Background: Symptomatic traumatic epidural hematoma (EDH) in a newborn is extremely rare. These injuries can occur for various reasons, such as prolonged labor, fetal distress, assisted delivery techniques such as forceps or vacuum extractors, or cesarean sections. Our literature research identified a total of fewer than 20 such patients with a skull fracture and underlying EDH, of which eight were treated with surgical decompression.
Case presentation: Here we report the case of one-day-old girl who was born at 37 weeks of gestation through urgent cesarean section under general anesthesia. Post-cesarian section, the infant was noted to have significant head deformity, hypotonia, and subgaleal fluid collection. Imaging showed a right parietal skull fracture with underlying EDH and midline shift. Symptoms continued to evolve with conservative management, so the infant was taken for surgical decompression and reconstruction of the skull fracture.
Conclusion: Cranial birth injuries can have a wide range of effects on the newborn, from minor bruises or swelling to more serious conditions like seizures, brain damage, or death. It is essential to seek immediate medical attention if you suspect a newborn has suffered a cranial birth injury. Infant EDH is an emergency and should be managed surgically when patients display poor neurologic status or when neuroimaging shows compression, a midline shift of at least 5 mm, or a hematoma larger than 2 cm.
Epidural hematoma, Skull fracture, Hypotonia, Brain compression
There is very limited literature on epidural hematomas (EDH) in newborns, as they are considered exceedingly rare, although this could be due to underdiagnosis [1]. Despite advances in obstetrics care, cranial trauma in the neonate remains a significant problem. Traumatic delivery is the principal cause of intracranial hemorrhage [2]. Excessive molding of the head in the birth canal during prolonged labor, breech delivery, and the use of forceps are commonly cited as the greatest risk factors [3].
Premature infants and full-term infants with low birth weight are at greater risk of intercranial hemorrhage [4].
The rate of hemorrhage is higher in infants who undergo instrumental delivery, which includes the use of vacuum assistance, forceps, or cesarian section during active labor [5]. Infants who undergo spontaneous delivery or cesarian section prior to the onset of labor have lower incidences of intracranial hemorrhage [5]. The source of EDH bleeding in newborns is usually venous given the anatomy of the neonatal skull and brain parenchyma [6]. Oftentimes, a concomitant skull fracture exists, which allows the EDH to communicate with an overlying hematoma [7]. The likelihood of EDH is evaluated based on the presence of risk factors, physical findings suggestive of injury, and the clinical manifestations of brain injury [8].
The rarity of these injuries makes it essential to review cases to better understand methods of diagnosis, management, and recovery. Currently, no consensus exists on best practices in the management of EDH in the neonate, as it is such a rare complication. Through our case review, we hope to provide guidance on the clinical manifestations of EDH and how to approach the decision to operate from a neurosurgical perspective.
We present a case of a one-day-old female newborn, born to a nulliparous woman at 37 weeks of gestation via cesarean section under general anesthesia. Delivery was complicated by pre-eclampsia with severe features, fetal intolerance to labor, and uterine fibroids. The neonate was noted to be small for gestational age with a head circumference and weight below the third percentile. Exam revealed significant posterior cranial molding, hypotonia, and subgaleal fluid collection. Her APGAR scores were 6 and 9 at one and five minutes, respectively. Initial hematocrit remained stable at 49% (RR 44.0-64.0%); however, the maximum diameter of the subgaleal fluid collection increased by one cm within the first hour of life.
An initial head ultrasound (Figure 1) suggested the possibility of an epidural or subdural hematoma. Subsequent brain CT scans (Figure 2) revealed a large right-sided parietal EDH with a maximum thickness of 1.8 cm, diffuse subarachnoid blood, effacement of the right lateral ventricle, and a 4 mm midline shift. A CT scan of the bony window (Figure 2) uncovered a complex right parietal skull fracture with a 3 mm inwardly displaced depression of the fracture.
 Figure 1: Transfontanellar ultrasound demonstrating intracranial bleed. (A) Coronal view; (B) Transverse view.
View Figure 1
Figure 1: Transfontanellar ultrasound demonstrating intracranial bleed. (A) Coronal view; (B) Transverse view.
View Figure 1
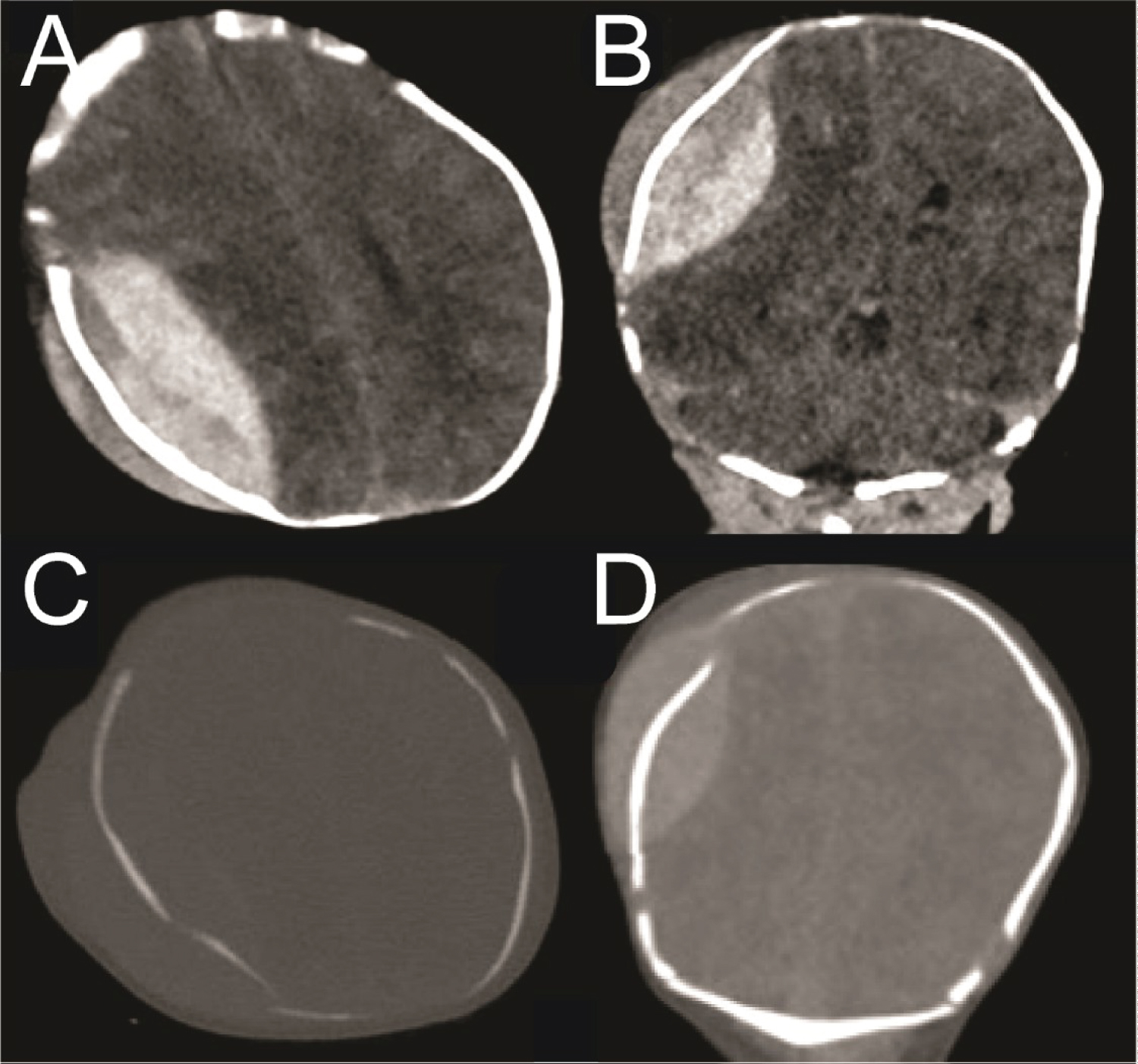 Figure 2: CT head with parietal EDH and skull fractures. (A) Axial view in the brain window demonstrating large EDH and overlying cephalohematoma; (B) Coronal view brain window showing the EDH; (C) Bony window of panel A; (D) Bony window of panel B.
View Figure 2
Figure 2: CT head with parietal EDH and skull fractures. (A) Axial view in the brain window demonstrating large EDH and overlying cephalohematoma; (B) Coronal view brain window showing the EDH; (C) Bony window of panel A; (D) Bony window of panel B.
View Figure 2
The neonate was then admitted to the Neonatal Intensive Care Unit (NICU) for careful monitoring. The following morning, her hematocrit had dropped to 39%. Exam revealed a full anterior fontanelle and abnormal movements, which were concerning for seizure activity in the setting of her known injury.
Neurology was consulted to facilitate continuous EEG monitoring. To better characterize the extent of the intracranial hemorrhage and limit radiation exposure, a Half-Fourier Acquisition Single-shot Turbo Spin Echo Magnetic Resonance Imaging (HASTE MRI) of the brain was performed. The results showed an expanded EDH, a 5 mm midline shift, and a trapped right ventricle (Figure 3). A repeat hematocrit returned at 32%.
 Figure 3: Pre-operative MRI brain HASTE protocol presented in T1 STIR. (A) Right parietal epidural hematoma, slightly increased in size from previous, with resultant mass effect on the right temporal and parietal lobes; (B) Trapped right ventricle with 5 mm midline shift; (B, C) Reduced diffusion along the bilateral temporal and parietal lobes with signal characteristics suggestive of subarachnoid hemorrhage.
View Figure 3
Figure 3: Pre-operative MRI brain HASTE protocol presented in T1 STIR. (A) Right parietal epidural hematoma, slightly increased in size from previous, with resultant mass effect on the right temporal and parietal lobes; (B) Trapped right ventricle with 5 mm midline shift; (B, C) Reduced diffusion along the bilateral temporal and parietal lobes with signal characteristics suggestive of subarachnoid hemorrhage.
View Figure 3
Given the progressive nature of the intracranial hemorrhage as demonstrated by the interval imaging changes, drop in hematocrit, full anterior fontanelle, and new seizure activity, the decision was made to perform an emergent craniotomy to evacuate the EDH. The neonate was positioned supine with her head tilted to the left using a small shoulder bump. During the procedure, a right parietal craniotomy was conducted, the EDH was evacuated, and the complex right parietal fracture was reconstructed. The surgery proceeded without complication, and she was successfully extubated and returned to the NICU.
The night following the operation, the infant had another seizure. It was uncertain if these seizures were transient and due to the recent surgical intervention or if they were a sign of permanent neurologic damage. However, on postoperative day 1, no further seizure activity was detected, and the neurology team felt it was safe to discontinue EEG monitoring. A follow-up HASTE MRI (Figure 4) confirmed successful hematoma evacuation, absence of residual clots, and improved midline shift. She continued to do well and was advanced to oral feeding. The surgical incision demonstrated satisfactory healing.
 Figure 4: Post-operative MRI brain HASTE protocol. (A, B) Axial views demonstrating adequate evacuation of the hematoma and improved midline shift.
View Figure 4
Figure 4: Post-operative MRI brain HASTE protocol. (A, B) Axial views demonstrating adequate evacuation of the hematoma and improved midline shift.
View Figure 4
She was discharged on postoperative day 5 and followed up in neurosurgery clinic three weeks post-operatively. The infant showed a remarkable recovery without any observed focal neurological deficits. Interval follow up for six months revealed no lasting neurologic deficits with the infant meeting all age-appropriate developmental milestones.
Epidural hematoma in neonates is a rare and potentially fatal result of injuries sustained during birth [9,10]. This case presents a complex clinical scenario of a newborn who had a significant intracranial injury after undergoing an emergent cesarean section complicated by uterine fibroids. The discussion provides an opportunity to highlight several key points that are important for clinical practice.
First, it underlines the potential risk factors for the development of EDH in neonates and subsequent workup. Neonatal EDH can be caused simply by the force from vaginal labor or by obstetric intervention that causes cranial damage [11,12]. Rapid vaginal delivery causes deformation of the skull and places neonates at risk for EDH. Similarly, during operative delivery, force placed on the skull by forceps, vacuum assistance devices, or physicians can precipitate EDH. Typically, infants are resistant to skull fractures due to a more elastic skull that can undergo deformation. However, EDH can still occur due to a highly vascularized diploic space in infants [13]. A review of 15 cases of EDH also suggests that parity may be a contributing risk factor, as most documented cases of EDH occurred following a difficult labor in a nulliparous woman [8]. Here, the nulliparous pregnant patient underwent cesarean section during active labor, an operation that was complicated by the presence uterine fibroids. These fibroids likely placed excessive force on the fetal skull, contributing to the development of EDH during an already high-risk cesarean section. After a careful literature review, it appears that this case is one of few, if not the only, documented case of EDH that occurred in the setting of uterine fibroids.
Shortly after birth, the patient in this case presented with significant head deformity, hypotonia, and a subgaleal hematoma, a constellation of symptoms which were suspicious for an intracranial bleed.
However, the presenting symptoms of EDH are often non-specific, such as seizure, anemia, apnea, and bradycardia [8,14]. The possible variations in presentation underscore the importance of early evaluation with neuroimaging. EDH is best characterized by CT or MRI because these modalities offer more accurate information about the hematoma [14]. In neonates, evaluation with CT must be weighed against the risk of exposure to radiation. In the case presented in this report, an initial transfontanellar ultrasound was suggestive of EDH, which CT later confirmed. After the infant was stabilized, MRI was used to clarify interval progression of the bleed. It is worth noting that postnatal transfontanellar ultrasound is standard of care for premature infants, infants who are small for gestational age, or those with other risk factors for intracranial hemorrhage [15].
At present, there is no consensus on optimal EDH management. Prior case reports have detailed spontaneous resolution of EDH in asymptomatic patients with blood collections of < 1 cm [16,17].
Conservative management can be appropriate when dealing simply with increased intracranial pressures, and in some instances, the continuity of the EDH with the overlying hematoma may facilitate resolution through hematoma aspiration [16]. However, cases with larger lesions, brain parenchyma compression, neurological impairment, and hemodynamic changes -as exhibited by this patient- warrant a more aggressive approach, such as craniotomy and hematoma evacuation [7,8].
Although these complications are not common, it is important for practitioners in the obstetrics and neonatal wards to pay special attention to infants who have undergone high-risk delivery. When EDH is properly identified, the mortality rate is exceedingly low [14]. If any concern for evolving intracranial pathology exists, parents and practitioners should not hesitate to seek neurosurgical consultation. Infant EDH is an emergency and should be managed surgically when patients display poor neurologic status or when neuroimaging shows compression, a midline shift of at least 5 mm, or a hematoma larger than 2 cm. This case study emphasizes the pivotal importance of surgical intervention in the successful management of severe EDH and how vigilant care minimizes complications. We encourage continued reporting and publication of cranial trauma sustained during birth so that the medical community can gain further insight into precipitating factors, possible presentations, and management practices.
The authors of this paper have no conflicts of interest or financial disclosures to report.