Rightsided traumatic diaphragmatic ruptures (RTDR) are rare. We report on a case of a two-stage detected RTDR after a quad accident.
A 30-year-old healthy man was brought to our level-one trauma center after a high-velocity trauma. While riding a quad he was hit by a car with about 60 km/h. Initial scores of Glasgow Coma Scale (GCS) and injury severity score (ISS) were 15. Extremity trauma with moderate craniocerebral injury and abdominal trauma with splenic and hepatic laceration was diagnosed. During follow up on the intensive care unit (ICU) the patient reported unspecific abdominal pain and dyspnea. Sonographic controls of the thorax and abdomen showed a hemothorax and dilated intestinal loops. We therefore performed a re-computer tomography re-(CT) scan, which showed an ileus and a RTDR. After immediate laparotomy, suture of the diaphragm and partial ileus resection the patient was rehabilitated and discharged at day 34 post trauma.
Acute two-stage detected traumatic right diaphragm ruptures after blunt high-velocity trauma are rare and difficult to diagnose. As they are associated with high mortality rates, even in case of unspecific clinical signs like abdominal pain exacerbation and dyspnea, sonographic controls of the thorax are recommended regularly and a multi-detector re-CT scan should be considered generously. Further thoracic x-rays may give hints like a raise of the diaphragm, liver herniation and lung atelectasis.
Right diaphragm rupture, High-velocity trauma, Blunt trauma
About 0.8%-5.6% of high velocity blunt thoraco-abdominal trauma is associated with diaphragmatic ruptures and about 14-18% of these are detected delayed after more than 48 hours [1-3]. Rightsided traumatic diaphragmatic ruptures (RTDRs) are even less common after blunt thoraco-abdominal trauma (< 0.01%) [2]. They are associated with higher mortality and require more urgent surgical correction [4]. The initial rupture is caused by a raised intraabdominal pressure forcing the abdominal organs towards the anatomical borders of the abdomen. Furthermore, stretching of the diaphragm during expiration causes further trauma to the muscle fibers and leads to a delayed diaphragmatic rupture with clinical relevance [1,5]. As clinical examination during acute phase can hardly contribute to the diagnosis (7-66%) multi-detector CT scan is the gold standard for diagnosis [6]. Sonographic controls of the thorax and abdomen can help to find RTDR [7,8]. We report a rare case of a two-stage detected RTDR which could not be seen in the initial multi-detector CT scan after a quad accident.
A 30-year old healthy man was brought to our level-one trauma center after high-velocity trauma. While riding a quad he was hit by a car with about 60 km/h. Informed Consent was given by the patient. Initial values of both, the Glasgow Coma Scale (GCS) and the Injury Severity Score (ISS) were 15, hemoglobin level was 14.5 g/dl, lactate 2.8 mmol/l and except an aspartate aminotransferase of 100 U/l all other laboratory exams were within reference ranges. Primary clinical examination, initial x-ray and trauma-computer tomography-scan showed a complex abdominal trauma with a splenic and hepatic laceration; however, neither signs of RTDR nor a jejunal ischemia could be observed at that time. Furthermore, an extremity trauma with additional moderate craniocerebral injury was diagnosed (Table 1). After the initial diagnostic procedures and operative stabilization of the extremity fractures the patient was transferred to the intensive care unit (ICU) for further treatment. The splenic and hepatic lacerations needed no emergency operative care as the patient was hemodynamically stable. During the following two days laboratory values stayed within range (Table 2). Although the patient constantly complained about moderate abdominal pain with an intensity of 4/10 on the visual analog scale (VAS), the abdominal tension was smooth and constant gut sounds were audible. No catecholamines were needed. On the second posttraumatic day, due to a pain exacerbation (VAS 7/10) we performed an abdominal sonography, which showed dilated intestinal loops and a pleural effusion on the right side however radiologically no intrathoracic sign for pneumothorax or clear diaphragm rupture could be observed. Especially comparted to the initial x-ray no clear sign for RTDR was detectable. Gut sounds were reduced. Therefore, we immediately performed an abdominal multi-detector re-CT-scan, which then showed a RTDR and a paralytic ileus. Based on these findings we initiated an urgent open laparotomy. Intraoperatively the diaphragmatic rupture could be confirmed and was treated by direct suture with a PDS-I-CTX wire by our abdominal surgeons. Furthermore, the evaluation of the small bowl revealed a subacute ischemic damage with necrotic jejunal loops due to a partial rupture of the meso, which necessitated partial resection. Due to the lack of any sign for loop perforation or peritonitis the abdomen was closed primarily. The iatrogenic right-sided pneumothorax as a result of the communication between peritoneum and thorax was sufficiently relieved with a chest drain. Postoperatively, the patient was transferred back to the ICU, was extubated 5:46 hours postoperatively without any catecholamine and stayed there for further six days (total 10 days). The further clinical course on the ICU was uneventful, so the patient could be transferred to the normal ward, where further extremity surgery was performed delayed due to acute trauma load without any complication (Table 2). He could be discharged on day 34 after prolonged mobilization.
Table 1: Overview of diagnosis and treatment. View Table 1
Table 2: Timeline of important blood parameters. View Table 2
After blunt abdominal trauma, diaphragmatic ruptures (DR) are rare and during explorative surgery only 3%-8% of the RTDR need to be treated. Out of all traumatic diaphragm ruptures, left-sided diaphragmatic ruptures are the most common with an incidence up to 65-75% [2,9]. Right-sided DRs can be observed in 22-39% however they are unusual as the liver protects the diaphragm and spreads the impact power above a larger surface than on the left side [2,10]. A further reason is, that on the left side the diaphragm is congenitally weaker than on the right side as a result of weakness during embryological fusion [11,12]. However, if herniation occurs it often leads to liver incarcerations causing abdominal pain and respiratory compromise potentially leading to strangulation with an associated high mortality rate up to 30%-60% [10,13]. The two-stage detected rupture of the diaphragm is probably caused by a necrosis of the diaphragmatic muscle fibers leading to a herniation of the liver. The liver herniation is a situation observed in delayed RTDR [1]. In our patient, the diaphragmatic herniation occurred at the same time the ileus was diagnosed. Both separate diagnosis demonstrated with separate clinical signs. Diagnostic marks for I) RTDR are the pain exacerbation, dyspnea, lactate rise and pleural effusion and II) for the ileus we observed the loss of gut sounds, pain exacerbation, sonographic dilatation of the intestinal loops, due to a partial rupture of the meso, lactate rise and a dilatation of intestinal loops in the subsequently performed multi-detector re-CT scan. Although the clinical signs like pain exacerbation, dyspnea, sonographic thoracic effusion and dilatated intestinal loops gave hints for the definitive diagnosis only the multi-detector re-CT scan was able to proof the correct diagnosis. The significance of the clinical examination is discussed controversially in the literature from limited- to best-tool [3,6,14]. Especially in this patient the course of pain and physical complains was a useful parameter for detection of RTDR.
It is interesting that the DR with herniation occurred at the same time as the ileus. We assume that the initially damaged diaphragm became a clinically relevant rupture due to the underperfusion and raised intraabdominal pressure as a consequence of the ileus. In both situations, a diagnostic laparoscopy and/or diagnostic laparotomy is recommended [10]. In isolated left-sided DR a laparoscopy is recommended, in right-sided DR either a laparoscopy and/or a thoracoscopy is recommended [1]. As CO2 inflation would have further raised the intraabdominal pressure and worsened the clinical situation, we decided to perform a laparotomy instead of a laparoscopy. Retrospectively we need to ask if any radiographic sign could have been detected earlier. In CT scans initially missed DRs range from 12-63% with a sensitivity of 87% and a speciticity of 72-100% [6,13]. A multi detector CT scan was used initially with a slice thickness of 1.2 mm. Although this type of CT scan is a better diagnostic examination than clinical examination (7-66% sensitivity) and x-ray (40% sensitivity), the initial CT scan in our case showed to the best of our knowledge no clear sign of DR [2,3,6]. Direct, indirect and signs of uncertain origin are described and classified for the CT scan [13]. The combination of signs has a sensitivity of 60-100% [3]. Direct signs for diaphragm rupture are direct discontinuity or dangling diaphragm sign [3,13]. Indirect signs are collar sign, intrathoracic herniation of viscera, dependent viscera sign, contiguous injury on either side of diaphragm and sinus cut-off sign [13]. Further signs of uncertain origin are thickening of the diaphragm, hypoattenuated diaphragm, fractured rip, diaphragmatic/peridiaphragmatic contrast extravasation [13]. Although the discontinuous sign has a good sensitivity of 73-82% and a good specific of 88-90% it is more difficult to be detected on the right side than on the left side due to the isoattenuation of the liver in the CT [3,13]. Neither the dependent viscera sign, nor the dangling-diaphragm sign were observed in the initial CT scan. Whereas the dependent viscera sign has only poor sensitivity (0%) the dangling-diaphragm sign is believed to be a reliable sign with 54% sensitivity and 98% specificity [3,13]. The organ herniation has a sensitivity of 55-81% and a specificity of 94-100% and could be observed in the re-CT-scan after clinical exacerbation with clear radiographic sign of discontinuous diaphragm and a liver herniation and furthermore a hemothorax on the right side which retrospectively can be correlated with the sonographic pleural effusion [13]. Therefore, we conclude that in this rare case of two stage detected RTDR after high velocity blunt trauma the longitudinal clinical examination is the first and most important diagnostic tool for detection of DR especially in cases of late onset. Thoraco-abdominal sonography can give indirect and direct signs for RTDR, however the multi-detector CT scan is the gold standard for diagnosis and a re-CT scan should be performed generously [7,13]. A hemothorax should be considered as an indirect sign for potential DR [7]. If either the clinical situation or the CT scan stays unclear an early diagnostic laparotomy, but not laparoscopy can prevent further harm.
Two-stage traumatic right diaphragm ruptures after blunt high-velocity trauma are rare however if they are missed, they are associated with a high mortality rate. Clinical signs are often unspecific with abdominal pain exacerbation and dyspnea. Initial laboratory values like hemoglobin level and lactate appear to stay within range. After initial trauma CT scan, we recommend at least daily sonographic controls of the thorax and abdomen in order to detect signs of hemothorax and free abdominal air or fluid. Further thoracic x-rays may give hints like a raise of the diaphragm, liver herniation and atelectasis (Figure 1).
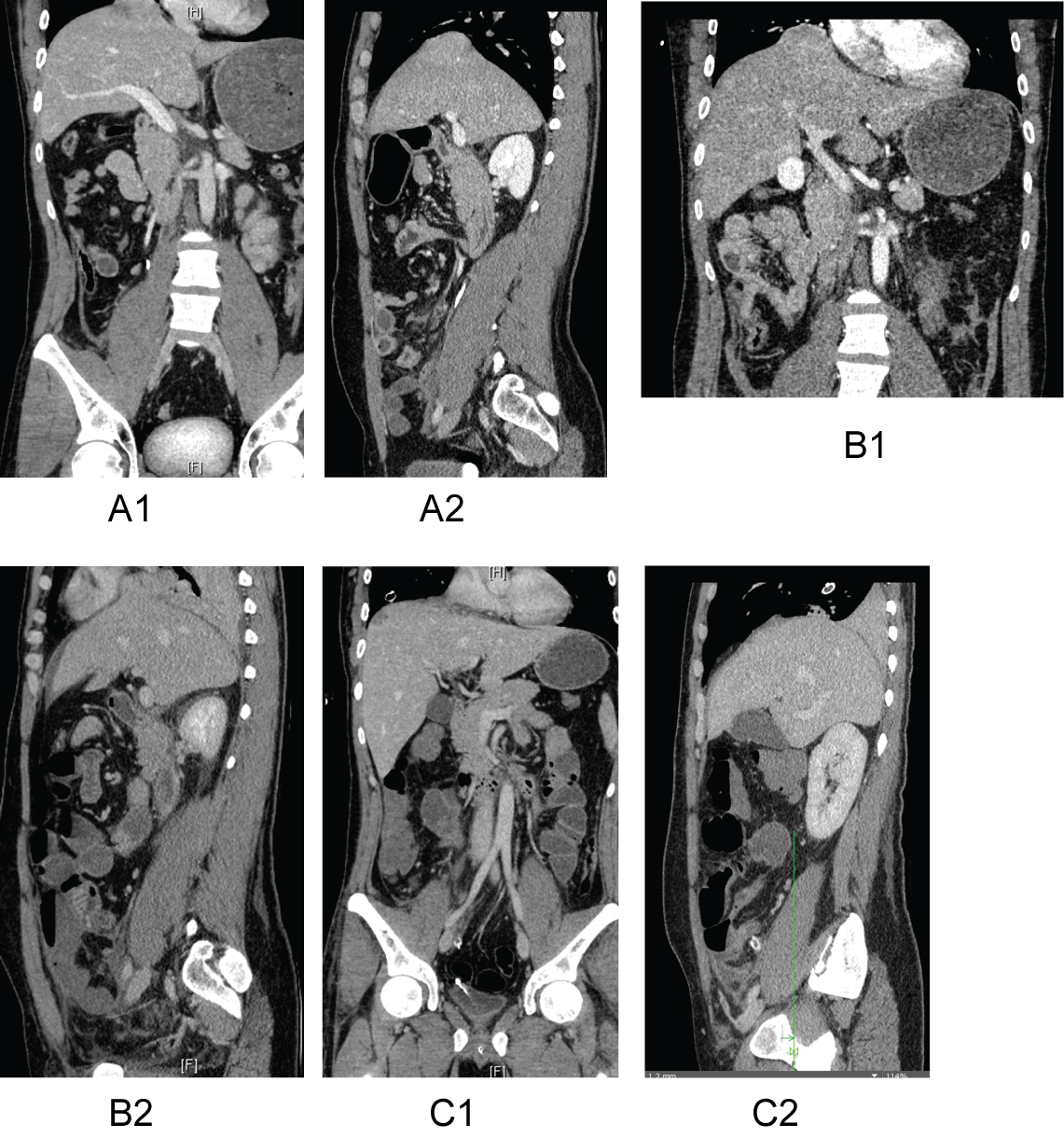 Figure 1: A1 and A2) Initial trauma CT scan with no clear evidence for RTDR although retrospectively one could have suspected a beginning rupture. B1 and B2) After two days, a distinct rupture of the right-side diaphragm could be observed. Coronal and sagittal sections show a liver herniation through the diaphragm into the thorax. C1 and C2) After operative treatment with suture of the diaphragm, no rupture and residual no herniation of the liver can be observed.
View Figure 1
Figure 1: A1 and A2) Initial trauma CT scan with no clear evidence for RTDR although retrospectively one could have suspected a beginning rupture. B1 and B2) After two days, a distinct rupture of the right-side diaphragm could be observed. Coronal and sagittal sections show a liver herniation through the diaphragm into the thorax. C1 and C2) After operative treatment with suture of the diaphragm, no rupture and residual no herniation of the liver can be observed.
View Figure 1
The study was not funded.
All authors declare that they have no conflict of interest.