Background: 5-ALA is a prodrug used to selectively illuminate high-grade glioma (HGG) tissue intra-operatively and optimize resection. Here, we present some of the first preliminary results on resection rates, survival analysis, and adverse effects from a single Canadian center.
Methods: We included 52 HGG patients (median age 61 years, 27 male) operated on using 5-ALA between 2020-2023, and 37 patients (median age 68 years, 22 male) operated on using conventional white light surgery between 2017-2020 as a control group. We compared the extent of tumour resection across treatment groups by comparing preoperative and postoperative MRI volumes. We compared overall survival across groups using the Kaplan-Meier estimator and logrank test. Adverse effects of the drug were monitored during the post-operative stay.
Results: The gross total resection (GTR) rate was significantly higher in the 5-ALA group (60%) compared to the white light group (14%; difference between groups 46% [95% CI 29-36]; p < 0.001). While results trended towards greater overall survival for 5-ALA patients, we did not find a statistically significant difference compared to conventional white light surgery (p = 0.394). The median survival was 502 days and 370 days for the 5-ALA and white light groups, respectively. 5-ALA was well-tolerated in all patients, with no reported side effects.
Conclusion: Our results support previous evidence that 5-ALA is a valuable tool in improving resection rates for patients with HGG. Additionally, the safety profile of 5-ALA remains favorable. A larger cohort is necessary to validate whether these improved resection rates translate to longer overall survival.
Malignant gliomas make up around a quarter of primary brain tumours, with glioblastoma multiforme (GBM) being the most cancerous type. This specific subtype accounts for nearly half of all brain tumours [1], with an incidence of 4 per 100,000 persons in Canada (Brain Tumour Foundation of Canada, n.d.). Literature shows that without treatment, the projected 2-year survival rate for GBM in Canadian patients is 8.7% [2]. On the other hand, with maximal treatment, the median survival time is between 12 to 18 months [2]. Moreover, malignant gliomas also cause 174,000 fatalities and 238,000 new cases of brain tumours annually throughout the world [3]. These statistics demonstrate the importance of scientific advances in terms of management for patients with high-grade gliomas (HGG). To this day, there is no perfect treatment for HGG, but in the last years, many researchers have developed new techniques to optimize the therapeutic intervention for these patients. Standard treatment consists of surgical resection, if possible, followed by complementary methods such as radiotherapy and chemotherapy [1]. It is important to note that due to the tumour's infiltrative growth and the inability to remove it with a large safety margin, the success of this procedure is limited [4]. Maximal resection is difficult to accomplish in HGG infiltration zones due to the limited macroscopic differentiation between white matter and pathological tissue [5]. Lacroix, et al. [6] conducted a study which determined that resection of 98% or more of tumour volume is associated with a significant advantage in terms of survival, compared to resections of less than 98%. In this study, the median survival for patients who underwent a resection of 98% or more was 13 months, versus 8.8 months for the group of patients who had a resection of less than 98%. For such reasons, there is a need for new modalities to better the clinical outcome of malignant glioma treatment, through optimizing the surgical resection aspect of the patient’s care. Numerous novel treatment modalities are currently under analysis to respond to this particular need. In the last 2 decades, surgical approach to HGG changed with the introduction of awake craniotomy [7], tractography MRI combined with navigation [8], and lately with fluorescence-guided surgery (FGS) using 5-Aminolevulinic Acid (5-ALA) [9]. This last method consists of an oral administration prior to surgery of a solution which enables the intraoperative detection of indiscernible tumour tissue under violet- blue light that would not otherwise be visible under normal white light [10]. We are reporting the first case series from a single Canadian center using 5-ALA in HGG surgery.
Our objectives for this study consist of firstly assess the use of 5-ALA-FGS in improving resection identified by the number of patients achieving GTR (gross total resection) of contrast-enhancing tumours on early postoperative MRI, and residual tumour volume on early MRI, as compared to control patients from our center. Secondly, we aim to compare overall survival between patients operated on with FGS vs. the conventional method using white light. Finally, in order to meet our objectives, a type A retrospective design will be used for this study.
5-Aminolevulinic acid (5-ALA) and Protoporphyrin IX (PpIX) fundamentals: 5-ALA consists of a precursor molecule of phototoxic and fluorescent protoporphyrin IX (PpIX) of the heme biosynthetic pathway [1]. The metabolism of 5-ALA leads to the production of PpIX, which has fluorescent capabilities, secondary to excitement induced by filtered light, such as violet-blue light [11]. At the biochemical level, starting inside the mitochondria, ALA-synthase produces 5-ALA from succinyl coenzyme A and glycine. Subsequently, following the formation of 5-ALA and its release into the cytosol, eight molecules of the sort are then converted into one molecule of PpIX by a series of enzymatic processes. The selective accumulation of PpIX in malignant glioma cells is a crucial characteristic to its benefits in terms of diagnostic and therapeutic applications for the use of 5-ALA [1]. This demonstrates the utility of using 5-ALA as a neurological adjunct, in order to distinguish between neoplastic and normal brain tissues during tumour removal [11].
Fluorescence guided surgery (FGS): Fluorescence-guided surgery (FGS) with the use of 5-ALA has been a growing intraoperative technique over the past years, that permits the delineation of tumour tissue from the subcortical tissue during HGG resection [12]. It was first described and introduced in Germany in 1998 [13]. The goal of FGS is to increase overall and progression-free survival (PFS) while ensuring that no functional deficits or quality of life is sacrificed in the process [1]. Fluorescence imaging based on 5-ALA differs from all other fluorescence-based techniques in that its non-fluorescent precursor, rather than the fluorochrome, is administered to the patient. As a result of this identified difference, the 5-ALA based fluorescence permits a higher contrast, since there is no background fluorescence from the circulation or interstitial space.
According to the U.S. Food and Drug Administration (FDA) approval of 5-ALA for glioma surgery, the recommended usage to obtain the benefits of 5-ALA in FGS and HGG surgical resection, is to use 20 mg/kg body weight of 5-ALA, dissolved in 50 ml of water and given orally within two to four hours before to anaesthesia [14]. However, it was recently demonstrated that 5-ALA FGS may be performed more than 6 hours after the drug has been administered, with clinical outcomes that are broadly consistent with earlier literature data [12], As previously mentioned, the administration of the drug then leads to PpIX accumulation in glioma cells, enabling the surgeon to perform a rather optimal resection of the tumour while distinguishing pathological tissue from subcortical tissue [1] with the use of a device that emits violet-blue light who has the capability of exciting the PpIX biological marker [11] (Figure 1).
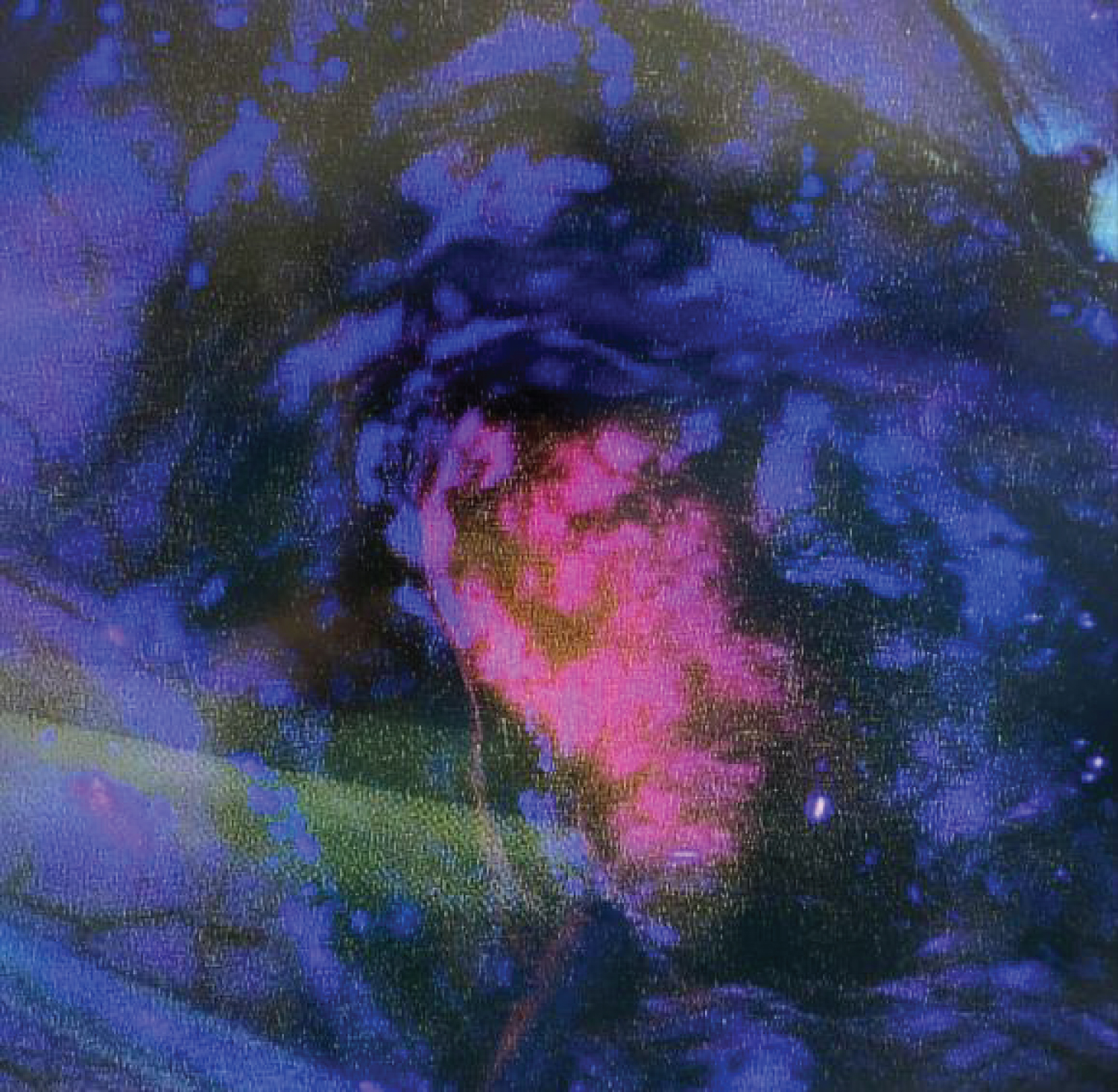 Figure 1: Per-operative view of the GBM in pink in contrast to non fluorescent surrounding brain parenchyma in blue.
View Figure 1
Figure 1: Per-operative view of the GBM in pink in contrast to non fluorescent surrounding brain parenchyma in blue.
View Figure 1
Applications and limitations of Ala-photodynamic therapy (ALA-PDT): 5-ALA uptake isn’t only applicable to HGG. The clinical and technical value of 5-ALA-induced fluorescence in stereotactic biopsies of intracranial lymphomas was demonstrated in a 2018 study. The study showed that for 41 patients with intracranial lymphoma, 75% of patients had the highest level of strong fluorescence, 4% had fluorescence that was slightly noticeable, and 21% had no fluorescence at all [15]. Another research also demonstrated positive fluorescence in 34 of 41 biopsies of primary central nervous system lymphoma, for a total of 82.9% [16]. Moreover, data from a study by Widhalm, et al. [17] showed that 85% of the World Health Organization (WHO) grade III gliomas in this investigation displayed localised fluorescence uptake. As for WHO grade II gliomas, 90% had no detectable fluorescence. Concerning meningiomas, Motekallemi, et al. [18] stated that both benign meningiomas (WHO grade I) and high-grade lesions meningiomas (WHO grades II and III) can exhibit tumour cell fluorescence. It was also mentioned that heterogenic fluorescence, which displays highly luminous and non-responsive regions within the same tumour, is a phenomenon associated with meningiomas [18].
In terms of limitations associated with 5-ALA use, the most frequent disease, pituitary adenomas, did not exhibit any intraoperative fluorescence in a study conducted by Micko, et al. [19].
As for metastatic brain tumours, a different type of fluorescence can be used. Brain metastases and skull base cancers were added as indications for fluorescence-guided surgery with fluorescein sodium in 2010 [20], this type of fluorescence will not be covered in this review.
History of gleolan (5-Ala): It was the pioneering 5-ALA multicentre randomised phase III study, directed by Dr. Walter Stummer in 2006, which revealed that surgeons utilising 5-ALA FGS as a surgical accompaniment could remove tumours in a more complete fashion for HGG patients and produce better patient outcomes than with standard surgery [21]. The study demonstrated that for the group of 139 patients with contrast-enhanced tumour resection by 5-ALA, 90 patients (65%) ended up with a completely resected tumour, while as for the control group, only 47 patients out of 131 (36%), had a complete tumour resection. Moreover, compared to patients who received white light, those who received 5-ALA showed a greater 6-month progression-free survival rate (41.0% vs. 21.1%; difference between groups 19.9%) [21]. Thus, with this addition to the literature, other researchers around the world started to investigate and analyze this revolutionary tool for intervention in HGG patients.
The European Medicines Agency (EMA) approved this new 5-ALA FGS method in 2007 (10). Over the following ten years, other works coming from Europe and other parts of the world looking at the usage of 5-ALA were published. Thereafter, in June of 2017, the United States FDA gave the approval for the usage of 5-ALA for HGG surgery [9]. Finally, on September 9 th , 2020, approval from Health Canada was given [22].
Cost and cost-effectiveness of gleolan (5-ALA): To facilitate the dosing and administration of Gleolan, a dose banding technique is used, that is, calculated doses within a certain weight range which are substituted to a predetermined dose. One or two vials (1500 to 3000 mg) are typically required for the dose. A vial is a dry powder of 1500 mg, which is then reconstituted with 50 ml of sterile water to a final concentration of 30 mg/ml. Gleolan is reconstituted on the unit immediately before it is administered to patients. Furthermore, the typical dose of 5-ALA (Gleolan) is 20 mg/kg, and is given 2 to 4 hours prior to surgery. Finally, in monetary terms, the cost of one vial is C$2,265.
Prior to 5-ALA surgery being accepted by the larger healthcare system in Canada, it was said to be essential to assess the cost-effectiveness of the procedure [23]. Recent research conducted by Warsi, et al. analyzed three studies in a systematic review format in order to evaluate the cost-effectiveness of 5-ALA in HGG surgery. In sum, despite the lack of high-quality data on the cost-effectiveness of 5-ALA, the information that is currently available points to this adjunct’s cost-effectiveness. The cost-utility of 5-ALA in comparison to white light was proven in two of the three studies (C$12,817 and C$13,508/QALY (Quality Adjusted Life Years)). One evaluated the cost-utility for a gross total resection (C$6, 813)). For each individual study, which were conducted in European countries, both of these numbers fell below the national cost- effectiveness standards. As for the third study, no significant difference was found for the cost of 5-ALA used in glioblastoma resection (C$14,732) compared to the previous therapeutic modality (C$15,936) [23]. Another study mentioned that for individuals with malignant gliomas, 5-ALA-guided surgery is thought to be more simple and less expensive than alternative procedures [24].
Benefits of 5-ALA use in HGG: In the last few decades, many researchers have been interested in studying the effects of FGS using 5-ALA to improve the therapeutic approach of HGG. It was with the research of Stummer, et al. [21] in 2006 that we really started to understand the benefits of the revolutionary intervention method for HGG. Stummer, et al. [21] analyzed data from a sample of 322 patients, which demonstrated that in patients with malignant gliomas, tumour fluorescence obtained from 5-ALA enabled more complete resections of tumours, thus improving PFS. Following this pioneering study, many other researchers added to the literature about this subject.
Firstly, it has been proven that 5-ALA FGS allows for the visual separation of malignant brain tumour tissues from white matter prior to the resection of the tumour during surgery, while providing a good quality of life and having minimal side effects [14], such as infrequent transient liver enzyme elevation and light sensitivity of the skin appearing 24 hours following administration [25]. In a recent systematic review regrouping 45 studies, resection of HGG with the use of 5-ALA for FGS was discovered to be linked to longer overall survival (OS) and PFS, as well as a larger degree of resection [26]. Furthermore, when it comes to real-time tumour viewing, excellent diagnostic accuracy, and minimum departure from the typical operating process for HGG excision, 5-ALA has unequivocally proven beneficial through the analysis of another systematic review [27]. In 2021, a meta-analysis also demonstrated that intraoperative imaging technologies such as FGS with 5-ALA could be beneficial in terms of maximizing HGG resection [28]. Also, it has been found that patients with malignant gliomas near or at the level of the eloquent areas of the brain may be treated with 5-ALA FGS without suffering from significant neurological deficits afterwards [21]. Moreover, a single-centre 7-year comparative effectiveness study using the Karnofsky Performance Scale, an assessment tool for functional impairment, showed that the use of FGS with 5-ALA did not worsen postoperative function in comparison to the conventional surgical method [29]. In addition, a study regrouping a systematic review and a meta-analysis, demonstrated that, in comparison to the phase III RCT conducted by Stummer, et al. in 2006, which reported a gross total resection (GTR) rate of 65%, the pooled analysis of 998 patients with HGG who underwent 5-ALA-guided surgical resection demonstrated a higher rate of GTR in the cohort of all patients with HGG (76%) as well as in the subgroup of patients with primary HGG (77%) [30]. As for the accuracy and medical diagnosis of 5-ALA FGS, a meta-analysis of the literature evoked a sensitivity of 82.6% (95% CI: 73.9-91.9, p < 0.001) and a specificity of 88.9% (95% CI: 83.9-93.9, p < 0.001) [31]. Another systematic review validated that 5-ALA can also, on top of all the other intraoperative and postoperative benefits, act as a radiosensitizer by stimulating oxidative stress in the mitochondria of malignant cells and increasing the host immune system response [32].
We conducted a literature review in order to identify a variety of articles discussing many subjects related to the area of research interest, such as 5-ALA fundamentals, FGS, the application and limitations of photodynamic therapy, the history behind the development of 5-ALA, the cost-effectiveness of the tool, as well as its benefits and clinical efficacy. All types of study designs conducted on 5-ALA-FGS in HGG surgery for patients of any age were included.
We retrieved English language studies from the PubMed database, and this, by searching with keywords consisting of “5-ALA”, “5-Aminolevulinic acid”, “high-grade glioma”, “malignant glioma”, and “fluorescence-guided surgery”. These keywords helped us retrieve all relevant full- text publications between 2000 and 2023, that is approximately 2000 articles. After analyzing the titles of all the articles, we selected the most pertinent ones to then analyze their abstracts. Subsequently, the reference lists of the identified articles were searched for additional literature published on the topic of interest. Finally, 33 articles were retained for the redaction of the literature review.
We retrospectively collected data for all patients operated on for suspected HGG between 2017 and 2023 at the Moncton Hospital (Horizon Health Network). Suspicion of HGG was based on pre-operative radiological findings. The 5-ALA group consisted of patients operated on since June 2020, after 5-ALA fluorescence-guided surgery had been approved in Canada and subsequently implemented at the Moncton Hospital. Our control (white light) group consisted of HGG patients operated on between May 2017 and June 2020 under white light and using conventional surgical techniques (prior to 5-ALA implementation). Patients were included in our analysis if their postoperative pathology report confirmed findings consistent with HGG (grade III/IV), as defined by the World Health Organization (WHO) [33]. Patients were excluded from our analysis if their postoperative pathology report described findings that excluded HGG (e.g., low-grade glioma, meningioma, lymphoma), or if the surgeon opted for biopsy instead of resection during the operation. Data characteristics we collected include tumour grade and classification, pre-operative and post-operative tumour volumes, age at the time of surgery, sex, survival status (alive or deceased), date of surgery, and date of death (if applicable).
5-ALA was given to patients 2 to 4 hours prior to surgery. The pharmacy department at the Moncton Hospital developed a dose banding protocol for the administration of 5-ALA. If the patient’s weight was between 40 kg and 84.9 kg, 1500 mg of Gleolan (one vial) was given once orally. If the patient’s weight was between 85 kg and 160 kg, 3000 mg was given once orally. If the patient’s weight was less than 40 kg or greater than 160 kg, 20 mg/kg rounded to the nearest 150 mg was given once orally. In all cases, the dose was prepared by adding 5 mL of sterile water for every 150 mg of Gleolan for a concentration of 30 mg/mL. Side effects were monitored over the course of the postoperative stay and recorded if notable.
In the post-operative stage, all patients from both groups received an extension of maintenance Temozolomide administered by the neuro oncologist. This postoperative adjuvant chemotherapy is backed by the Stupp protocol, which found that adding this medication to radiotherapy for newly diagnosed glioblastoma improved survival in a clinically and statistically significant manner [34].
We assessed the extent of tumour resection across treatment groups by comparing preoperative and postoperative contrast-enhancing tumour volumes on T1-weighted MRI. In all cases, postoperative scans were acquired no later than one day after surgery. Preoperative and postoperative volumes were calculated using the model proposed by Singhal, et al. [35], that is, a simplified tumour volume estimation from the linear dimensions of intracranial lesions. This model was proposed to be more accurate than the standard ellipsoid method for calculating tumour volumes from linear dimensions. Specifically, given the maximal anterioposterior (AP), medio-lateral (ML), and cranio-caudal (CC) diameters of the tumour, the volume of small tumours having the product of their diameters less than 2.5 cm 3 was calculated as 𝑉 = 0.513 × (𝐴𝑃 × 𝑀𝐿 × 𝐶𝐶) + 0.047, while the volume of all other larger tumours was calculated as 𝑉 = 0.444 × (𝐴𝑃 × 𝑀𝐿 × 𝐶𝐶) + 0.339 [35]. The three principal diameters for each tumour volume were recorded by a radiologist and extracted during our chart review. Gross total resection (GTR) was defined as an operative attempt in which the remaining residual tumour volume was less than 0.175 cm 3 , in keeping with the convention in Stummer, et al. [21]. The gross total resection rate for a particular treatment group was defined as the percentage of operations which resulted in gross total resection. Operations with a residual tumour volume greater than 0.175 cm 3 were classified as subtotal resection (STR).
Besides resection rates, we also compared survival and safety outcomes across treatment groups. Survival was measured as days alive since the date of each patient’s most recent surgery. Dates and survival status were collected up to May 2023, and any patients alive as of this date were treated as censored in our survival analysis. To assess drug tolerance and safety, we checked patient records for any signs of photosensitivity, elevated liver enzymes, nausea, vomiting, or hypotension as these have been described as potential side effects of 5-ALA in previous literature [36,37]. Any instances of these side effects were recorded in our chart review.
We used Pearson’s chi-squared test [38] to compare resection rates across treatment groups. The variables of the associated contingency table were treatment group (5-ALA vs. white light) and resection status (GTR vs. STR). p -values and confidence intervals for the chi- squared test were calculated using SPSS statistical software (IBM, Armonk, NY). The odds ratio was calculated based on the ratio of the odds of achieving gross total resection given surgery with 5-ALA to the odds of achieving gross total resection after white light surgery. The odds ratio was calculated using SPSS software. We compared the distributions of pre- and postoperative tumour volumes between 5-ALA and white light groups using the Mann-Whitney U -test [39], which is a nonparametric statistical test with fewer distributional assumptions compared to the Student’s t -test. We used the logrank test [40] to compare survival distributions between the 5-ALA and white light groups. Patients who were alive as of May 2, 2023, were treated as censored in this analysis. Mann-Whitney U and logrank tests were implemented using the SciPy ( SciPy , n.d.) and kaplan meier [41] open-source libraries for Python.
We included 52 patients operated on using 5-ALA FGS between 2020-2023 and confirmed to have a high-grade glioma (WHO grade III or IV) based on pathology reports of intra-operative specimens (Table 1). Twenty-three additional patients were operated on using 5-ALA surgery for suspected high-grade glioma on pre-operative MRI imaging, but were excluded either due to a confirmed non-high-grade glioma on pathological analysis (e.g., low-grade glioma, meningioma, lymphoma) or opting for biopsy as opposed to complete resection. Our retrospective chart review yielded 37 patients operated on using conventional white light surgery between 2017 and 2020, before our institution’s use of 5-ALA (Table 1). We compare these two groups (5-ALA and white-light) throughout the rest of the results.
Table 1: Baseline characteristics for included patients. View Table 1
5-ALA was well-tolerated in all patients-notably, none of our patients receiving 5-ALA exhibited side effects that have been associated with the drug including photosensitivity, elevation of liver enzymes, nausea, vomiting, or hypotension as compared to the literature [36,37]. As mentioned in the methods, all patients were monitored for side effects related to 5-ALA over the course of their postoperative stay.
The gross total resection (GTR) rate was significantly higher in the 5-ALA group (60%) compared to the white light group (14%; difference between groups 46% [95% CI 29-36]; p < 0.001; Figure 2a). The common odds ratio for GTR with 5-ALA compared to conventional white light surgery was 9.44 (95% CI 3.17-28.19). Preoperative tumour volumes were comparable across groups (p = 0.351; Figure 2b). Meanwhile, there was a significant difference in postoperative tumour volume across groups (p = 0.002; Figure 2b. The white light group had a median postoperative tumour volume of 1.3 cm 3 (range 0.0-18.7) compared to 0.0 (range 0.0-32.2) in the 5-ALA group. Notably, using conventional white light surgery, there were several more cases with a small amount of residual tumour left after resection (between 0-5 cm 3 ) than in the 5-ALA group (see Figure 2b, bottom).
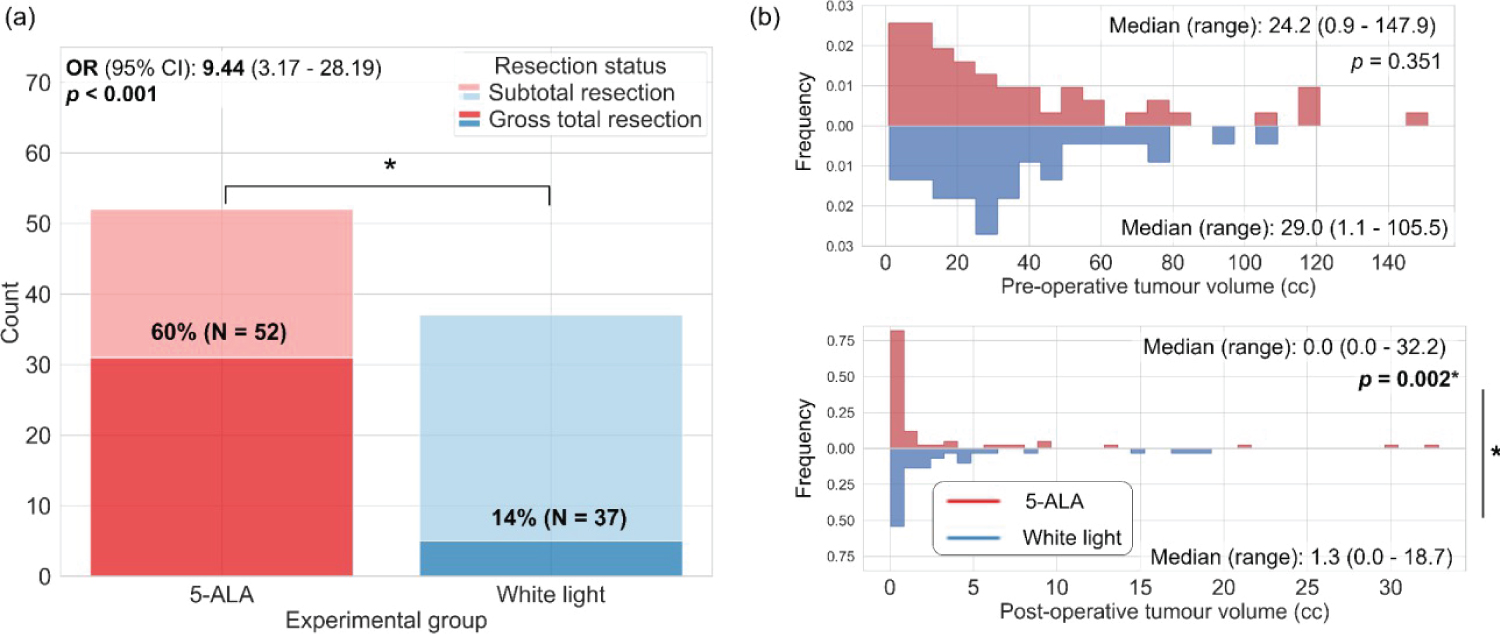 Figure 2: 5-ALA significantly improves GTR rates and median postoperative tumour volume compared to traditional white-light surgery. (a) Counts of patients achieving GTR in the 5-ALA group (red) vs. the white light group (blue) (p < 0.001; OR = 9.44 (3.17 - 28.19)); b) Preoperative (top) and postoperative (bottom) tumour volume distributions for the 5-ALA (red) and white light (blue) groups. The difference between postoperative tumour volumes across groups was significant (p = 0.002).
View Figure 2
Figure 2: 5-ALA significantly improves GTR rates and median postoperative tumour volume compared to traditional white-light surgery. (a) Counts of patients achieving GTR in the 5-ALA group (red) vs. the white light group (blue) (p < 0.001; OR = 9.44 (3.17 - 28.19)); b) Preoperative (top) and postoperative (bottom) tumour volume distributions for the 5-ALA (red) and white light (blue) groups. The difference between postoperative tumour volumes across groups was significant (p = 0.002).
View Figure 2
In our cohort, we were not able to find a statistically significant difference in survival benefit from 5-ALA compared to conventional white light surgery (p = 0.394; Figure 3), although we observed a slight trend towards longer survival in the 5-ALA group. In the 5-ALA group, the median survival was 502 days (95% CI 334-669; 26/52 patients censored) compared to 370 days (95% CI 192-548; 9/37 patients censored) in the white light group.
 Figure 3: Survival curves compared between 5-ALA (red) and white light (blue) groups.
View Figure 3
Figure 3: Survival curves compared between 5-ALA (red) and white light (blue) groups.
View Figure 3
In our study, we investigated the use of 5-Aminolevulinic Acid (5-ALA) fluorescence- guided surgery (FGS) in patients with high-grade gliomas (HGG) at a single Canadian center. Our main objectives were to assess the benefits of 5-ALA-FGS in terms of improving GTR rates and survival outcomes compared to conventional white light surgery, as well as to evaluate the safety profile of the product in terms of side effects. To put our findings into context, we will now compare our results with those of the literature, primarily focusing on the landmark study by Stummer, et al. [21].
Our study showed a significantly higher GTR rate in the 5-ALA group (60%) compared to conventional white light surgery (14%). This finding is consistent with the results reported by Stummer, et al. [21], where the GTR rate with 5-ALA-FGS was 65%, compared to 36% with conventional surgery. The higher GTR rate observed with 5-ALA-FGS in both studies highlights the efficacy of this technique in improving the extent of tumor removal during surgery.
A review of the literature further supports our findings, with several studies indicating that 5-ALA-FGS improves GTR in patients with HGG [1,11,30]. This benefit is crucial as achieving a higher rate of GTR has been associated with improved survival outcomes in patients with malignant gliomas [6]. Our study adds to the existing evidence, demonstrating the consistent effectiveness of 5-ALA-FGS in improving surgical outcomes.
While our study showed a trend towards longer survival in the 5-ALA group, we did not find a statistically significant difference in survival benefit between 5-ALA-FGS and conventional white light surgery. However, this finding may be influenced by factors such as the limited sample size and the relatively short follow-up period. To draw more definitive conclusions, larger studies with longer follow-up durations would be necessary.
When reviewing the literature, we found conflicting results regarding the impact of 5-ALA- FGS on overall survival [1,26,28]. Some studies reported a survival advantage with 5-ALA-FGS [21]. Stummer, et al. reported a greater 6-month progression-free survival rate in the 5-ALA group (41.0%) compared to the white light group (21.1%) [21]. On the other hand, other studies did not find a significant difference in survival outcomes when compared to conventional surgery [26,28]. The variation in results could be attributed to differences in patient populations, tumor characteristics, treatment modalities, and study designs.
Our study demonstrated that 5-ALA was well-tolerated in all patients, with no reported side effects. This finding aligns with the existing literature, which generally reports a favorable safety profile for 5-ALA [11,21,25]. The most commonly reported side effect of 5-ALA is photosensitivity, which typically resolves within 24 hours after drug administration [25]. Other side effects, such as nausea, vomiting, or hypotension, were not observed in our study or in most studies included in the literature review.
Our study has some limitations that should be acknowledged. First, the sample size is relatively small, and a larger cohort would provide more robust statistical power for survival analysis. Second, being a single-center study, our findings may not be fully generalizable to other centers or populations. In addition, there are many other factors that have the possibility to influence survival besides resection outcome, such as post-operative treatment regimen (chemotherapy, radiotherapy, etc.), lifestyle, etc. Furthermore, we compared across groups consisting of patients operated on in different years, which could be seen as a minor limitation or confounding factor.
Despite these limitations, our results are in line with the existing literature and provide valuable insights into the use of 5-ALA-FGS in HGG surgery at our Canadian center.
Overall, our study supports the growing body of evidence that 5-ALA-FGS is a valuable tool in improving surgical outcomes for patients with HGG. The higher GTR rate achieved with 5-ALA-FGS compared to conventional surgery can potentially lead to improved overall survival for patients. Additionally, the safety profile of 5-ALA remains favorable, with few reported side effects.
While our study contributes to the existing knowledge on 5-ALA-FGS, further research with larger sample sizes and longer follow-up periods is warranted to provide more robust evidence on its impact on survival outcomes. As 5-ALA-FGS continues to gain approval in different regions, it is essential for clinicians and researchers to collaborate and share their findings to optimize the clinical management of HGG patients. By combining evidence from different centers and countries, we can build a more comprehensive understanding of the benefits and limitations of this novel surgical approach.
The authors declare the study was carried out without any financial or commercial ties that might be viewed as a potential conflict of interest.
FL: Conceptualization, methodology, investigation, data curation, writing - original draft, writing - review & editing, visualization, project administration; LB: Conceptualization, methodology, formal analysis, data curation, writing- original draft, writing- review & editing, visualization; TN: Conceptualization, methodology, formal analysis, writing- original draft, writing- review & editing, visualization; JB: Investigation, resources, data curation; DC: Investigation, conceptualization, methodology, resources, project administration; MR: Investigation, resources, data curation; AEH: Conceptualization, methodology, investigation, resources, writing- original draft, writing- review & editing, visualization, supervision, project administration, funding acquisition.