Paravalvular leak (PVL) driven intravascular hemolysis (IVH) is a recognized complication of surgical aortic valve replacement. This has been described less following transcatheter aortic valve implantation (TAV). We present a case of a patient with severe life-threatening hemolytic anemia following TAV, requiring multiple blood transfusions, and emergent TAV-in-TAV procedure.
TAV-in-TAV, Hemolytic anemia
AR: Aortic Regurgitation; AVA: Aortic Valve Area; DAT: Direct Antiglobulin Test; IVH: Intravascular Hemolysis; MPG: Mean Pressure Gradient; NYHA: New York Heart Association; PVL: Paravalvular Leak; TAV: Transcatheter Aortic Valve; THV: Transcatheter Heart Valve; TTE: Transthoracic Echo; Vmax: Maximum Velocity
A 77-year-old woman with critical aortic stenosis (Vmax 4.9 m/s, MPG 69 mmHg, AVA 0.5 cm2) (Figure 1A), moderate mitral annular calcification and mild-moderate mitral regurgitation and NYHA class III symptoms was referred for TAVI following Heart team discussion [1]. Annular area measurements were underestimated at the time of the procedure and the patient underwent transfemoral single-access TAVI [2] with a 20 mm balloon-expandable Sapien 3 Ultra prosthesis (Edwards Lifesciences, CA) deployed under rapid pacing. Due to post-deployment asystole and hemodynamic instability requiring a 2-minute cycle of cardiopulmonary resuscitation, the primary operator was disinclined to perform post-dilatation despite the appearances of moderate paravalvular aortic regurgitation (AR) on post-deployment aortogram (Figure 1E and Video 1). Post-procedure transthoracic echocardiography (TTE) confirmed moderate AR and patient was discharged with a view to early follow-up (Figure 1B, Figure 1C and Figure 1D) (Video 2 and Video 3). Within 2 weeks, she was readmitted to the local hospital with symptoms of fatigue, chest pain and NYHA class IV symptoms reporting red-brown urine discoloration. Clinical examination confirmed moderate AR.
Video 1: To show moderate paravalvular aortic regurgitation on a post-deployment aortogram. View Video 1
Video 2: To show moderate paravalvular aortic regurgitation post-TAV on a five-chamber view echocardiogram. View Video 2
Video 3: To show moderate paravalvular aortic regurgitation post-TAV on a short axis view echocardiogram. View Video 3
Sjogren's syndrome, hypothyroidism, blepharitis, hypercholesterolemia.
Blood film demonstrated fragmented red cells on film; and full blood count confirmed normocytic anemia (Hb 78, MCV 94); intravascular hemolysis screen was positive (Ret 135, LDH 2521, Haptoglobin < 0.1, Bilirubin 25, ALT 25, DAT negative), thus meeting criteria for TAVI-induced anemia [3].
• Acquired hemolytic anemia of another etiology: Drug-related etc.
• Heart failure with preserved ejection fraction.
The patient was rapidly transfused 4 units of packed red blood cells (Hb increase to 112) and transferred urgently to our center. Following heart team discussion and repeat CT analysis, annulus area was measured at 323 sqmm and felt to be suitable for TAV-in-TAV with a 23 mm S3 Ultra in the first instance due to significant under sizing of the initial valve. Single access right transfemoral TAV-in-TAV was performed as previously described [2]. In brief, the right common femoral artery micro puncture was performed just proximal to previous access site, with sheath exchanged to deliver 14Fr E-sheath, advanced over Amplatz super-stiff to aorta. The TAV was crossed centrally (confirmed in orthogonal views) with a pigtail catheter. The 23 mm Sapien 3 Ultra system (Edwards Lifesciences, Santa Ana, California) was aligned distally with the original prosthesis (Video 4), to minimize conduction defects and was deployed over 45 seconds under rapid pacing to ensure valve alignment. Post TAVI aortogram and on table TTE confirmed resolution of AR, patent coronary arteries, good valve expansion with no gradient on invasive pullback (Figure 1F, Figure 1G and Video 5). 12 lead ECG remained in sinus rhythm with no change in conduction. There was an immediate resolution (within 24 hours) of symptoms of fatigue, breathlessness, and hemoglobinuria.
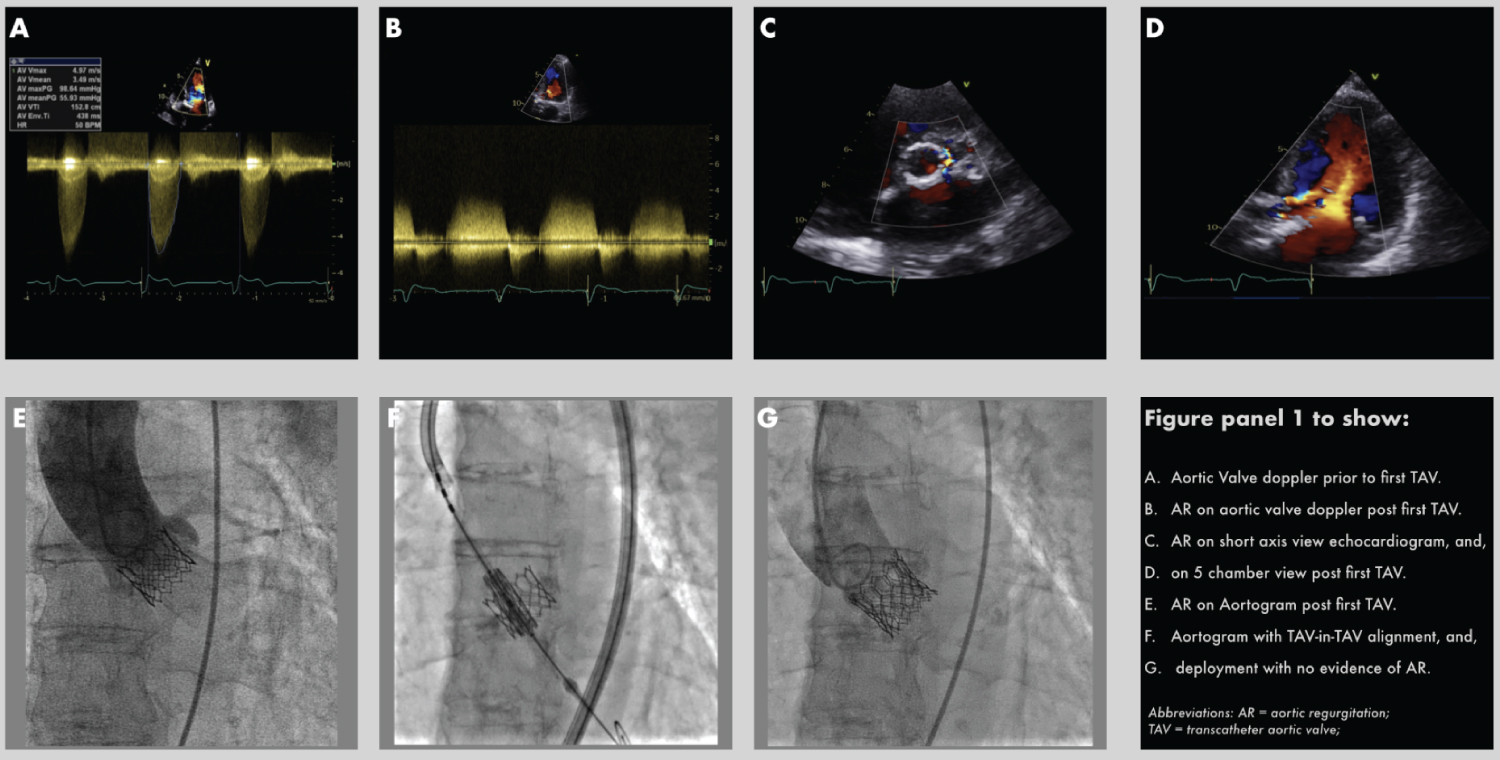 Figure 1: (A) Aortic valve doppler prior to first TAV; (B) AR on aortic valve doppler post first TAV; (C) AR on short axis view echocardiogram, and; (D) On 5 chamber view post first TAV; (E) AR on Aortogram post first TAV; (F) Aortogram with TAV-in-TAV alignment, and; (G) Deployment with no evidence of AR.
Abbreviations: AR: Aortic Regurgitation; TAV: Transcatheter Aortic Valve
View Figure 1
Figure 1: (A) Aortic valve doppler prior to first TAV; (B) AR on aortic valve doppler post first TAV; (C) AR on short axis view echocardiogram, and; (D) On 5 chamber view post first TAV; (E) AR on Aortogram post first TAV; (F) Aortogram with TAV-in-TAV alignment, and; (G) Deployment with no evidence of AR.
Abbreviations: AR: Aortic Regurgitation; TAV: Transcatheter Aortic Valve
View Figure 1
Video 4: To show TAV-in-TAV alignment on a pre-deployment aortogram. View Video 4
Video 5: To show TAV-in-TAV expansion on a post-deployment aortogram. View Video 5
Since the development of 3rd generation TAV devices with sealing skirts, the incidence of PVL has reduced dramatically, however, this less commonly seen complication post-TAV still has important consequences if left untreated. We describe a case of undersized TAV bio prosthesis resulting in profound hemolysis, this IVH was felt secondary to turbulence and shear stress was induced by high velocity moderate PVL [3-5]. In the absence of bicuspid anatomy, or significant calcification, we will advocate selection of a larger size prosthesis if the patient falls between two THV sizes.
1. Recognize IVH as a possible complication of undersized TAV.
2. For patients whose aortic annulus area falls between two THV sizes, consider a choice of a larger size prosthesis to reduce the risk of IVH.