Since the first description of the cross-finger flap in 1950 for finger injury defect cover, over the last 70 years it has been tremendously explored and has underwent innumerable refinements and modifications. Whether used alone or in combination with other flaps for the reconstruction of finger defects, traumatic or non-traumatic, cross finger flap has proven its worth as a workhorse for finger reconstruction. Despite a handful of innate disadvantages, it has given excellent sensory, functional, and aesthetic outcomes in vast majority of studies. This article has been an attempt to reveal the entire rich journey and inexhaustible history of cross finger flap. With such a grandiose potential, it only seems that the cross finger flap will be continuously evolving over time and keep serving mankind in better ways.
Cross-finger flap, Fingertip reconstruction, Finger injuries, Transdigital flap, Heterodigital flap
Critical defects of fingers with exposed tendon, bone or joint warrants early soft tissue cover. Over time, innumerable techniques have been described for reconstruction of various finger injuries and deformities. Among all of them the journey of "the cross finger flap" has been most consistent and rich. It is doubtful whether any other finger injury reconstruction modality had been explored to this extent and so many modifications introduced, as has been the cross finger flap. This article is an attempt to make us aware of the vast plethora of finger defects that have been successfully managed by cross finger flap, and have this flap as a valuable addition in our armamentarium for various finger reconstructions.
PubMed [MEDLINE] database was searched on August 2020 using the MeSH terms: "cross finger flap [MeSH Terms] OR heterodigital flap [MeSH Terms] OR transdigital flap [MeSH Terms] AND finger [MeSH Terms] OR thumb [MeSH Terms] OR finger injuries [MeSH Terms] OR finger amputations [MeSH Terms] AND reconstruction [MeSH Terms]". Studies were limited to human, published in English language between 1946 to 2020. The titles and abstract were reviewed manually to identify appropriate studies. In cases of unclarity, full text was reviewed. References of appropriate articles were also screened to identify additional related studies not obtained from original search. Pre-determined inclusion and exclusion criteria (Table 1) were applied to the search result to identify relevant citations.
Table 1: Inclusion and Exclusion Criteria. View Table 1
The PubMed search produced 1926 results. After title and abstract review of primary search and references, and applying the inclusion/exclusion criteria, 76 citations were identified (Figure 1), that went full text review and have been summarized as following (Table 2).
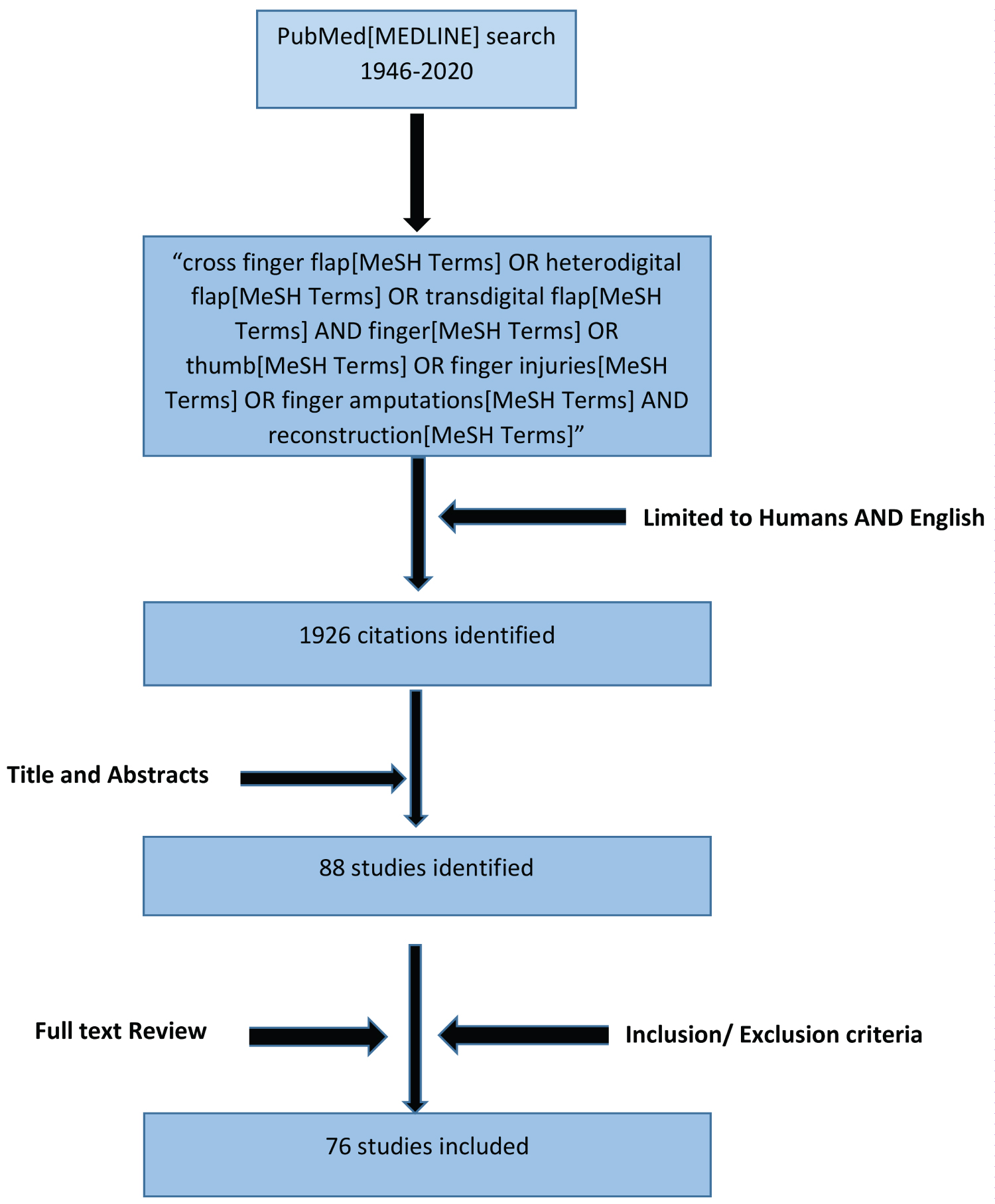 Figure 1: Flow chart of literature search. View Figure 1
Figure 1: Flow chart of literature search. View Figure 1
Table 2: Chronology of evolution of cross-finger flap with its variants. View Table 2
The earliest report of using trans-digital flap repair that could be found in literature was done in a series of 6 cases, by Gurdin and Pangman in 1950 [1] for finger injuries, as a two staged procedure. They used it when there was exposed bone or tendon, defect size was not very extensive, and donor finger was uninjured. They divided the flap at an interval of 2-3 weeks and reported no flap loss. However, it was Cronin [2] who first used the term cross finger flap in 1951. In the same year, Horn [3] reported excellent to good follow up result in 9 out of 10 cross finger flaps performed for traumatic amputation of distal phalanx and in two cases of extensive pulp loss. He also published the surgical principles of preparation of defect, atraumatic raising and tensionless insetting of flap, donor site grafting, adequate immobilisation and dressings, and flap division in 10-14 days. He suggested flap should be limited within joint flexion creases, and must not coincide with midline of palmar aspect of donor finger. He enumerated rheumatoid arthritis, Raynauds disease, Dupuytren's contracture and advanced age as absolute contraindications for flap repair.
Adding to the points of Horn, in 1952, Tempest [4] stressed the importance of fingertip repair to elude chronic infection, scar, pain and anaesthetic fingertip. He enumerated advantages of cross finger flap for fingertip repair, namely better durability than any other part's skin, sensory recovery. He was the first to mention that flap can be raised proximally, distally or longitudinally based. He advocated against use of volar skin, not to violate neurovascular bundle, and flap division to be done at 2-3 weeks. In 1957, in a series of 17 patients, Curtis [5] used cross finger flap for reconstruction of finger injuries with 100 percent successful surgical result. Apart from the principles proposed by previous authors, he added (1) Dividing a layer of oblique fascial fibres to gain more pedicle length laterally, and (2) To place skin graft over donor finger and pedicle so as to obtain minimum scar. Kislov and Kelly [6] presented series of 53 cases, who underwent cross finger flap for reconstruction of traumatic amputation, flexor skin avulsion, degloving of terminal digit, secondary repair of scarred amputation stumps, defect cover following flexor contracture release. 34 flaps had excellent results. They introduced immobilisation using Kirschner wire, which was passed from middle phalanx of recipient finger transversely to proximal phalanx of donor finger, protecting the extensor apparatus and neurovascular bundles. Period of immobilisation ranged from 7 to 16 days.
Hoskins in 1960, mentioned that in longer flaps a ratio of 1:3, width-to-length ratio, must be maintained, and the pedicle must be proximally raised on the donor digit [7]. In an ambitious attempt to compare the late results of fingertip reconstructions using cross finger, split or full thickness grafts, palmar flaps or abdominal pedicled flaps done in 235 patients, Sturman and Duran [8] found that cross finger flap had better sensory recovery (mean two-point discrimination 6 mm), and lesser tenderness, cold intolerance and disability than other reconstruction modalities. In 1965, Smith and Bom [9] were the first to use esthesiometer to measure two-point discrimination to evaluate sensory outcome in 17 out of 29 cross finger flaps used for fingertip reconstruction. Other measures used to assess outcome were sensibility to light pin-prick and touch, tip contour, sweating, mobility in donor and recipient fingers. In 1967, Thomson & Sorokolit [10] published a follow up study, in which 75 fingertip amputations in children were reconstructed with cross finger flap. Clinical assessment of reconstructed fingertip in terms of hyperesthesia, cold intolerance, sensory recovery (using two point discrimination test), colour, scar over donor areas and complications were done. They concluded that better clinical results are obtained in children in comparison to adults undergoing cross finger flap, namely lesser altered sensation, no postoperative stiffness, better aesthetic outcomes. So they recommended to include all age groups as an indication for cross finger flap, which was limited to above 7 years of age in that era. Wilkinson [11] reported 2 cases where functional thumb pad was reconstructed using radial innervated cross finger flap from proximal phalanx of index finger. Artz and Posch [12] were first to use cross finger flap to treat congenital broad constricting band, with an atrophic distal phalanx, in 3 cases. However they cautioned its use in narrow bands, for which multiple Z-plasty technique is ideal. In 1979, Hamilton, et al. [13] presented a series of 3 cases where they successfully used cross toe flap cover.
In 1980, Atasoy [14], one of the greatest pioneer of finger reconstruction, used radially based flap from proximal phalanx of thumb to reconstruct index finger tip injuries in 10 patients. He cautioned to preserve the dorsal sensory branches of the thumb and to pin index finger to the thumb. Nicolai and Hentenaar [15] were the first to objectively measure the progress of sensory recovery in 51 cross finger flaps, in 1981, by measuring difference between two point discrimination of flap and corresponding area in contralateral digit. They concluded that maximum sensation reaches within one year and usually does not improves further. Younger patient achieve better recovery. But results are unpredictable in patients over age of 20 years.
After 35 years of its inception, Kappel and Burech [16] published their results of cross finger flap over more than 200 patients. Various subjective questioning and objective parameters for neurosensory, functional and aesthetic outcomes were assessed, and finally declared cross finger flap as an "established reconstructive procedure".
In 1971, Alonso-Artteda [17] increased the umbrella of cross finger from mere defect cover to its use in replantation. He reported a case in which right hand ring finger degloving injury with distal phalanx amputation was replanted and a cross finger flap (from middle finger) along with its ulnar neurovascular bundle was used to wrap around the avulsed ring finger. The syndactyly thus resulted was released two weeks later. Normal length was restored with good sensation and mobility. He also suggested that with a bone graft combined with cross finger flap having one complete neurovascular bundle an amputated digit can be even lengthened. Joshi [18], in 1976, reported two cases of technically demanding two staged sensory cross finger flap. In first stage, a radially based flap elevated preserving the dorsal branch of volar digital nerve. In next stage, this branch is dissected out, isolated from main neurovascular pedicle of donor finger and transposed onto recipient finger during flap detachment. A two point discrimination test after 2 months ranged 5-9 mm. In 1982, Sorman reported a case in which viable distal phalanx tip of injured ring finger was transferred over amputee stump of middle finger [19]. Anastomosis was done between ulnar digital artery and nerve of tip of ring finger to corresponding artery and nerve of middle finger. Venae comitantes were left intact within the bridging skin pedicle, which was divided after 3 weeks. Thus length of amputated middle finger was restored.
In 1983, in an attempt to reconstruct 8 fingertip amputation, Cohen and Cronin used innervated cross finger flap [20]. In lines of Joshi they dissected out the dorsal sensory nerve from end which is distal to pedicle in donor finger, and the digital nerve (or a branch) in recipient finger. An epineural neurorrhaphy between them is performed during first stage of flap insetting. After mean follow up of 14.4 months 7 patients acquired average two-point discrimination of 4.8 mm, as against in the control group who underwent standard cross finger flap, only 50 percent achieved a mean upto 9 mm. However they warned its use for defect in proximal segment. Following footsteps of Cohen, in 1985, Sucur performed cross finger flap based on superficial terminal branch of radial sensory nerve for volar defect of thumb in 5 patients [21]. Walker, et al. [2] performed cross finger flap for 6 patients with thumb pulp loss and transposed the radial sensory branches of the flap to recipient finger in first stage itself, and followed for a mean of 3 years. Preblock and postblock (radial sensory nerve) sensibility testing of radial and ulnar sides of the flap suggested that active sensory axons present in flap inhibits the functional or anatomic neurotization of the transferred flap. This hypothesis was not previously found in man, but in experimental animals.
Another breakthrough in use of cross finger flap came when Martin [23] suggested use of reverse cross finger flap, not to cover a defect but as a vascularized vein graft carrier in 3 cases of Wolff class II & III ring avulsion injuries by creating venous anastomoses dorsally. Using the technique of Cohen, Lassner, et al. [24] performed innervated cross finger flap by coapting dorsal sensory branch of non-adjacent donor finger with contralateral nerve stump of injured finger in stage one. In addition they also coapted the adjacent donor nerve with the nearby nerve stump of traumatised finger in stage two during flap division. In this bilaterally innervated cross finger flaps they obtained far superior sensory recovery (average two-point discrimination of 3.6 mm) in their case series of 15 patients with zone 2 & 3 finger pulp amputation. In 2011, Zhao, et al. [25] presented a novel solution for venous congestion post digital replantation, which could not be conservatively managed, or by cross anastomosis, vein grafts, reanastomosis. They used proximally based cross finger flap as venous conduit in 10 such patients, in which 9 had successful results. In 2012, Wang, et al. [26] reported reconstruction of 18 degloving finger amputation using a combination of bilaterally innervated cross finger flap and a composite free flap from the dorsal aspect of second toe. All the cross finger and free flaps survived well. At mean follow up of 17 months, they assessed static two point discrimination (2PD), cold intolerance, range of motion and donor sites morbidity.
Until 1982, cross finger flap was used only for reconstruction of amputated finger stump or volar defects. Taking inspiration from Pakiam [27], Atasoy introduced reversed cross finger subcutaneous flap for dorsal digital defect in series of 4 patients [28]. The thin full-thickness skin flap elevated from dorsum of middle or proximal phalanx of donor finger itself cover the donor defect, while the adipofascial tissue covers the recipient dorsal defect. Fejjal, et al. in 2008 [29] reported a case in which this flap was used to cover index finger dorsum defect, with successful results. Again Atasoy, et al. in 1983 [30], presented a series of 4 patients with hook nail deformity with a follow up of 1 to 4 years, which was corrected using cross finger flap. They named it "antenna" procedure, as it looks so due to multiple small K-wires used in first stage. Patients achieved upto 4-8 mm of two-point discrimination. In 1985, Robbins [31] used de-epithelised cross finger flaps in 10 patients with dorsal finger defect. Only difference from Atasoy's reverse cross finger flap was he completely removed the split skin graft. In the same year, Groenevelt, et al. [32] used cross finger flap from scarred skin of ring finger to cover exposed tendons following release of 21 palmar flexion contractures of little finger and 4 button hole deformity of PIP joint. All the flaps survived, were cosmetically favourable and showed no tendency to contract.
Vlastou, et al. in 1985 [33], introduced a rather radical modifications, when they performed volar cross finger flap using proximal phalanx of middle finger to cover thumb defects of 10 patients. They enumerated its advantages, namely better bulk, as well as tissue and colour match for thumb, comfortable positioning, very reliable, and decreased chances of contracture. The patients had no donor site morbidity, painful scar or contracture or decreased grip strength or adhesions. In 1986, Yanai, et al. [34] presented 4 cases of thumb tip reconstruction with flag shaped cross finger flap harvested from dorsum of middle phalanx with its pedicle raised from radial side of proximal phalanx, approx. 1 X 0.5 cm. All the flaps developed distal margin blistering, however none of them had necrosis and survived well. In 1988, Gault & Quaba [35] established role of cross finger flap in primary management of 5 untidy flexor tendon injuries, with 60% excellent and 40% fair results as per Kleinert criteria. This was comparable to the results of zone 1 & 2 flexor injuries with soft tissue loss. Robbins in 1988, innovated "Jam Roll" flap for reconstruction of oblique fingertip amputation in a 15 year girl, using de-epithelised cross finger flap, and preferred it over a thenar flap for giving bulk [36]. In 1991, Harrison, et al. [37] successfully covered the volar defect after releasing Dupuytren's contracture in 15 patients, with a one stage cross finger flap, raised from dorsum of adjacent fingers proximal phalanx. They advocated maximum permissible width of 1 cm for primary closure of donor defect and to centre the pedicle in proximity to web space. Mutaf, et al. [38], in 1993 advocated a C-ring flap design, an axial pattern cross finger flap based on one digital vascular bundle either proximally or distally. They successfully used this innovated flap in 12 patients with various finger injuries. Two times size, wider rotation arc, excellent blood supply were the advantages over traditional cross finger flap.
After the introduction of reverse digital island flap by Sapp, et al. [39] in 1983 initially designed for homodigital use, in 1995, Lai, et al. [40] pioneered a bold modification, in which they harvested reverse digital artery neurovascular flap based on palmar digital arterial network, along with digital nerve dorsal branch sparing the radial digital nerve, from lateral aspect of donor finger to cover the soft tissue and nerve defect over adjacent injured finger. In lines with Lai, Germann, et al. [41] in 1997, successfully used reverse pedicle heterodigital cross finger island flap in 5 patients. 3 of them suffered congestion but eventually all of the flaps survived well. Following this, in 2007, Nuzumlali, et al. [42] presented the versatility of this midlateral reverse-flow digital artery cross finger flap to cover finger defects of 9 patients. They noted no complications and achieved a two point discrimination score of 3-4 mm in 2 years in 7 patients. They warned not to elevate the flap distal to middle of middle phalanx, and cover donor area with skin graft.
El-Khatib [43] in 1996, described elevation of adipofascial axial pattern cross finger flap with either side vascular pedicle, proximally or distally based, for finger defect cover in 15 patients. The following year, Spokevicus and Gupta [44] presented 2 cases in which they harvested innervated cross finger flap along with some extra subcuticular tissue from adjacent phalanx, which was used to cover nail bed defect in one case and in the other to provide bulk to the finger pulp. They reported no donor morbidity or flap necrosis. Sabapathy [45] made use of soft tissue from non-adjacent injured fingers to cover small defects in salvageable digits, in 5 cases of multi-digital mutilating injuries. They named it as "jumping" cross finger flap. Perks being replacement of like with like, and least amount of tissue is discarded. In 2000, Chakrabarty, et al. [46] performed two cross finger flaps from middle and proximal phalanx of middle finger to cover defect over index finger, sparing 1 cm of skin bridge over PIP joint and recorded almost negligible morbidity of donor finger in terms of mobility after 6 months of follow up. In 2004, Al-Qattan [47] reported the use of distally based adipofascial flaps for dorsal digital defects as cross finger and turnover flaps in series of 15 cases. In the subsequent year [48], he presented a comparative analysis, where de-epithelised cross finger flap done in 31 patients and turnover adipofascial flap was done in 42 patients, and reported that latter was better suited in children, elderly with joint diseases and multiple finger injuries.
Tadiparthi, et al. [49] increased the reach of cross finger flap far beyond imagination. To cover a medium sized circumferential defect of ring finger, they used skin flap form donor middle finger (for volar cover) and the adipofascial flap from same digit (for dorsal cover). They named it "open book" flap, and reported no immediate or post-operative complication or stiffness in their patient. Capitalising on this concept, in 2010, Moosa [50] introduced "double cross finger" flap. In the 22 cases of ring avulsion injury (Adani type IV), in middle or ring fingers, he performed 44 transdigital flaps from both adjacent donor fingers (longer cross finger flap to cover volar defect of recipient finger while shorter reverse cross finger flap from another donor to cover the dorsal defect). With very few complications of donor site, they achieved 9-11 mm of two-point discrimination and active range of motion of upto 70-80 degrees at MCPJ and 60-75 degrees at PIPJ.
Mishra and Manisundaram [51] described another modification where they raised a reverse flow skin flap from hemidorsum of donor finger to cover defects in 32 finger injuries. The limits are midlateral line, midline of dorsum of finger, distal interphalangeal joint and upto 2 mm of web space. It gives an advantage of lesser donor site morbidity, however lesser width is a limitation. Hahn, et al. [52] in 2010, in their series of 9 patients with long standing proximal interphalangeal joint contracture performed cross finger flap for defect cover and vigorous post-operative exercises, showed promising results. Ismail described use of an adipofascial fillet flap from a non-viable digit for reconstruction of adjacent finger defect in 2010 [53]. Shah used cross digital dorsal adipofascial flap for post thermal burn dorsal defect, in which paratenon was also damaged, in 2010 [54]. They reported no post-operative complications. Patil [55] performed distally based traditional cross finger flap to cover 27 amputation stumps in avulsion amputation and reported stable cover and full recovery of range of motion in donor finger after an average 13 months follow-up. They routinely designed the flap by planning in reverse and in none splintage was done. In 2013 Feng, et al. [56] performed cross finger flap based on dorsal branch of proper digital artery, located withing 5-7 mm distal to PIP joint at middle phalanx, for 18 cases of distal fingertip degloving injuries. They also coapted the dorsal branch of proper digital nerve with digital nerve stump of injured finger and used 1.5 mm K-wire fixation for 2 weeks immobility. They reported a mean static two-PD 6.3 mm at mean follow up of 20.5 months. They advocated its indication in distal fingertip degloving injuries with 2 to 6.5 cm defect size. The following year Tan, et al. [57] performed series of artery-only distal fingertip replantation, and augmented the venous outflow by insetting a trap door flap from adjacent donor finger with the de-epithelised area of amputee. 3 of the amputees survived after flap division in 2-3 weeks. In the same year Gopalakrishna [58] reported a case of ring finger avulsion that was salvaged by a double cross finger flap with satisfactory 25 year follow up results.
In 2016, reverse cross finger flap's indications, contraindications, technique, and post-operative management were described by Atasoy [59]. In 2017, Yang, et al. [60] described use of reversed cross finger fascial flap combined with 0.3 cm split-thickness toe nail bed graft for reconstruction of large defect of nail bed in 6 patients, with satisfactory results. In 2018, Li and Chen [61] presented a case report in which composite grafting of zone 1A thumb tip amputation was performed. Without any vascular anastomosis the graft survived as cross finger subdermal pocketing into middle phalanx of middle finger was also done. In same year, Al-Qattan, et al. [62] presented case series with 4 patients, in which large defects of index or ring fingers were covered by two dorsal cross finger flaps (either traditional or reverse cross finger) using middle finger as single donor. They observed no postoperative complications. In donor finger mild stiffness at DIP joint and hyperpigmentation in all patients, blistering of grafted site in one patient, mild cold intolerance in two patients were reported. None developed any painful neuroma in their 7-8 months follow up period. Paterson [63] and Koch [64] had previously evaluated donor finger morbidity in their case series of 16 and 23 patients respectively who underwent cross finger flap, in terms of stiffness, cold intolerance, active and passive range of motion (ROM), pain, aesthesis, pinch grip strength etc.
Chong, et al. [65] performed laterally based cross finger flap for volar or dorsal soft tissue defects in 13 fingers. Flap was elevated from middle or proximal phalanx with pedicle over midlateral line (minimum pedicle width 5 mm) and donor site primarily closed (maximum flap width 13 mm). 11 of the flaps completely survived. They reported lesser donor site morbidity than conventional cross finger flap. In 2019, Gunasagaran, et al. [66] reported reconstruction of fingertip and nail bed post chemical burn, using cross finger flap and split thickness nail bed graft. Following footsteps of Sabapathy and Ismail, in 2019, Al-Qattan and Mohrij [67] reported 2 cases with crush injury of multiple fingers, where defects were covered using spare parts in cross finger fashion.
The survivability of flap depends on neovascularisation. Clinical assessment of capillary filling after applying tourniquet to the donor finger was at times equivocal. In 1990, Hallock [68] showed first time successful use of laser doppler flowmetry as a noninvasive objective measurement of relative perfusion in cross finger flaps and concluded that using 50% flow criteria all flaps survived following division. In their article published in 2001, Steenlage [69] described the method of evaluating the capillary refill of the flap clinically to determine the correct time for division.
Nishikawa and Smith [70] performed cross finger flaps for 54 single fingertip volar defects. In this ambitious study done over 5 years, the outcomes were measured, first time, based on subjective questionnaire, timed capillary return & surface temperature for vascularity, electrical conductance testing as a measure of sweating, objective tests for sensory recovery namely protective sensation to pin prick, hot and cold thresholds, static and moving two-point discrimination, Von Frey hair testing, moving light touch, vibration, voltage and current thresholds. For hand functions they used questionnaire, pinch, grip strengths, joint mobility, pick up testing and tactile gnosis. Woon [71] performed 31 cross finger flaps using dorsum of middle or index finger to reconstruct oblique defects of distal thumb, and after a mean follow up period of 137 days assessed 2PD, Semmes Weinstein pressure aesthesiometer testing, ROM, donor site morbidity. They also tabulated their excellent sensory recovery and compared with previous studies. In 2015 Rabarin, et al. [72] reported long term outcomes of cross finger flap performed in 28 patients for fingertip amputation. After a mean follow-up period of 19.7 years they evaluated various parameters- complications, pulp volume as a ratio of contralateral and reconstructed fingertip pulp on lateral X-rays, static 2PD and Semmes Weinstein monofilament test of reconstructed tip compared to contralateral fingertip, cold intolerance, presence of neuroma, patient satisfaction with visual analogue scale.
It took more than 30 years since the first description of innervated cross finger flap for someone to conclusively prove its better sensory results over traditional cross finger flap. Lee, et al. [73] conducted a large series of reconstruction of fingertip defects, in which 69 cases underwent innervated cross finger (neurorrhaphy was performed between pulp branch from proper digital nerve of donor finger and recipients sensory nerve, while rest 21 cases defect cover was done only with the opposite pulp tissue of adjacent finger. They reported that after 12 months of surgery mean two-point discrimination in non-innervated cross finger was 7.2 mm, while in innervated cross finger flap was 4.6 mm which was statistically significant (p = 0.001). All flaps survived. Taking inspiration from Feng [56] and Lee [73], in 2014 Chen, et al. [74] published an article, comparing outcomes of 17 bilaterally innervated sensory cross finger flap and 28 non innervated cross finger flap, all of which were based on dorsal branch of digital artery, for fingertip degloving injuries. They reported significantly better static 2PD, cold intolerance, and pain of injured finger (P < 0.05) and lower incidence of neuromas in the innervated pedicled cross finger flap in comparison to non-innervated pedicled cross finger flap. By contrast the same parameters had no significant difference in the two groups in their donor fingers.
In 2013, Kumar and Segu [75], in their unexpected study, performed cross finger dorsal adipofascial flap in their 15 patients with various finger injuries and compared their aesthetic outcomes with standard cross finger flaps 6 months post-operatively. They reported that mobility and sensory recovery was similar to the standard cross finger flap but this flap was aesthetically superior and therefore increased the horizon of dorsal adipofascial cross finger flap to injuries beyond the dorsal defects. In their prospective study, Ekinci and Gubuz [76] evaluated the surgical and clinical outcomes of reversed cross finger subcutaneous flap in 25 patients with dorsal digital defects. 6 months postoperatively they recorded 2PD, ROM of donor and recipient fingers, cold intolerance and Quick Disabilities of the Arm, Shoulder and Hand (DASH) score. They concluded owing to minimal donor site morbidity, satisfactory sensory and functional results, easy applicability, this flap must be preferred in dorsal digital defects.
Surprisingly for almost 30 years palmar cross finger flap was totally silent until In 2014, Erken [77] performed volar cross finger flap from index finger for reconstruction of dorsal oblique and transverse amputations of thumb in 12 patients. They reported mean 2PD scores of 4.5 mm and 4.3 mm in reconstructed thumb tip and donor site respectively after a mean follow up of 28 months. They also achieved excellent range of motion of injured and donor fingers.
Kim [78] measured the long term outcomes of reverse digital artery cross finger flap done for defect cover over 11 failed index and little finger replants. In all cases neurorrhaphy was performed between donor dorsal sensory branch and injured proper digital nerve stump of injured finger. All 11 flaps survived well. After a mean follow-up of 53 months mean static 2PD was 5.3 mm, none had any cold intolerance or dysesthesia. ROM of donor finger achieved satisfactorily.
The Authors declare that there is no conflict of interest.
This study received no grants.
Not applicable.
None declared.
SSC: Study design, data acquisition, and analysis and interpretation of data. Manuscript preparation, drafting the article, revising it critically for important intellectual content and final approval of the version; SA: Literature search, study design, data collection. Revising it critically for important intellectual content and final approval of the version; MM: Literature search, study design, data collection, revising critically for important intellectual content and final approval of the version; RKS: Editing and revising the manuscript critically for important intellectual content writing, critical revision, and final approval of the version.