Despite a general reduction in the number of myocardial revascularization surgeries in recent decades, more than 150,000 are still performed annually in the United States. Early complications of venous graft use include an occlusion rate of up to 25% in the first year. The aneurysmal dilatation of the great saphenous vein, when used in aorto-coronary venous bridges, is rare and requires important care by the cardiology team.
This study aimed to present a case report on saphenous vein aneurysm in a patient with coronary artery disease and myocardial ischemia who was diagnosed by angiotomography of the coronary arteries.
The 68-year EDAV patient due to coronary artery disease received saphenous vein grafts. After the last angiotomography of the coronary arteries by computed tomography performed in 2019, May-21, aortic root ectasia, measuring 39 × 40 × 42 mm and Grafted Saphenous Vein Aneurysms (GSVA), and mural atheromatosis of the thoracic aorta were found.
GSVA may present in a heterogeneous way, but are more commonly discovered as an incidental finding in those patients with prior coronary artery bypass grafting. Therefore, there is a paucity of literature to help guide decision-making and the timing of catheter-based interventions.
Coronary artery disease, Cardiac ischemia, Safena, Safene's aneurysm
Despite a general reduction in the total number of myocardial revascularization surgeries in recent decades, more than 150,000 are still performed annually in the United States [1]. Arterial bypass ducts, particularly the left internal mammary artery, are frequently used and have been associated with better patency rates and clinical outcomes compared to patients treated without mammary artery graft [2]. However, the vast majority of patients undergoing myocardial revascularization surgery have at least one Saphenous Vein Graft (SVG) used as a bypass conduit. Early complications of venous graft use include an occlusion rate of up to 25% in the first year [3].
The great saphenous vein is usually used as a conduit in vascular derivations, and is considered, by most surgeons, the best and longest lasting arterial substitute in the infra-inguinal positions. Its degeneration and formation of true aneurysms are extremely rare [1,3,4].
Aneurysmal dilatation of the great saphenous vein, when used in aorto-coronary venous bridges, is a rare event [2]. Most patients develop asymptomatically. They may appear as a pulsatile mass when the graft is in a superficial position. Like true arterial aneurysms, they may present with compressive symptoms. If untreated, true aneurysms of venous graft tend to complicate with their rupture or even formation of fistulas with adjacent organs leading to potentially fatal frames [2].
Late complications include graft degeneration, intimal hyperplasia with resulting graft stenosis, and aneurysm formation [2]. Although degeneration and stenosis are associated with typical symptoms of cardiac ischemia, Grafted Saphenous Vein Aneurysms (GSVA) are generally asymptomatic and are often identified incidentally during imaging for other concerns. Those with symptoms may experience angina, symptoms of compression in the surrounding structures (ie cough), dyspnea, hemoptysis (fistula), orthopnea (hemothorax), or sudden death. Generally defined as a dilation greater than 1.5 times the reference graft vessel, the incidence of GSVA is largely unknown, with reports varying dramatically from as low as 0.07% to as high as 14%. The management of the aneurysms was significant enough to justify that the intervention has been traditionally surgical. However, with the new use of several endovascular pathways [2].
In this sense, as a diagnostic test of this problem, we highlight Coronary Angiotomography (CAT) with important technical advances such as greater axial coverage (from 2 cm to 16 cm) and better temporal resolution, allowing the CAT to become the imaging method noninvasive technique for the diagnosis of artery aneurysms and saphenous vein grafts, with sensitivity and specificity of approximately 95% [5].
Therefore, the present study aimed to present a case report on saphenous vein aneurysm in a patient with coronary artery disease and myocardial ischemia who was diagnosed by angiotomography of the coronary arteries.
The patient EDAV, with 68-years old, due to coronary artery disease received saphenous grafts. After the last angiotomography of the coronary arteries by computed tomography performed in 2019, May-21, aortic root ectasia was measured, measuring 39 × 40 × 42 mm and GASV, as well as mural atheromatosis in the thoracic aorta, as shown in Figures 1, Figure 2 and Figure 3.
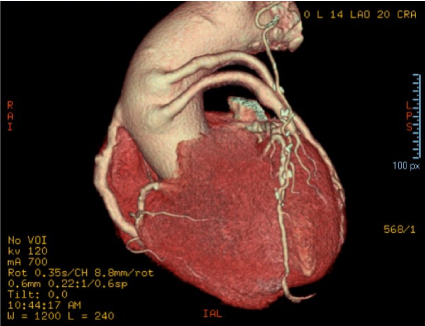 Figure 1: Angiotomography examination of the coronary arteries, showing the saphenous vein aneurysm grafted by the angle of observation 1. View Figure 1
Figure 1: Angiotomography examination of the coronary arteries, showing the saphenous vein aneurysm grafted by the angle of observation 1. View Figure 1
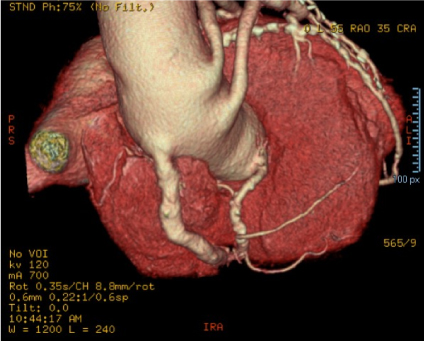 Figure 2: Angiotomography examination of the coronary arteries, showing the saphenous vein aneurysm grafted by the angle of observation 2. View Figure 2
Figure 2: Angiotomography examination of the coronary arteries, showing the saphenous vein aneurysm grafted by the angle of observation 2. View Figure 2
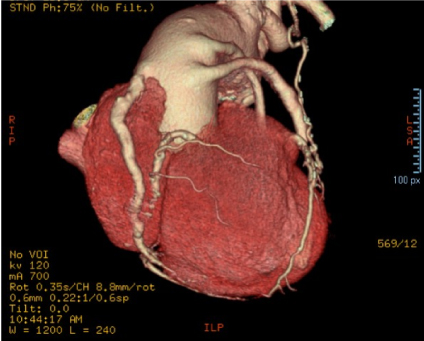 Figure 3: Angiotomography examination of the coronary arteries, showing the saphenous vein aneurysm grafted by the angle of observation 3. View Figure 3
Figure 3: Angiotomography examination of the coronary arteries, showing the saphenous vein aneurysm grafted by the angle of observation 3. View Figure 3
The present case report showed through coronary artery angiotomography examinations that grafted saphenous vein resulted in aneurysmal alterations. The cause of this degeneration still remains unknown, being suggested by some authors as atherosclerotic or as a process of global dilatation of vessels in patients affected [1-3]. In other histopathological studies, proliferative and fibrotic lesions of the intima were noted, leading to weakening of the venous wall and, thus, favoring graft aneurysm formation [2].
In this sense, there is a substantial risk of complications following saphenous graft, including rupture and death, so that surgical or percutaneous treatment may be considered, in particular, in symptomatic patients [2]. One study highlighted three cases highlighting various options and considerations of percutaneous management, including stent placement, coil occlusion, and a combined approach to the use of a peripheral stent. Intervention within this patient population lacks large long-term population outcomes and, as such, should be performed with care by experienced operators [2].
Thus, aneurysms of saphenous vein grafts are rare but are potentially fatal and their ideal management is not clearly established. A case report study of GSVA that was successfully treated with surgical intervention, including aneurysmal resection and re-grafting [6]. The aneurysm detected 36-years after myocardial revascularization surgery was located in the proximal part of the grafted saphenous vein for the posterolateral branch; the left anterior descending coronary artery flow was limited due to compression of the left internal thoracic artery by the adjacent aneurysm. The site of the proximal anastomosis was reconstructed under deep hypothermic circulatory arrest using a pre-sewn vascular prosthesis patch with radial artery graft [6].
In this context, previous data demonstrated that aneurysms over 60 mm in diameter have a combined rate of mechanical complications, rupture, myocardial infarction and death above 50% [7]. However, aneurysms less than 20 mm in diameter had a combined risk of complications approaching 35%, making it very difficult to assess what is and is not a stable or unstable aneurysm. Certainly, once any complication has occurred which can be directly attributed to the aneurysm, intervention is a reasonable option [8]. Given the significant variability in the way, GSVA is diagnosed, at which point the diagnosis is made, and the most common presentation as an incidental finding during other medical care, data are lacking on any correlation between growth rate and risk of rupture [9,10].
Percutaneous management was previously shown as a safe and viable option in a small series of cases (n = 33) [2]. The successful closure of a percutaneous approach can be considered with the placement of an aneurysm exclusion stent or with a coil embolism or Amplatzer implantation device (Abbott) for the occlusion of the aneurysm. There are no published data on large long-term population outcomes [2].
The GSVA may present in a heterogeneous form, but are more commonly discovered as an incidental finding in those patients with prior coronary artery bypass grafting. Once identified, the risk of any complication, including death ranging from 33.3% in small aneurysms to 69.2% in aneurysms with more than 100 mm [2].
Therefore, there is a paucity of literature to help guide decision-making and the timing of catheter-based interventions. The choice of the intervention should be guided by the characteristics of the aneurysm, the venous graft and the relevant myocardial territory. Percutaneous intervention is a safe and viable option for the management of GSVA.
The work was supported by Domingo Braile Institute - São José do Rio Preto - SP, Brazil.
The authors declare no conflict of interest.