Aortic dissection is a preventable life-threatening condition, but fatality can be extremely high if not treated timely. And if it is associated with dilated cardiomyopathy, it can be catastrophic for them, and managing this can be an anesthetic nightmare. Here, we present elderly female patients diagnosed with aortic dissection on evaluation with a known case of dilated cardiomyopathy coming for hip fracture fixation. The case was managed with low-dose spinal anaesthesia along with good hemodynamic monitoring, adequate fluid therapy, and careful planning.
Patients with aortic dissection and dilated cardiomyopathy presenting for a non-aneurysmal correction surgery pose a significant challenge for anaesthesiologists. Literature searches for managing these patients in the perioperative setting are scanty. Acute manifestation of aortic dissection is a life-threatening emergency with high-case fatality. In one study 30-day fatality rate was 47.45 for patients with type A dissections and 13.3% for patients with type B dissections, that survived hospital admission [1]. Moreover, dilated cardiomyopathy will further increase the risk of fatality in such patients due to compromised cardiac contractility and cardiac output. Here, we present a case of type B aortic dissection extending from the subclavian artery to the left common iliac artery along with a dilated cardiomyopathy (DCMP) diagnosed on echocardiography, with features of moderate to severe global hypokinesia posted for hip fracture surgery. Anaesthetic management for the hip surgery in this patient was particularly challenging as there was the risk of acute aortic dissection along with compromised cardiac function. This patient was successively managed well with good anesthesia planning. No such case report has been published till date now. Therefore, we aim to help anaesthesiologists adopt safer techniques for optimizing and managing these patients perioperatively.
A 68-year-old female patient came to the emergency department with an alleged history of falls at level ground. She was evaluated at another hospital, where an echocardiography finding revealed-a dissection flap in the descending thoracic aorta, moderately severe aortic regurgitation, mildly dilated left ventricle with moderate systolic dysfunction (LVEF-40%), and moderate global hypokinesia. For this above-mentioned echocardiographic finding, she was referred to our hospital. Two years ago, she was diagnosed with dilated cardiomyopathy (DCMP), for which she is taking metoprolol (50 mg) and aldactone. Also, she was known hypertensive for the last 5 years, for which she is taking the tablet losartan (80 mg). Her chest X-ray finding showed cardiomegaly and mediastinal widening (Figure 1), which was consistent with echocardiographic findings and an X-ray of the left hip revealed an inter-trochanteric fracture of the left femur. A CT angiogram (Figure 2) was done, as advised by the cardiothoracic team, which showed type B aortic dissection extending from the distal to left subclavian artery till bifurcation of the aorta and extending into the left common iliac artery with a total aortic diameter of more than 40 mm and patent false lumen of more than 22 mm showing no signs of rupture/impending rupture. Considering her age, and clinical and medical conditions, the cardiothoracic team has advised conservative management for dissection and stratified very high risk for any other surgical procedures. Since the management of an inter-trochanteric fracture is considered urgent and delaying it for more than 48 h increases the risk for both morbidity and mortality, the patient was posted for hip fracture surgery and an aesthesiologists were informed of the same.
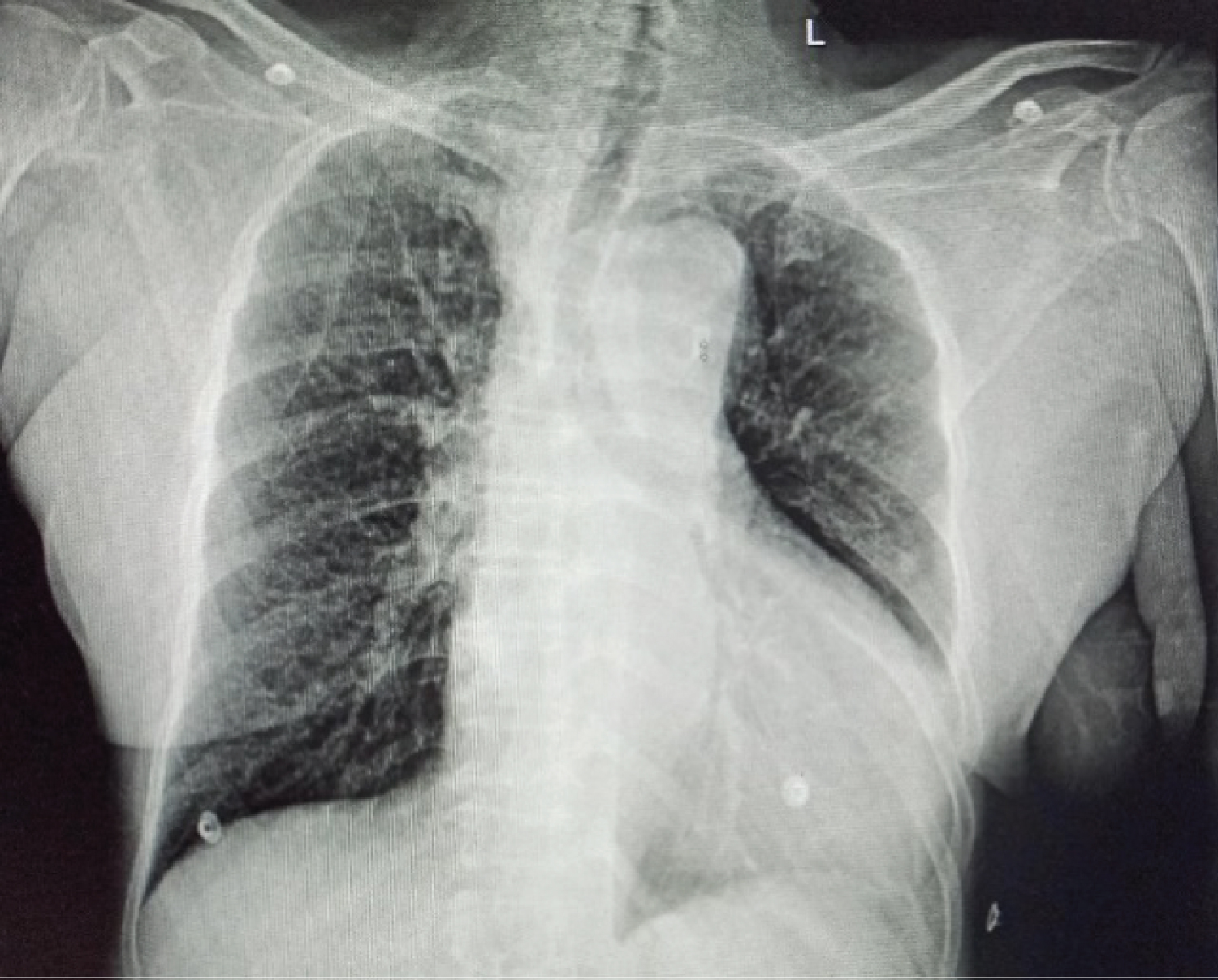 Figure 1: Chest X-ray PA view.
View Figure 1
Figure 1: Chest X-ray PA view.
View Figure 1
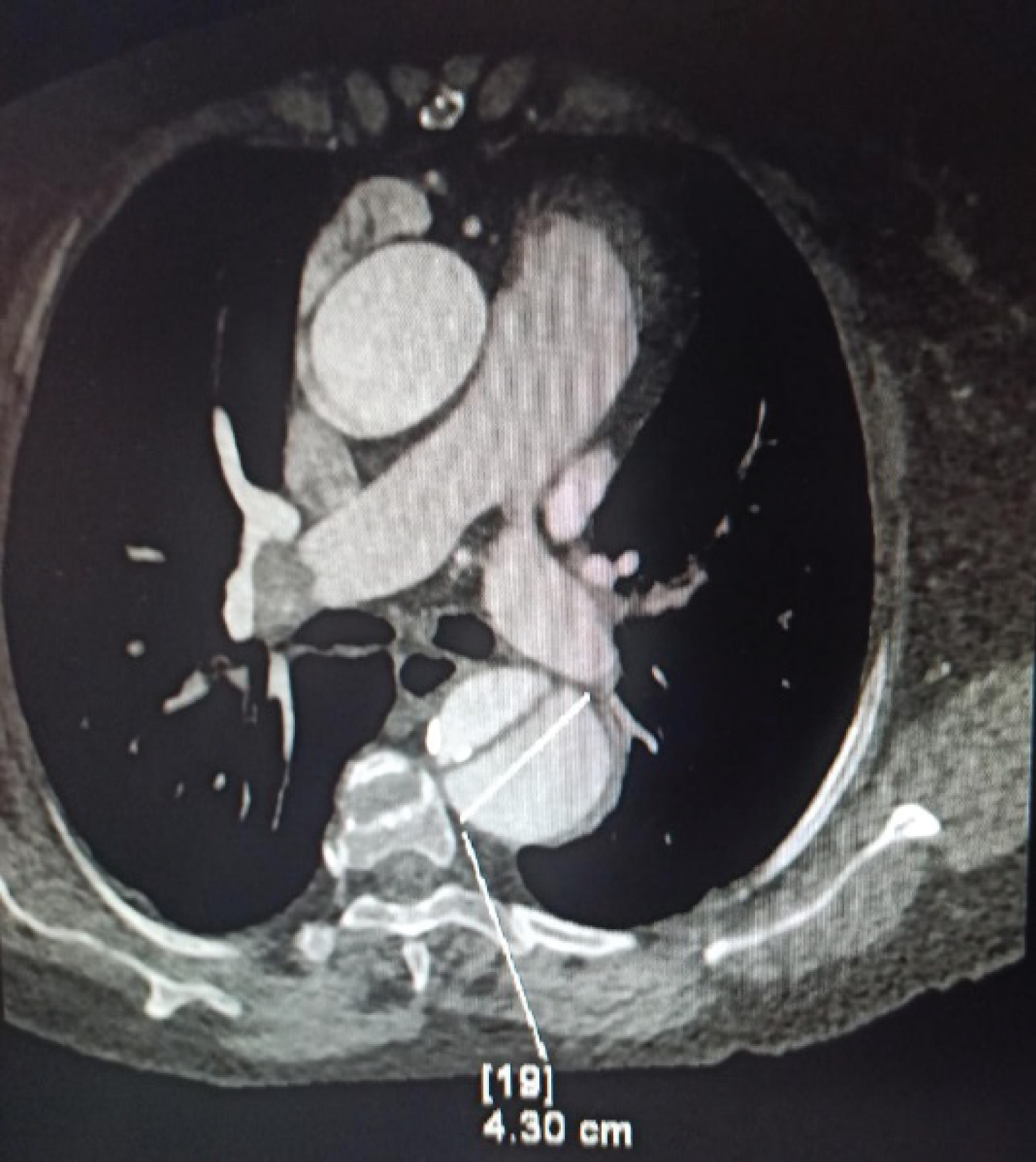 Figure 2: CT angiogram transverse section.
View Figure 2
Figure 2: CT angiogram transverse section.
View Figure 2
A Preoperative anaesthetic check-up of the patient revealed that the patient was a chronic smoker with a pack year of 30, dyspnea on exertion classified under the New York Heart Association (NYHA) as 2, and breath holding time of 13 secs. Other physical and airway examinations were normal. Risk stratifications were performed using the Revised Cardiac Risk Index, which shows an RCRI of 3/6 with ASA physical status classification (ASA-4), a high-risk informed written consent was taken before the procedure. She was advised to take all medications as prescribed except losartan on the morning of surgery.
In the operation theatre, all her baseline data were recorded (HR-88/min, BP - 155/82 mmHg, and SpO 2 -96% on room air). She was premedicated with 1 mg of midazolam and 1g of paracetamol intravenously. The anaesthesia workstation was checked and all necessary medications like esmolol, labetalol, phenylephrine, and ephedrine were kept ready. Her anaesthetic plan consisted of taking a pre-spinal invasive arterial blood pressure (IABP) monitoring followed by a combined spinal-epidural technique. Under local infiltration with 2% lignocaine, her left radial artery was cannulated. Her pre-spinal vitals were BP-142/82 mmHg, HR-80/min. She was given a combine spinal epidural at L3-L4 level with the administration of 12.5 mg of hyperbaric bupivacaine intrathecally. The sensory level of T9-T10 was achieved and surgery was allowed to continue.
After 3 minutes of intra-thecal dosing, her BP decreased from 155/82 to 104/69 and her HR increased from 88/min to 99/min. Phenylephrine boluses in low doses were given (20-40 U) initially followed by infusion to maintain BP within 20% of the patient baseline. No other vasopressors or inotropic agents were required intra-operatively and the surgery went uneventful with blood loss of 100-150 ml only, lasting for 50 min and a total of 1.2-L crystalloids were used. The patient was shifted to recovery for monitoring, later shifted to the ward with an uneventful hospital course and was discharged on the seventh postoperative day. Post-operative pain was managed with epidural morphine 1.5 mg, 12 hourly for 2 days, and 1g acetaminophen 12 hourly.
With the above patient, our main concern was the incidence of acute aortic dissection which can become fatal at any time, during the intraoperative period due to surgical stress and any hemodynamic derangement, leading to sudden death. Aortic dissection is the most common acute aortic syndrome and is considered a medical and surgical emergency. Aortic dissection is classified by Stanford and DeBakey based on its anatomy, as shown in Figure 3 [2]. Type A aortic dissections are always considered a surgical emergency, while type B aortic dissections can be managed conservatively or with selective surgical interventions as the case with our patient [3]. Our patient had an incidental finding of aortic dissection in her regular follow-up echocardiography performed for DCMP. In such asymptomatic cases, echocardiography may not be available for all patients, one may use chest X-rays. In plain radiography, mediastinal widening is the most common abnormality seen in approximately 80% of patients, while other findings include - double aortic contour, irregular aortic contour, or inward displacement of atherosclerotic calcification [4].
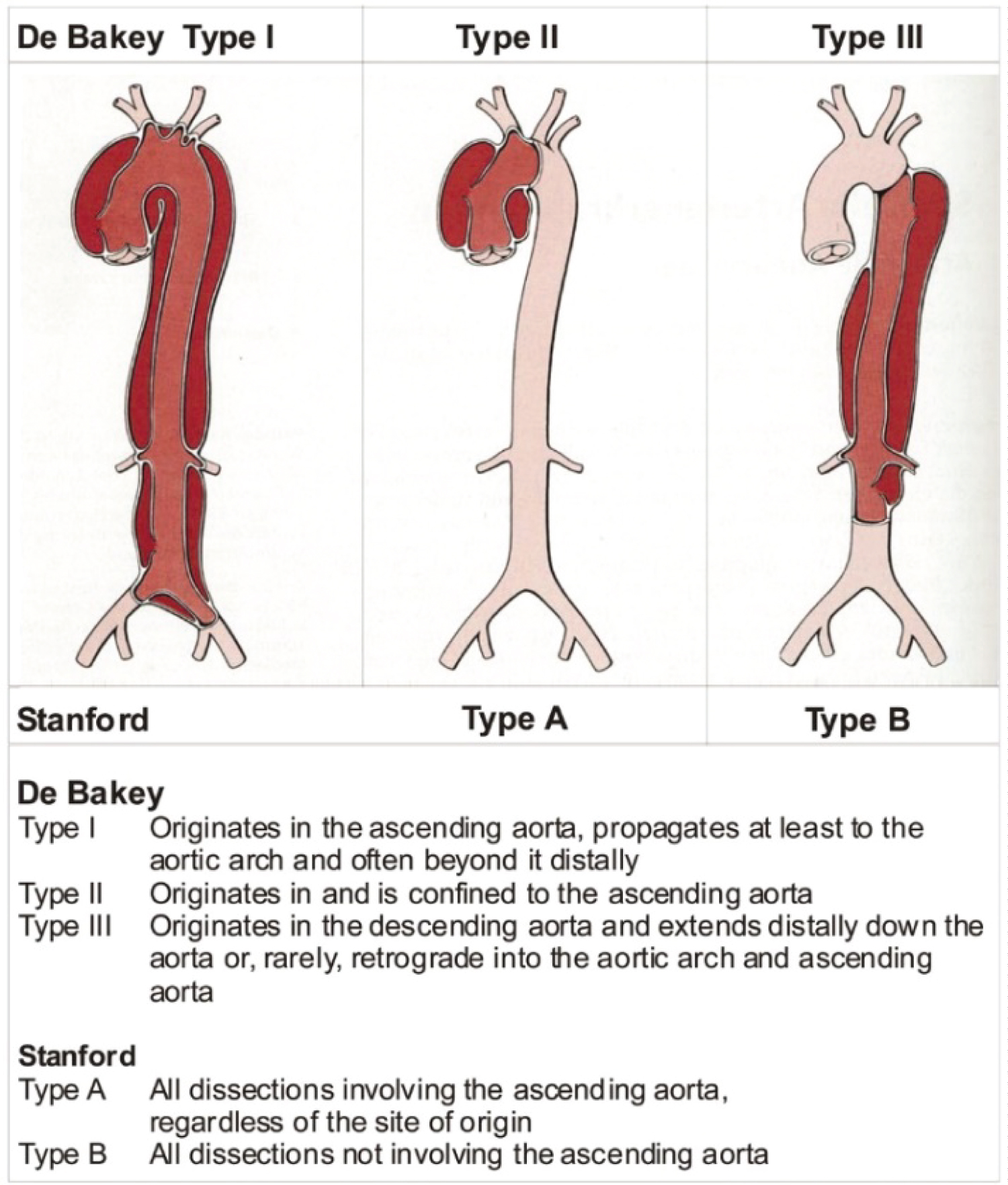 Figure 3: Aortic dissection classification.
View Figure 3
Figure 3: Aortic dissection classification.
View Figure 3
Another concern in our case was the presence of dilated cardiomyopathy, which imposes an increased risk of perioperative arrhythmias, heart failure, and sudden cardiac death. Further, such patients exhibit elevated filling pressures, and impaired myocardial contractility and pose an inverse relationship between the stroke volume and the afterload. Moreover, in this case, cardiothoracic surgeons advised managing this aortic dissection medically seeing her age and the underlying DCMP. But, proceeding with this aortic dissection, patients for non-aneurysmal surgery have a significant risk of aortic rupture and sudden death. And even postponing the case of fracture will keep the patient bedridden causing an inability to do daily routine work, and dependency on other family members and thus increasing the risk of thromboembolism and other complications. Understanding these all patient was taken up for surgery to provide a quality life to her.
Further in our case, apart from the two conditions discussed, she was also a chronic smoker, with a chest x-ray suggestive of COPD. Considering all the above factors, we decided to proceed with the neuraxial technique i.e..., low-dose combined spinal-epidural anesthesia (CSE). In addition to the known advantages of neuraxial over general anesthesia, we wanted to avoid exposure to inhalational agents (myocardial depressants), avoid paralysis and mechanical ventilation (increased risk for perioperative pulmonary complications), reducing afterload (beneficial for both DCMP and aortic dissection. The decision to proceed with titrated doses of combine spinal epidural technique over single-shot spinal anesthesia was taken, to avoid a sudden fall in blood pressure and hemodynamic collapse, as she was a chronic hypertensive patient with a hypertrophied myocardium as it was imperative to maintain the blood pressure within 20% of the baseline values. Moreover, the presence of an epidural catheter helps in postoperative analgesia also and thus helps in reducing the stress on the cardiac workload. In this patient, our target was to maintain the heart rate to < 80/min in view of DCMP, as it not only reduces the risk of life-threatening arrhythmias and improves the NYHA status but also reduces the risk of rupture of aortic dissection. It is also required to maintain a preload without causing fluid overload [5].
Aortic dissection has a considerable risk of fatality. But such patients can be managed with good anesthesia care as well as good planning. The anaesthesiology team should be aware of the varied presentations of aortic dissections and be vigilant in hemodynamic monitoring and management of perioperative care of these patients.