Treatment of high-energy trauma of the lumbosacral region is a challenging entity for clinicians. They are complex and often associated with other injuries such as active bleeding and substantial soft tissue injuries. Therefore, good wound healing is reliant on multiple local and systemic factors. Only a multidisciplinary approach between the trauma team and subspecialists will dictate the most appropriate management for these patients, and recent data has shown that best outcomes are obtained when these lesions are cared for at level 1 trauma centers. We present a case of complex major trauma involving rachis, thorax, abdomen, pelvis and lower limbs.
Sacral fractures, Major trauma, Wound care
GCS: Glasgow Coma Score; KPC: Klebsiella Pneumoniae Carbapenemase-producing; EF: Ejection Fraction; CRP: C-Reactive Protein; PCT: procalcitonin; CT: Computed Tomography; MRI: Magnetic Resonance Imaging; HBOT: Hyper Baric Oxygen Therapy; NPWT: Negative Pressure Wound Therapy; LTC: Long Term Care
Treatment of high-energy trauma of the lumbosacral region is a challenging entity for clinicians. They are complex in nature and pose diagnostic challenges and technical difficulties for treatment [1]. In addition, sacral fractures are often associated with other injuries such as active bleeding and substantial soft tissue injuries, because of the vulnerable soft tissue coverage around the pelvis. Therefore, good wound healing is reliant on multiple local and systemic factors and consequently each wound is very different to the next.
Only a multidisciplinary approach between the trauma team and subspecialists will dictate the most appropriate management for these patients, and recent data has shown that best outcomes are obtained when these lesions are cared for at level 1 trauma centers. A good functional outcome for this type of injury is the result of the combined effort of intensivists, orthopaedics, surgeons, together with hyperbaric physicians and physiotherapists in a multidisciplinary team.
We present a case of complex major trauma involving rachis, thorax, abdomen, pelvis and lower limbs.
A 24-year-old male patient presented to our Emergency Department after a high energy road-traffic accident. He was agitated, not conscious, not responsive to external stimulation (GCS 8) and dyspneic. After analgosedation and orotracheal intubation, once primary survey was terminated, a full-body CT scan showed: thoracic trauma (left pneumothorax, bilateral pulmonary contusions, displaced fractures of VI and VII left ribs), abdominal trauma (ruptured spleen), pelvic trauma (multifragmentary sacral fracture with extensive hematoma in the surrounding soft tissue, ischiopubic and ileopubic ramus fractures, bilateral acetabular fracture), vertebral trauma (L2 burst fracture with displacement of vertebral soma), limb trauma (bifocal fracture of left tibia and fibula) (Figure 1).
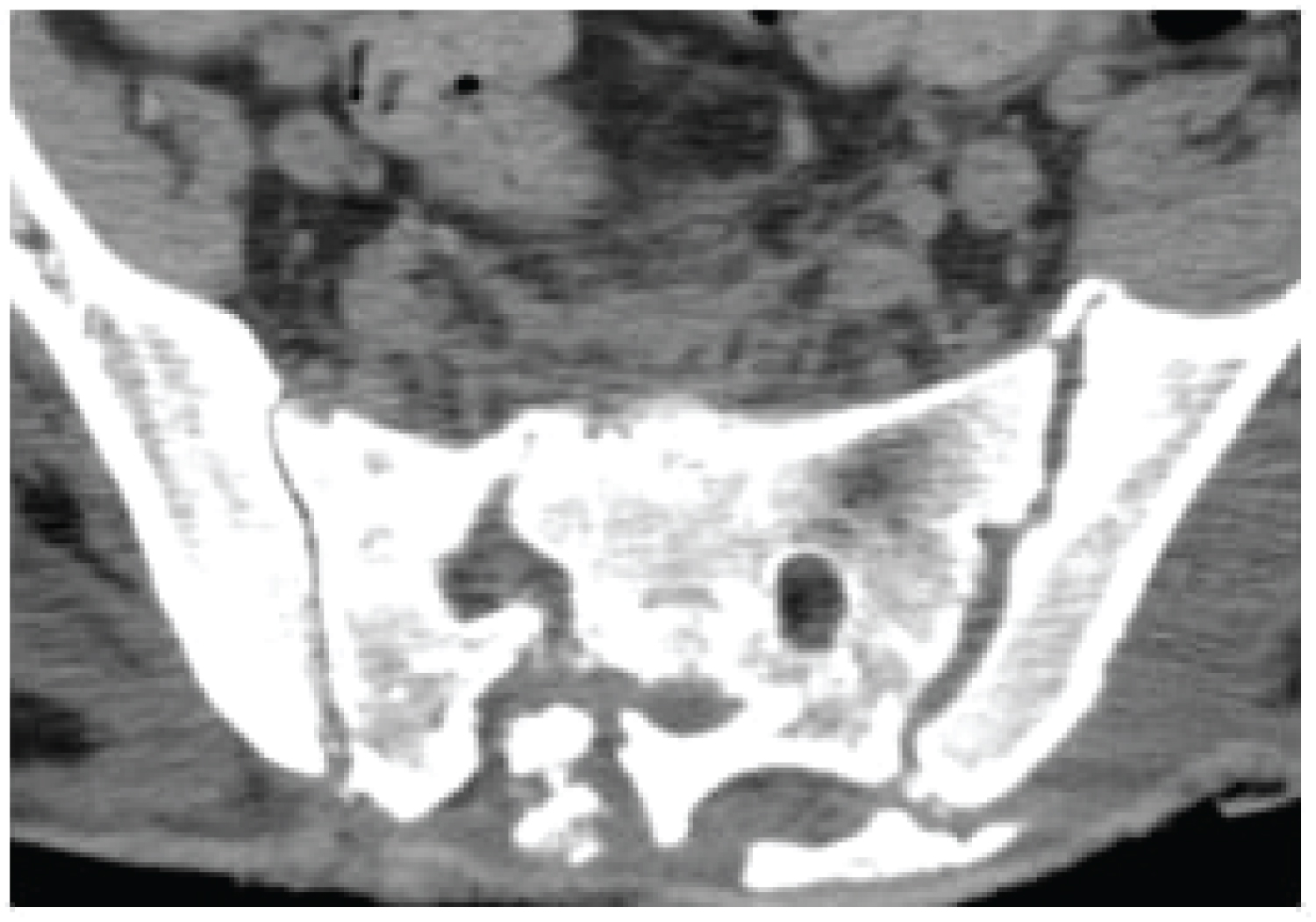 Figure 1: CT imaging showing sacral fracture.
View Figure 1
Figure 1: CT imaging showing sacral fracture.
View Figure 1
Subsequently the patient underwent surgery for splenectomy and fixation of left tibia and fibula fractures. Then he was admitted to the ICU. Both the neurosurgeon and the orthopedist do not give immediate surgical indication for the stabilization of the sacrum and the L2 fracture, but only a clinical re-evaluation after the patient's awakening and a lumbosacral spine MRI study.
On the 7th day after admission, an increase in size of the hematoma in the sacral and gluteal area bilaterally was clinically evident. Therefore, surgical incision and drainage was performed with the leakage of about 0.5 L of partially coagulated blood. A significant skin and soft tissue loss resulted following the surgical maneuver. An accurate assessment of the wound area was made by conducting a thorough evaluation of the size, depth, wound edges, skin temperature, and exudates and/or necrosis. The sacral decubitus ulcer had formed a huge pocket measuring 12 × 10 cm in size and 8 cm deep (Figure 2). There was some exposed muscle, tendons and bone visible at the base of the ulcer following sharp debridement of the necrotic tissue, classifying the wound as a stage IV injury according to NPUAP/EPUAP classification.
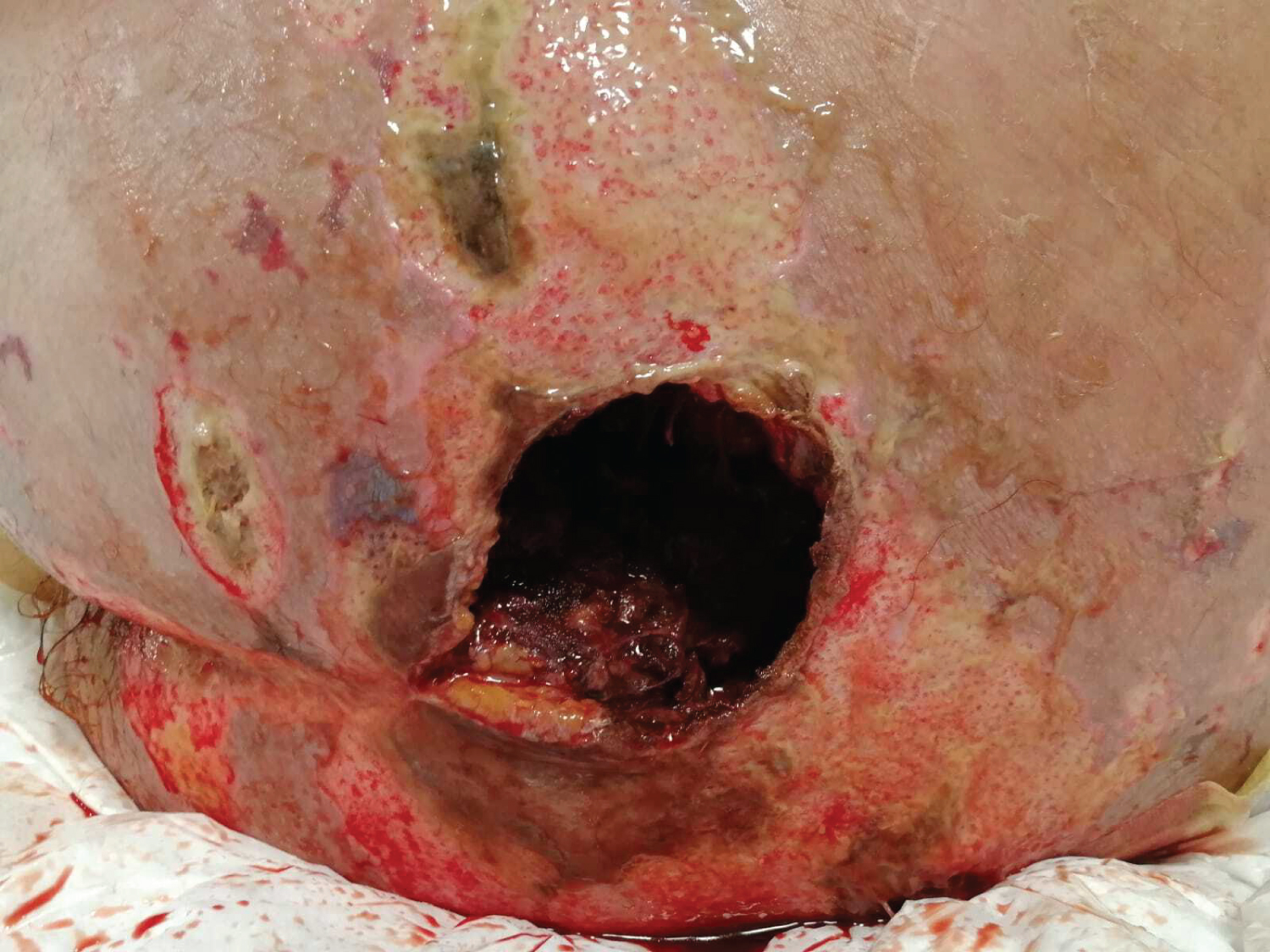 Figure 2: Extension of the sacral ulcer 7 days after admission.
View Figure 2
Figure 2: Extension of the sacral ulcer 7 days after admission.
View Figure 2
According to the TIME acronym (tissue debridement, infection/inflammation, moisture balance and epithelial edge), the initial management of the lesion included autolytic debridement of the wound bed with a necrotic base to remove infected, necrotic, and desiccated tissue. For this purpose, hydrogel-based dressings were used, covered with a thin polyurethane film and replaced every 2 days.
Wound swab for culture showed positivity for Klebsiella pneumoniae and Enterococcus faecium. Therefore, i.v. administration of ceftazidime/avibactam (2.5g tid), amikacin (1.5g uid) and tigecyclin (50 mg uid after 100 mg loading dose) was initiated according to antimicrobial sensitivity profile. A faecal collection catheter was applied for the management of incontinence in order to reduce the possibility of contamination with liquid or semi-liquid stool and prevents the skin being damaged by exposure to wetness, given the proximity of the faecal material to the wound. The skin surrounding the ulcer was kept clean and dry using a neutral pH skin cleanser, while an emollient product was used to hydrate xerotic skin.
A negative pressure therapy (NPWT) was started using polyurethane foam and wall suction. Instillation was carried out with 5% povidone iodine (10 ml) and normal saline (500 ml) twice a day. The NPWT system was changed every two - three days, making the wound less susceptible to cross-contamination.
After the first week of hospitalization in which the improvement of haemodynamics and resolution of rhabdomyolysis was achieved, a percutaneous tracheostomy was performed on the 10th day from admission. Then analgosedation was stopped resulting in progressive recovery of cognitive functions and hyposthenia to the lower limbs, while weaning from mechanical ventilation was achieved after 5 days.
Parenteral nutrition was started two days after splenectomy and continued for the first five days due to haemodynamic instability. Enteral nutrition was introduced on the 7th day postoperatively through a nasogastric tube. The caloric requirement, calculated with indirect calorimetry, was approximately 35 kcal/kg/day. Protein intake represented 25% of total calories and was about 1.8 g/kg. Immuno-modulating formulas containing arginine, glutamine and fish oils were used.
The patient underwent intense physical therapy to help alleviate his immobility status from the second week from admission and was repositioned every two hours using an air-fluidized bed as a supporting surface.
One month after admission the patient was referred for HBOT (hyperbaric oxygen therapy) and a total of 40 sessions were administered over 9 weeks. HBO was performed once a day, with weekends off. Treatment was given in a multiplace chamber at a depth of 2.4 ATA (14 metres of sea water (msw) with three 30-minute cycles of oxygen, separated by five-minute air breaks). The NPWT pump was switched off and disconnected for the duration of the treatment -one hour and 50 minutes- and was reconnected upon completion.
The development of ulcer severity was measured every 7 days with the PUSH-TOOL scoring system.
The amount of wound exudate gradually decreased and there were signs of improvements including significant granulation tissue development on the surface of the ulcer and a reduction in slough and necrotic tissue evident to the wound bed. After 2 months the sacral wound size reduced by 60% and it showed no more signs of infection, wound swab for culture was sterile and pressure ulcer severity decreased (Figure 3). At the same time CRP and procalcitonin (PCT) levels diminished. Antimicrobial therapy was stopped.
 Figure 3: Reduction of wound side by 60% 2 months after admission and 1 month after HBOT was started.
View Figure 3
Figure 3: Reduction of wound side by 60% 2 months after admission and 1 month after HBOT was started.
View Figure 3
Once a bedside swallowing assessment has been carried out, tracheal cannula and nasogastric tube were removed. So the patient returned to oral feeding.
One month later healthy and clean granulation tissue covered almost 80% of the wound; the patient was discharged from the hospital and transferred to the LTC facility where he was reviewed using a one-to-one interview. One month after discharge, the ulcer had completely healed and was ready for skin graft (Figure 4). The patient was able to manage independently the sitting position and to stand up with crutches. He did not have any new occurrences or recurrence of pressure ulcers.
 Figure 4: Improvement and almost complete resolution of the sacral lesion 4 months after the traumatic event.
View Figure 4
Figure 4: Improvement and almost complete resolution of the sacral lesion 4 months after the traumatic event.
View Figure 4
Traumatic wounds vary from abrasions and minor skin incisions to wounds with extensive tissue injury or loss and damage to bone and internal organs. Soft tissue reconstruction on sacral and coccyx is a challenging problem for reconstructive surgeons because of poor tolerance, challenging surgical debridement, and limited flap alternatives [2]. Primary closure of these wounds is avoided because of the high rate of recurrence with closure over the bony prominence. Skin grafting has a low success rate and is often precluded because of the frequent presence of a bony wound bed and the absence of adequate soft tissue bulk [3].
There are several metabolic conditions that contribute to the development of non-healing wounds. Apart from ischemia and hypoperfusion, other factors that prevent normal healing from occurring include poor nutrition, infection, oedema, persistent moisture, fecal and urinary soiling, shearing forces, supine position.
The approach has to be multidisciplinary and involves optimizing nutrition, controlling infection, improving the overall medical condition and eliminating sources of external pressure and contamination.
Infection control should be achieved by reducing wound bacterial burden. Systemically administered antibiotics do not effectively decrease bacterial levels in granulating wounds. Methods that may be suitable include enhancing host defense mechanisms, debridement, wound cleaning, and topical antimicrobials.
Nutrition must be adequate to provide sufficient protein to support the growth of granulation tissue. Proteins are required for the proliferation of fibroblasts and the synthesis and deposition of collagen. Proteins are also necessary for important immunologic functions such as phagocytic activity of macrophages, T-cell function, and antibody production. Malnutrition can impair wound healing by prolonging the inflammatory phase and reducing the proliferation of fibroblasts and deposition of collagen. Moreover, malnutrition is associated with increased risk of wound infection, which has deleterious effects on wound healing.
The underlying contributing factors for pressure ulcers must be reduced by providing pressure redistribution and specialized support surfaces. A repositioning schedule to avoid pressure on the wound should be established.
Consideration needs to be given to the pathophysiological effects of contamination by faecal matter in wound management. The combination of urinary and faecal incontinence results in increased skin wetness and permeability, leading to skin breakdown. Urine and faeces contain both proteolytic and lipolytic enzymes that are deactivated during the digestive process. If faeces remain on the skin, ammonia released from the faeces reactivates the enzymes leading to further skin irritation. The containment of faecal matter from the patient's skin is therefore a vital element in the maintenance of skin integrity. To prevent damage to the skin's integrity and wound contamination due to faecal incontinence, faecal collection systems may be used.
Meticulous local wound care with debridement and proper wound dressings will help maintain a healthy environment that will promote granulation tissue formation, tissue ingrowth and epithelization. Wound debridement can be accomplished by sharp debridement, wound irrigation, autolytic debridement and/or enzymatic debridement. The goal of debridement is to remove infected or devitalized tissue, pathogens, contaminants, and foreign materials, in order to prepare the wound bed for optimal healing and closure.
Local wound care with the help of wound dressings is an important element in the preparation of the wound bed for healing. The type of wound dressing used has to be individualized, based on the characteristics of the ulcer and the stage of healing [4].
In cases of significant tissue loss or when there are concerns about residual infection or tissue viability due to vascular compromise then NPWT can be valuable as a bridge to secondary closure or flap coverage. It aids closure in high risk traumatic wounds. Proposed mechanisms by which NPWT supports wound healing include; controlling oedema, promoting granulation tissue, improving micro-vascular circulation and decreasing bacterial load at the wound bed [5]. NPWT accelerates debridement in a similar fashion to autolysed debridement and physical debridement. It can also stimulate biofactors that can further promote wound healing.
Conversely, HBO treatment determines an increase in oxygen tension in tissues responsible of different advantages including the improvement of white blood cell function, enhanced fibroblast activity, promotion of angiogenesis, enhanced collagen synthesis, and reduction of oedema.
None.
None.
None.
CB conceived, designed and drafted the manuscript; DS and EA interpreted the data; IO, FS and SG critically reviewed the article; VS and IE acquired the data. All authors read and approved the final draft of the study.