of such an abnormality is of significant relevance [2]. This study aims to describe and discuss a case of aneurysm associated with PPTA, including its diagnosis, follow-up, and management.
A.L.L.S., woman, 53-years-old, with a history of headache and previous clipping of an unruptured cerebral aneurysm of the Anterior Communicating Artery (AcoA) in 2018. During follow-up, she underwent Magnetic Resonance Angiography (MRA) 3D-TOF of cerebral vessels, which demonstrated a saccular aneurysm in the cavernous segment of the right Internal Carotid Artery (ICA), measuring 5.9 mm in its largest diameter and with a neck of 4.8 mm (Figure 1). This lesion is associated with the presence of a Persistent Primitive Trigeminal Artery on the right (PPTA), which arises immediately proximal to the aneurysm (aneurysm orientation).
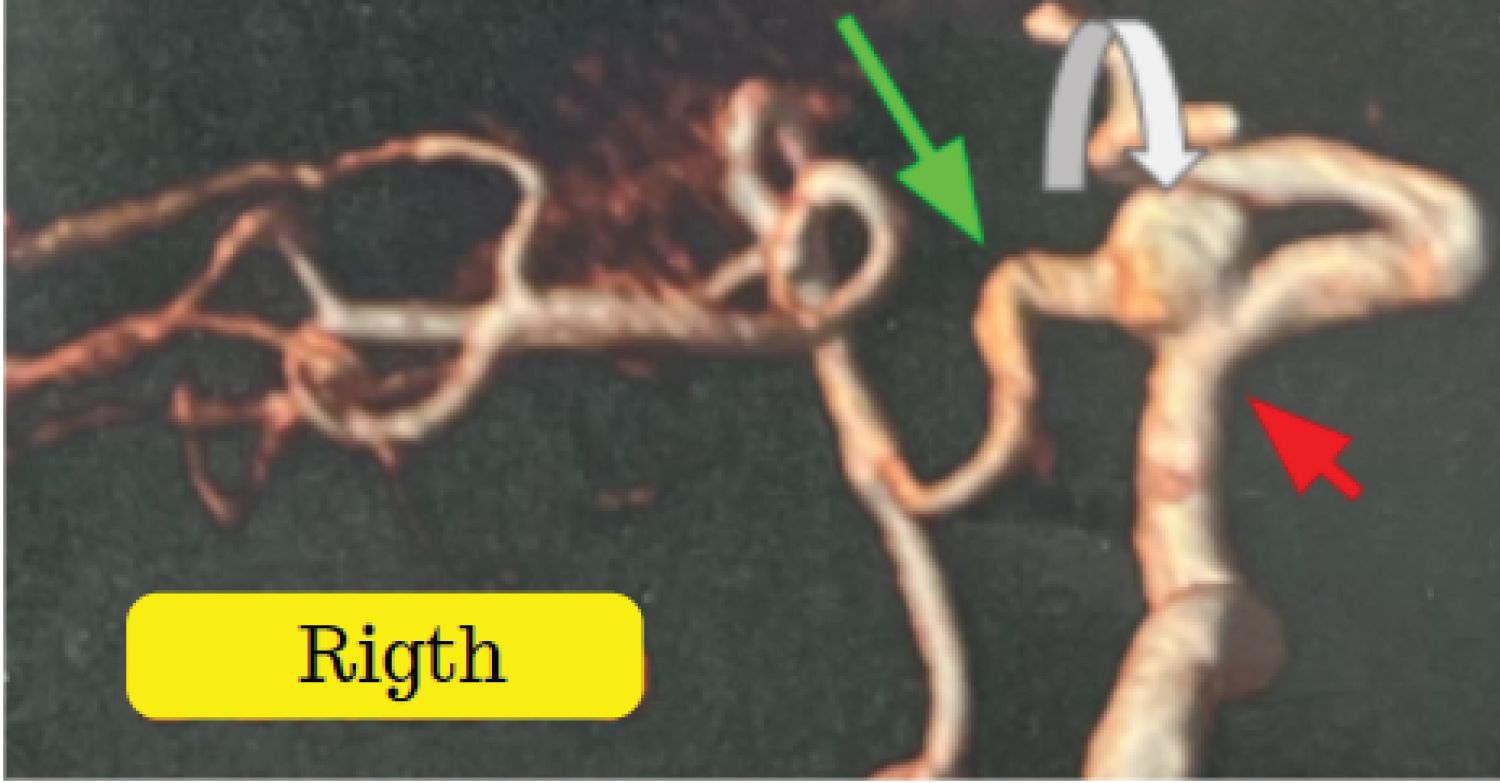 Figure 1: Arterial 3D-TOF cerebral MRA - white curved arrow pointing to saccular aneurysm, green arrow indicating persistent trigeminal artery, red arrow indicating right internal carotid artery.
View Figure 1
Figure 1: Arterial 3D-TOF cerebral MRA - white curved arrow pointing to saccular aneurysm, green arrow indicating persistent trigeminal artery, red arrow indicating right internal carotid artery.
View Figure 1
The diagnostic workup was extended with cerebral arteriography, during which the trident sign (Figure 2) compatible with Persistent Trigeminal Artery was observed, along with the absence of the right posterior communicating artery (P-com), classifying the Persistent Primitive Trigeminal Artery as type I of Saltzman. The left P-com originates from fetal circulation (Figure 3), while the right vertebral artery terminates in the right Posterior Inferior Cerebellar Artery (PICA), and the left vertebral artery is dominant (Figure 4).
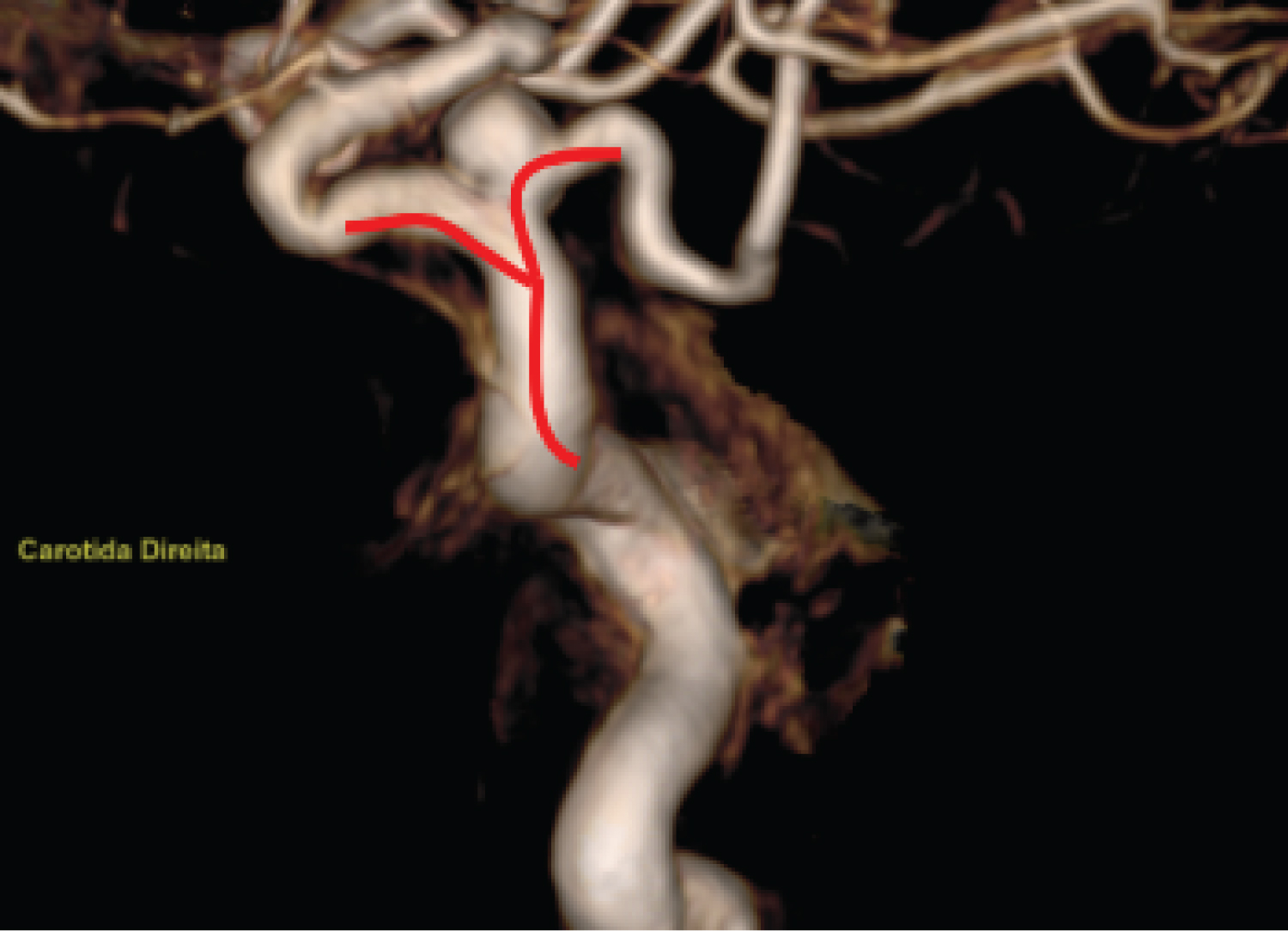 Figure 2: Arteriography of the right internal carotid artery (RICA), arterial phase, with 3D reconstruction showing the trident sign (red).
View Figure 2
Figure 2: Arteriography of the right internal carotid artery (RICA), arterial phase, with 3D reconstruction showing the trident sign (red).
View Figure 2
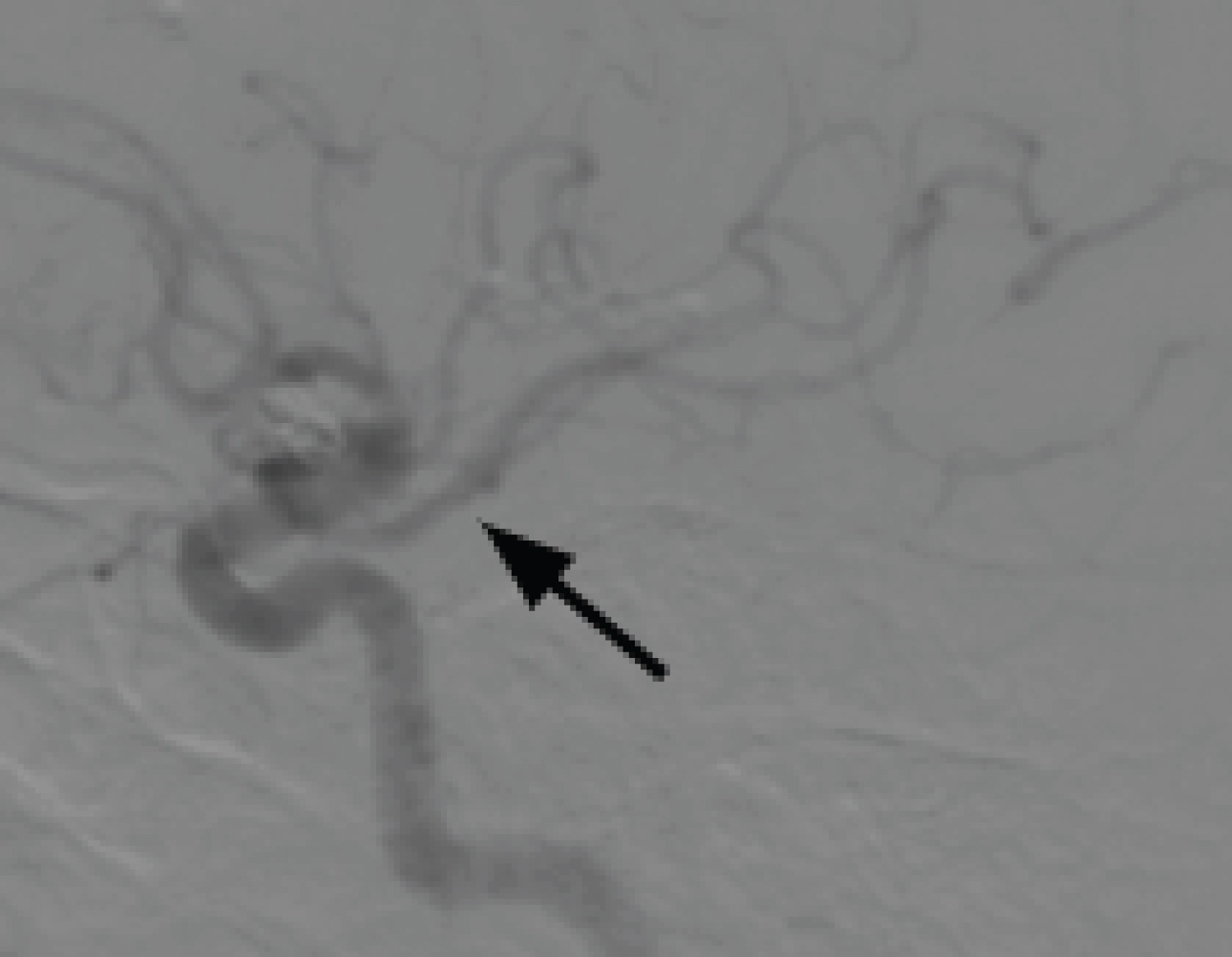 Figure 3: Profile view of left internal carotid artery arteriography (ACIE), arterial phase, black arrow indicating fetal-type left posterior communicating artery (P-com).
View Figure 3
Figure 3: Profile view of left internal carotid artery arteriography (ACIE), arterial phase, black arrow indicating fetal-type left posterior communicating artery (P-com).
View Figure 3
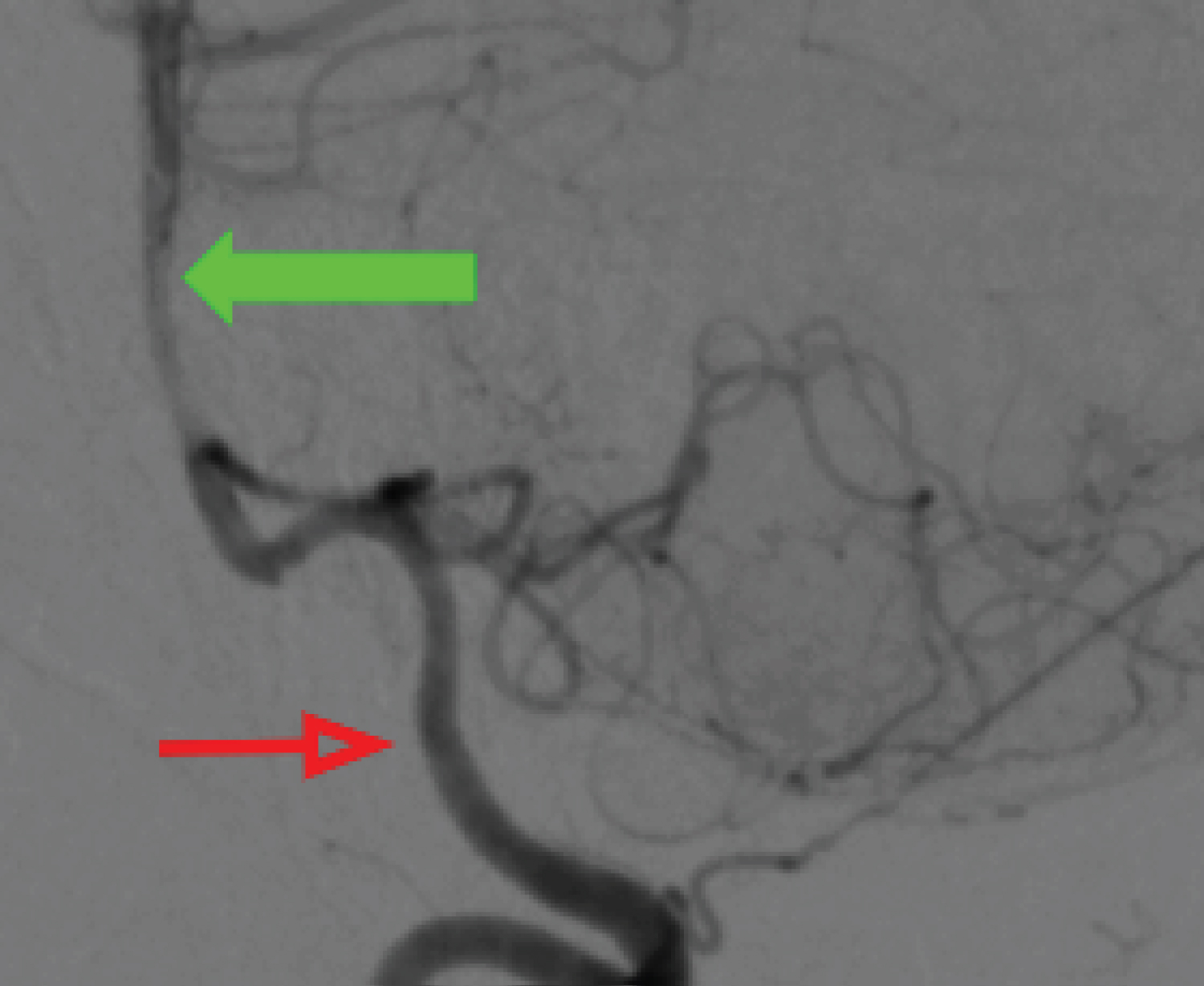 Figure 4: Dominant left vertebral arteriography in profile, arterial phase (red arrow), filling the basilar artery (green arrow).
View Figure 4
Figure 4: Dominant left vertebral arteriography in profile, arterial phase (red arrow), filling the basilar artery (green arrow).
View Figure 4
During the embryonic stage, blood supply to the rhombencephalon primarily occurs through four anastomoses between the primitive carotid system and the paired longitudinal dorsal arteries. These connections regress as the posterior communicating arteries and the vertebrobasilar system develop [3]. If regression does not occur between the anterior and posterior arterial systems, four primitive fetal anastomoses can form: Persistent Primitive Trigeminal Artery, Persistent Hypoglossal Artery, Persistent Otic (Acoustic) Artery, and Pro-atlantal Intersegmental Artery [4].
The Persistent Primitive Trigeminal Artery (PPTA) is the most common of the four anastomoses, with a prevalence of 0.02-0.6% [5]. According to Saltzman, PPTA can be classified into three types: Type 1, where PPTA supplies the entire vertebrobasilar system and the ipsilateral posterior communicating artery (P-com) is absent or poorly visualized; type 2, where PPTA fills the superior cerebellar arteries and the blood supply to the posterior circulation is predominantly through a patent P-com; and type 3, which terminates without directly anastomosing with the Basilar Artery, subdivided into type 3a, where the connection occurs with the Superior Cerebellar Artery (SCA), type 3b, the connection with the Anterior Inferior Cerebellar Artery (AICA), and type 3c, connecting with the Posterior Inferior Cerebellar Artery (PICA). In the presented case, the classification is Saltzman type 1 [6].
The course of the Persistent Primitive Trigeminal Artery can be lateral or medial depending on its relationship with the cavernous sinus. When it follows a lateral course, the PPTA runs posterolaterally to the trigeminal nerve roots. In the medial course, the PPTA courses posteromedially from its origin with an intra-sellar or trans-hypophyseal course. Due to its proximity to anatomical structures, neurovascular conflict or compression syndromes of cranial nerves, such as trigeminal neuralgia, oculomotor, trochlear, or abducens nerve palsy, may be part of the clinical presentation, as well as subarachnoid hemorrhage and cavernous sinus fistula, secondary to aneurysmal rupture associated with such pathology [7].
Although the prevalence of PPTA is considered rare, understanding its anatomy and possible correlation with vascular pathologies is of fundamental importance. Neglecting the existence of PPTA during para- and intrasellar neurosurgical procedures can cause serious and even fatal complications, as well as percutaneous procedures of the trigeminal ganglion [5].
The association between PPTA and concomitant intracranial aneurysms remains unclear, with some authors describing a prevalence of associated aneurysms ranging from 14 to 32% [4]. These aneurysms can be located in various vascular segments or related to the bifurcation of the PPTA with the Internal Carotid Artery (ICA). Aneurysms of the PPTA itself are less common [3]. In addition to the presence of PPTA, there may be various anatomical variations or vascular and cerebral anomalies such as fetal pattern of the posterior communicating artery (P-com), hypoplasia of the vertebral and basilar arteries, anterior Inferior Cerebellar Artery (AICA) duplication, absence of posterior Inferior Cerebellar Arteries (PICAs), vertebrobasilar insufficiency, PHACE syndrome, Moyamoya disease [2].
Among the treatment modalities for aneurysms related to PPTA, endovascular procedures such as coiling and stent-assisted coiling stand out [8]. Preserving the patency of PPTA during these procedures is crucial, as the perforating arteries originating from it play an essential role in the irrigation of the brainstem [4]. Therefore, in cases of aneurysms associated with PPTA, performing a detailed study of the arteries is imperative to prevent ischemia of the brainstem and cerebellum, especially when PPTA is the main source of supply for the distal vertebrobasilar system [9].
A presence of Persistent Trigeminal Artery represents the maintenance of one of the anastomoses between the carotid and vertebrobasilar systems present during fetal development. It can also be correlated with other vascular variations and anomalies, which can cause a variety of symptoms and complications. Anatomical knowledge and familiarity with various therapeutic modalities are essential for the proper management of patients with this condition.
Own financing.
Dantas Mageste Ferreira provided guidance at all stages of the research. Jéssica Aguilar da Silva, Lano de Sousa Moreira and Tarciano Costa Nascimento wrote the main manuscript text. Taianne Fiore Schumann, André Guimarães Soares, Fernando Miguel Resck Gadbem and Ítalo Guilherme Giarola de Freitas Mariano made tables and prepared figures. All authors reviewed the manuscript.