Tongue-type fractures are unusual calcaneal fractures that produce an unique and relatively uncommon injury pattern to the bone and soft tissues, due to the separation of the calcaneal tuberosity into superior and inferior fragments. The displacement of the superior fragment has the potential to tent the skin of the posterior heel and, if not treated emergently, partial or full-thickness skin breakdown can progress quickly, and potential necrosis can occur. Early recognition by the emergency physician and prompt operative repair prevent further injury and obviate the need for surgical soft tissue coverage or potential amputation. Although this type of fracture is often associated to high-energy injuries in younger individuals, we present a case of a 62-year-old female with tongue-type calcaneal fracture due to minor trauma.
Tongue-type fracture, Calcaneal fracture
Calcaneus fractures represent 60% of all tarsal bone fractures and 2% of all fractures [1-4]. They are the most commonly diagnosed tarsal bone fractures in emergency medicine [3]. Approximately, 75% of calcaneal fractures are intraarticular [4]. One of the morphological variants of calcaneal fractures is the tongue-type fracture, which represents an unique an relatively uncommon injury pattern to the bone and soft tissues [2]. Tongue-type calcaneus fractures (TTCF) make up 25-35% of intraarticular calcaneal fractures [2].
TTCF is characterized by a secondary fracture line exiting posteriorly through the calcaneal tuberosity in continuity with some or all of the posterior facet, causing the separation of the calcaneal tuberosity into superior and inferior fragments [3,5,6]. The superior fragment is often displaced posteriorly and superiorly to varying degrees, because of the insertion of the Achilles tendon and consequent pull motion of the triceps surae complex [2,3,5]. Plantarflexion of this tongue piece can lead to increased pressure of the soft tissues overlying this fragment, what can compromise their blood supply and result in catastrophic secondary soft tissue lesion [2,5,6].
The typical mechanism of injury in younger individuals is a high-energy injury with an axial load applied to the heel [2,3,5]. This results in the lateral process of the talus being driven into the calcaneus, which, depending on the position of the subtalar joint, may result in a TTCF (or a depressed variant) [2-5]. Nevertheless, TTCF can also occur after relatively minor trauma in patients with compromised bone quality [2,3,5].
Radiographs are typically the initial method of investigation [2]. The management of TTCF is distinctly different from other calcaneal fractures, as urgent surgery may be required [1,2].
The authors describe the case of a 62-year-old female who was admitted to the Emergency Department due to a left foot injury. She was medicated for high blood pressure and dyslipidemia, and had previous medical history of left mastectomy due to breast carcinoma and right hemicolectomy due to intestinal adenocarcinoma - both in remission for more than 5 years).
The patient was walking on the street when she stepped into a manhole cover with her left foot, unaware that the cover was partially loose. The heel stayed partially positioned on the sidewalk, whereas the rest of the foot (firmly placed towards the center of the cover) followed the cover's movement as it gave up a few centimeters. This caused the distal part of the foot to undergo a downward axial movement, while the more posterior region of the heel (corresponding to the calcaneal tuberosity area) remained supported on the floor, therefore leading to a displacement of both mid- and forefoot areas relatively to hindfoot.
The patient felt and immediate acute pain and incapacity, falling to the ground. Due to open wound in the posterior region of the heel and inability of baring weight and walking, the patient seek help in the nearest hospital.
Physical examination revealed swelling and ecchymosis around the entire hind- and midfoot, with an abrasion wound in the posterior area of the heel. The postero-lateral bony prominence of the calcaneal tuberosity was palpable. Active and passive movements of the ankle joint were limited due to the swelling and pain, but motion of the toes did not cause pain. The patient denied sensory alterations on the toes and on the dorsal and plantar side of the foot. Arterial pulses were present.
X-rays were obtained and showed a tongue-type calcaneus fracture with significant superior displacement that was prominent posteriorly towards the skin posteriorly, causing significant soft tissue tension and leading to impinging on the anterior portion of the insertion of the Achilles tendon (Figure 1).
 Figure 1: Pre op X-ray (lateral view), at admission, showing a tongue-type calcaneal fracture with displacement of the superior bony fragment. View Figure 1
Figure 1: Pre op X-ray (lateral view), at admission, showing a tongue-type calcaneal fracture with displacement of the superior bony fragment. View Figure 1
On the same day, open reduction and internal fixation with three partially threaded cannulated screws were performed (Figure 2).
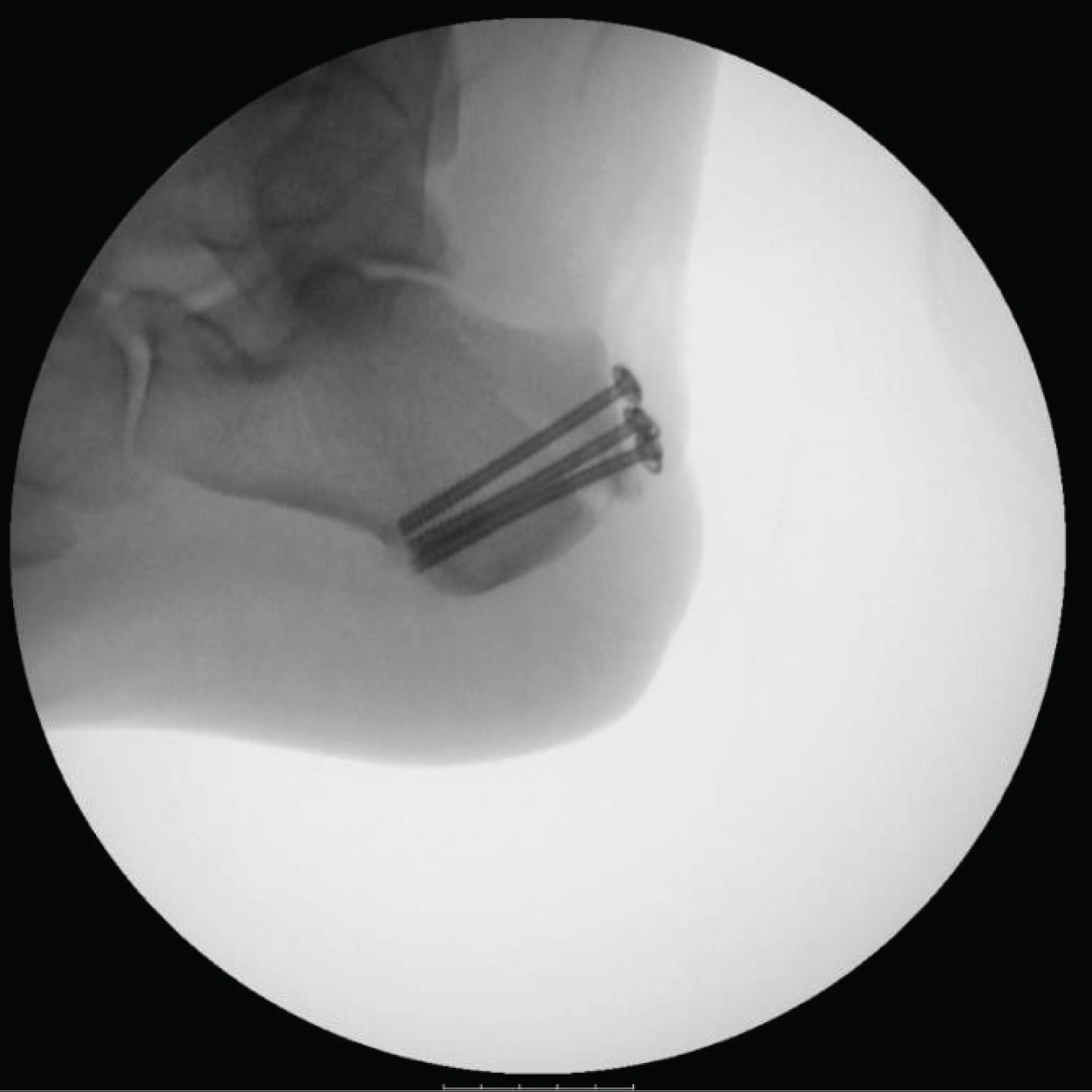 Figure 2: C arm X-ray showing fracture fixation. View Figure 2
Figure 2: C arm X-ray showing fracture fixation. View Figure 2
The pain was successfully managed with analgesics. A cast immobilization of the ankle was maintained for 9 weeks with concomitant thromboprophylaxis with enoxaparin (Figure 3).
 Figure 3: Lateral X-ray after 9 weeks of cast immobilization. View Figure 3
Figure 3: Lateral X-ray after 9 weeks of cast immobilization. View Figure 3
After cast removal, the patient was evaluated at the Physical Medicine and Rehabilitation Department and was integrated in a rehabilitation program with indication for progressing weight bearing ambulation as tolerated. Currently, 3 months after the injury, the patient has painless full range of motion of tibiotarsal and subtalar joints and she is able to walk slowly without aids. The posterior heel skin is healed, with some minor hypoesthesia and discomfort to palpation around the surgical incision scar area. Neurovascular examination of the foot is normal (Figure 4).
 Figure 4: Clinical picture of the foot and ankle 3 months after surgery, showing cutaneous integrity of the posterior skin and 90 degrees active dorsiflexion of the ankle. View Figure 4
Figure 4: Clinical picture of the foot and ankle 3 months after surgery, showing cutaneous integrity of the posterior skin and 90 degrees active dorsiflexion of the ankle. View Figure 4
Unlike our case, TTCF typically occur in younger individuals (average age of 40-years-old) and are nearly four times more likely in males [1]. The mechanism is usually a high-energy injury with an associated axial load applied to the foot, driving the lateral process of the talus into the calcaneus [1]. Depending on the position of the subtalar joint, it may result in a TTCF or a depressed variant.1 Nevertheless, TTCF can also occur due to a low-energy injury in the more elderly population [1]. In this case, the mechanism usually is a sudden dorsiflexion force to the foot, which leads to eccentric contraction of the Achilles tendon, resulting in an avulsion of the posterosuperior calcaneus [1,7]. Several studies have suggested an osteoporotic origin to these fractures [7].
Essex-Lopresti divided calcaneus fractures into two categories: Joint depression type and tongue type [1,2]. The two patterns share a common primary fracture line and are distinguished from each other based on a secondary fracture line [1,2]. When a tongue-type fracture results, the secondary fracture line propagates longitudinally and exits posteriorly from the calcaneal tuberosity, below the level of the Achilles tendon insertion [2,5]. Some studies refer that these fractures may be related to chronic tightness of the triceps surae or to a wider and broader insertion of the Achilles tendon [5,7]. Gardner, et al. further characterized TTCF as complete articular, in which the entire posterior facet articular surface is attached to the posterior tuberosity fragment; or partial articular, in which the fracture line traverses the posterior facet [2]. The resulting fracture pattern after hindfoot impact may be related to the direction of the applied force [5].
Radiographs are typically the initial method of investigation for suspected calcaneal fracture [2]. The views typically obtained include lateral and axial (Harris) views of the heel, as well as anteroposterior and oblique views of the foot to evaluate the calcaneo-cuboid joint [2]. The findings of a TTCF are best appreciated on the lateral view, and typically include a fracture line that extends horizontally from the angle of Gissane or the posterior facet of the subtalar joint to the posterior calcaneal surface, inferior to the Achilles insertion [2]. Computed tomography (CT) allows better visualization of the subtalar joint, and can provide an improved assessment of fracture pattern and injuries and determine if the fracture is complete or partial articular [2]. CT also gives improved visualization of the surrounding soft tissues compared to X-ray, and may show tendon entrapment or dislocation [2]. Radiologists should describe the posterior fracture fragment with care taken to describe where the anterior fracture line exits relative to the posterior facet and where the posterior fracture line extends relative to the insertion of the Achilles tendon [2].
The simplicity of the Essex-Lopresti classification, which relies solely on plain film X-rays (specifically the lateral X-ray), makes it an extremely useful classification in the emergency department, assisting the emergency physician to determinate how to acutely manage the fracture [1]. A tongue-type pattern inherently implies impending or associated soft tissue injury in a unique way that other classifications systems do not [1].
TTCF generally result in a separation of the posterior calcaneus into superior and inferior fragments [2]. The superior fragment inherently has a large deforming force as the Achilles tendon inserts onto the calcaneal tuberosity and displaces it posterosuperiorly to a varying degree [1,2,5]. This displacement pattern has the potential to tent the skin of the posterior heel, due to the thin layer of soft tissue and superficial nature of the fracture, and place it under significant tension [1-3,5]. On clinical evaluation, this particular area should be quickly and carefully inspected, as blanching of the skin is a sign of increased pressure that is limiting the vascular supply to the overlying skin [1,2,7]. In this case, if not treated emergently in a matter of hours, partial or full-thickness skin breakdown can progress quickly, and potential necrosis can occur [1-3,5,7].
Tongue-type fractures that are not tenting the skin or causing blanching may be splinted in plantarflexion to neutralize the force of the Achilles, and meticulous care should be taken to offload the posterior calcaneus and minimize pressure to the posterior skin [1-3,5]. A cast window can allow for easy clinical evaluation of the posterior skin [2,5]. Then subsequently they may undergo non-urgent surgical percutaneous pin fixation or open reduction and internal fixation from a lateral approach, with plate and screw fixation, once the soft tissues are amenable [2].
The tongue fragment is frequently in a position of valgus, adduction, and plantarflexion [6]. Using either a supplementary pin laterally for axial and coronal correction or by placing a varus/abduction moment through pins placed posteriorly into the tongue fragment, may aid in achieving a successful closed reduction [6].
On the other hand, urgent fracture reduction should be performed as soon as clinical signs of soft tissue compromise become evident [5]. Unfortunately, skin compromise complicates a large percentage of TTCF, namely the ones caused by non-fall mechanism and the ones with greater displacement of the fracture segment [3]. An emergent orthopedic consultation is necessary to proceed to an open reduction to relieve the tension and to perform an internal fixation to minimize soft tissue devitalization [1,3,5,7]. In these patients, further soft tissue intervention can be avoided through early reduction and immobilization [3]. The reconstruction of soft tissue defects in this region represents a challenge for plastic surgeons because of the limited local soft tissue availability to obtain a good functional outcome [2].
A delay or error in diagnosis and treatment can result in a closed fracture becoming an open fracture which can lead to increased patient morbidity [2]. Early recognition by the emergency physician and prompt operative repair prevent further injury and obviate the need for surgical soft tissue coverage or potential amputation [3].
On follow up imaging, the hardware should be evaluated for fracture or adjacent lucency which may be seen with loosening [2]. In addition, the fracture fragment alignment should be evaluated for change in position, which indicates refracture [2].
Tongue-type fractures are unusual calcaneal fractures in which the displacement of a bony fragment has the potential to tent the skin of the posterior heel. Although they are often associated to high-energy injuries in younger individuals, this type of fracture can also occur due to minor trauma. Early recognition by the emergency physician and prompt operative repair is necessary to prevent further complications.
All authors contributed equally to this work.