Historically, heat has been used to treat wounds. Now a days electrosurgery unit (ESU) is an important part of operation theatre equipments utilized by almost every surgeon. Electrocautery and diathermy are the terms typically used by medicals and paramedicals including surgeons for electrosurgery. However, electrosurgery, electrocautery and diathermy are three different tools. Cutting monopolar needle electrode of electrosurgery is a safe tool for skin incision in neurosurgery but it is not a popular tool used by surgeons to make skin incisions. Potential reasons for not using this tool for skin incision can be poor wound healing, deep burning of underlying tissue or lack of awareness about this tool. The objective of this case study is to bring awareness about 'cutting monopolar needle electrode of electrosurgery' as an available tool for skin incision in neurosurgery with less blood loss and marked reduction in incision time than stainless steel surgical blade.
Monopolar needle, Electrode, Electrosurgery, Skin incision, Neurosurgery
The objective of this case study is to increase awareness about the use of monopolar cutting electrosurgery as a tool for skin incisions in neurosurgery. Neurosurgeons typically use stainless steel blades for skin incisions. However, there are other safer tools and technique such as the monopolar cutting needle electrode of electrosurgery which is not a common practice and neurosurgeons may not be aware of this tool. The reason could be, fear of deep skin burns and poor wound healing or awareness about the technique.
Heat has been applied to treat wounds since ancient times in the form of heated stones and metals. Bleeding from war wounds was stopped by application of hot sword. Same principle is used in electrocautery, in which heated probe by direct electric current is applied to stop bleeding. Electrocautery cannot be used to cut, as it only coagulates the tissue. Electrosurgical device was first developed by William T. Bovie, an electro physicist in Harvard University. Credit goes to the legend in neurosurgery, Harvey Cushing using electrosurgical unit first time in operation theatre for removing a mass from a patient's head, at Peter Bent Brigham hospital in Boston, Massachusetts in 1, 1926 [1].
In Electrosurgery, high-frequency (radio frequency) alternating electrical current is used to cut, coagulate, desiccate, or fulgurate biological tissue [2,3]. Mostly surgeons from almost every specialty use electrosurgery but call it as electrocautery or diathermy [4-7]. Electrocautery, diathermy and electrosurgery are three different technique. Electrocautery uses the direct current which does not pass-through patient's body, only heated electrode touches the tissue to get desired effect. In diathermy, electric heat produced due to rotation of molecular dipoles in a high frequency electromagnetic field. In electrosurgery, alternating current is converted into high frequency (radio frequency) of more than 100,000 cycles per second (100 kilohertz) by electrosurgical unit, which passes through body or human tissue. Standard alternating electric current at 60 cycle per second stimulates nerves and muscles giving rise to electric shock like effect. Nerve and muscle stimulation ceases at 100,000 cycles per second (100 kilohertz) and there is no electrocution. For electrosurgery, standard alternating electric current is converted into high frequency (radio frequency) by electrosurgical generator also called electrosurgical unit (ESU). Hand piece connected to the ESU, is applied to the tissue for desired effect. Hand piece is either monopolar or bipolar, difference between two is that in monopolar hand piece has one electrode while in bipolar both electrodes are in hand piece. Constant waveform of low voltage generated from ESU gives cutting effect to the tissue, while intermittent waveform of high voltage helps in coagulation.
In monopolar electrosurgery, hand piece is active electrode attached to ESU and requires another electrode called dispersive electrode which is put elsewhere on patient's body. Dispersive electrode is also attached to ESU. Electric circuit in monopolar electrosurgery is composed of ESU, hand piece, patient, dispersive electrode, and back to ESU. In bipolar electrosurgery, hand piece is has both electrodes at the tip of a forceps. Current travels through tissue between two tips of bipolar forceps, not through patient.
Technique: Needle electrode of monopolar hand piece on cutting electrosurgery is used for making skin incision. Blunt monopolar hand piece electrode should not be used. Gentle retraction on skin edge is applied to widen gap between skin edges. Vessels are identified and coagulated by bipolar forceps before cutting. Bleeding and blood oozing out from cut skin edges is remarkably less with skin incision by monopolar cutting needle electrode of electrosurgery (as shown in Figure 1 and Figure 2) while more in a skin incision made by stainless steel surgical blade (Figure 3). No normal saline or xylocaine infiltration is required in subcutaneous plain before putting skin incision with monopolarcutting electrosurgery. Incision in fascia is also made with needle electrode. Surgical wound made by needle monopolar cutting electrosurgery showed proper healing of wound after stitches removal on 7th post stitch day (as shown in Figure 4).
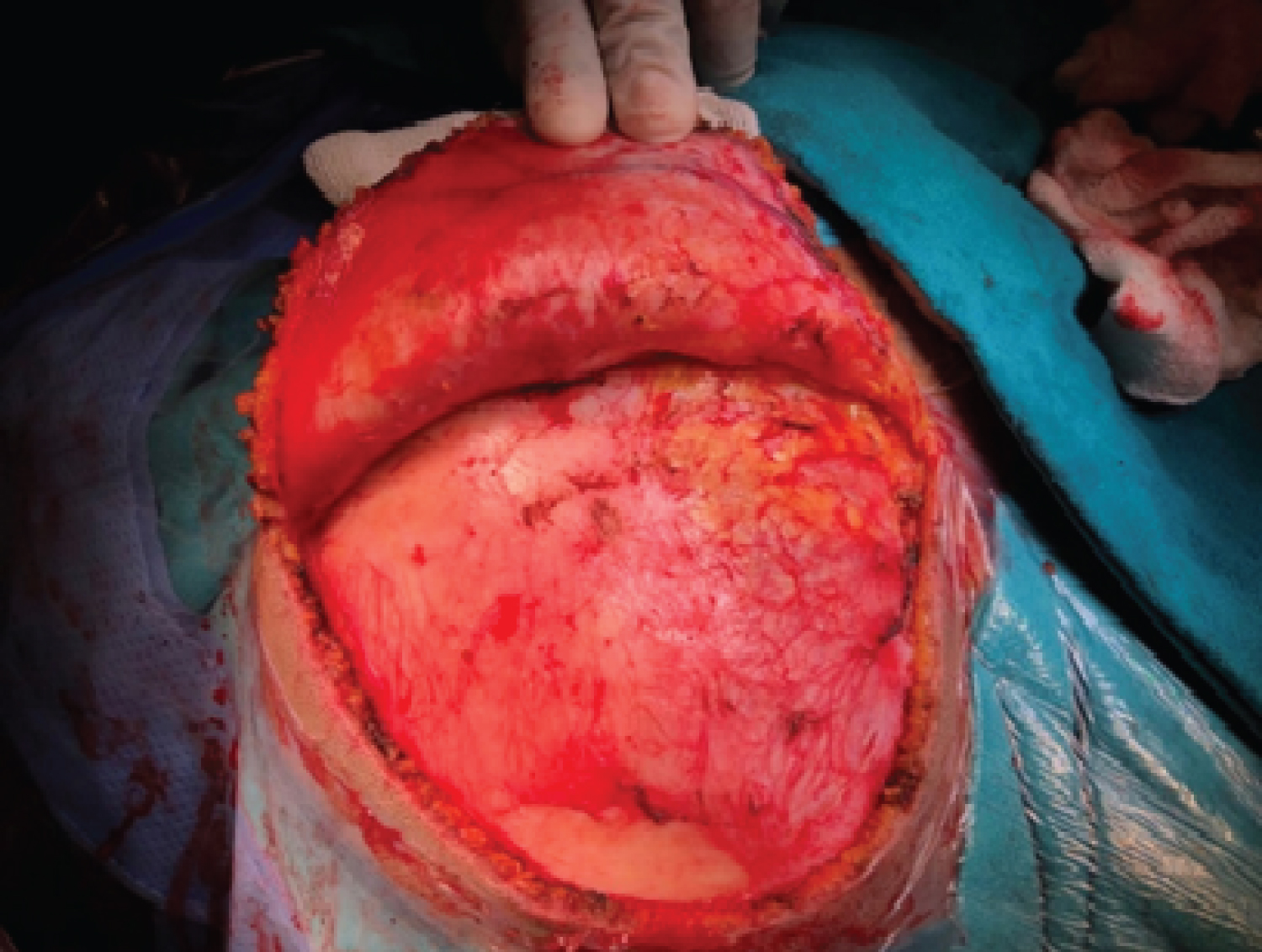 Figure 1: Skin incision with electrosurgery, cutting monopolar needle electrode.
View Figure 1
Figure 1: Skin incision with electrosurgery, cutting monopolar needle electrode.
View Figure 1
 Figure 2: Skin incision with electrosurgery, cutting monopolar needle electrode.
View Figure 2
Figure 2: Skin incision with electrosurgery, cutting monopolar needle electrode.
View Figure 2
 Figure 3: Skin incision with stainless steel surgical blade.
View Figure 3
Figure 3: Skin incision with stainless steel surgical blade.
View Figure 3
 Figure 4: Proper wound healing after suture removal on 7th post stitch day, electrosurgery skin incision of Figure 2.
View Figure 4
Figure 4: Proper wound healing after suture removal on 7th post stitch day, electrosurgery skin incision of Figure 2.
View Figure 4
Initially, electrosurgery was used for haemostasis by coagulating bleeding vessels. It was not used for making skin incisions, because of fear of poor wound healing, deep burns, excessive scarring, and infection. Due to continuous upgradation and improvement in electrosurgical units, now electrosurgery is safe for making skin incisions by monopolar needle electrodes. Electrosurgical skin incision is faster with less bleeding and results are comparable [8,9] with skin incision made by stainless steel blade in terms of wound healing, infection & pain at incision site and scar formation. In a survey conducted among neurosurgeons worldwide site on telegram "Neurosurgery cocktail", one out of ten responded that they use monopolar electrosurgery for making skin incision during neurosurgery, rest nine used stainless steel blade. Potential reason for not using monopolar cutting electrosurgery needle electrode for making skin incision in surgery, could be fear of deep skin burns and poor wound healing or awareness about it. There are no added complications while using needle electrode of monopolar cutting electrosurgery over stainless steel surgical blade for making skin incision in neurosurgery.
Cutting monopolar needle electrode of electro surgery is a safe available tool for making skin incision in neurosurgery, with less blood loss and marked reduction in incision time. It is an equally good alternative to stainless steel surgical blade.
None.