Administration of single dose of ferric carboxymaltose (FCM) is useful for both control of anemia in hemodialysis patients and end stage renal disease. Its use in peritoneal dialysis (PD) patients is not as well known. We report our experience of FCM administration in PD patients.
PD patients treated with i.v. in the last three years in our unit were analyzed retrospectively. Main reasons for administration of i.v. iron therapy were evaluated. Previously oral iron therapy or erythropoietic stimulating agents (ESA) treatment were also evaluated.
Twenty-four PD patients received i.v. FCM. Three received a kidney transplant during the study and one patient did not fulfill 6 months follow-up. Seven patients received oral iron therapy at the beginning and all but four received ESA. The median dose of i.v. FCM was 875 ± 222 mg, without exceeding 15 mg of iron per kg. of body weight. The average hemoglobin at six months increased (baseline: 10.7 ± 1 vs. 11.2 ± 1.1, P < 0.05). Ferritin and TSAT also presented significant differences, baseline: 242 ± 122 vs. 462 ± 252, 20 ± 8 vs. 30 ± 8, respectively, P < 0.01. Hemoglobin < 10 g/dl, serum ferritin levels < 200 ng/ml or TSAT < 20% were the reasons for administration of i.v. FMC. We did not observe statistically significant differences in the dose of ESA despite a reduction in their weekly needs. No side effects were observed whereas FCM was administered. No patients were taken oral iron after FCM.
FCM is an easy alternative to improve the control of anemia in PD patients. In our experience no side effects have been observed in six months. It maintains recommended levels of ferritin at least six months after administration. The requirements of ESA could be reduced.
Iron therapy, Peritoneal dialysis, Anemia, Ferritin
The correct control of anemia in chronic kidney disease (CKD) is one of the main challenges of nephrology. Although its management has been optimized since the emergence of erythropoietic stimulating agents (ESA), some aspects remain elusive. The current guidelines recommend an adequate correction of iron levels to ensure optimal control [1,2]. The ideal form of iron administration in patients with CKD remains unclear and it varies according to the technique of renal replacement therapy (RRT). Intravenous administration is the most used in hemodialysis (HD), however the best iron therapy is more controversial in peritoneal dialysis (PD) [3,4].
PD patients also require strict monitoring of anemia, where successful control of iron levels is crucial [5]. Although current recommendations support the oral correction of iron deficiency, it is not free of limitations. Side effects such as digestive intolerance and the difficulty of bioavailability and absorption, due to their interactions with food, phosphate binders and the lower gastric acidification in renal patients, limit their results [6,7]. In addition, the need for many tablets to achieve objectives, added to other multiple daily treatments, implies a lower therapeutic adherence and is a limitation of its effectiveness. The administration of i.v. iron in PD has been shown to be effective in previous studies, regarding the improvement of hemoglobin levels and the lower requirement of ESA doses [8-12].
Also, taken in consideration that previous studies in HD patients found that mortality was elevated among patients given higher doses of IV iron administration and some lines of evidence indicate that such practices may cause hepatic iron overload, IV iron in PD is unusual [13]. However, its application in PD patients has presented limitations, because of lack of information about the possible side effects and the potential increased risk of infections and death, due to cardiovascular causes [14]. In addition, the ambulatory regimen of PD patients limits the i.v. dosage. The need to perform punctures and more visits to the hospital to reach the correct doses with the classic formulations are obstacles to overcome. New formulations of i.v. iron, such as ferric carboxymaltose (FCM), allow high doses with a single i.v. administration [15]. FCM is a type of i.v. iron with a physiological osmolarity and an almost neutral pH (5.0-7.0), has no cross-reactivity with dextran, the iron-carbohydrate complex is more stable than that of ferric gluconate or iron sucrose, does not require a test dose and several studies in advanced CKD or HD have reported success results with few side effects and high efficacy [16-20].
FCM was included in our unit with the aim of optimizing the control of anemia, reducing the number of pills and decreasing the needs of ESA. Its application in PD patients is less well known and its results have not been widely described. We show the experience of our centre in FCM application in PD patients in our usual clinical practice.
The usual clinical practice in our centre for the control of anemia was that recommended by the current guidelines, with the use of ESA in combination with oral iron therapy, i.v. iron was only occasionally administered [1].
PD patients treated with i.v. FCM in the last three years in our unit were studied retrospectively. All patients older than 18 years in RRT with PD treatment were re-evaluated for i.v. FCM administration. Patients were not indicated for FCM if they had severe liver disease, hypersplenism or had received a blood transfusion in the previous month. Severely malnourished patients or those who had demonstrated sensitivity to iron preparations or had severe inflammation or infection, or malignant tumours were also excluded.
The levels of Hb, hematocrit, TSAT, and ferritin were analyzed from the beginning and every two months. The levels of serum creatinine, urea, total proteins, albumin and serum bicarbonate were also evaluated, according to usual clinical practice. The liver profile, which included alkaline phosphatase, gamma-glutamyl transferase (GGT), aspartate aminotransferase (ASAT) and alanine aminotransferase (ALAT), as well as the bone/mineral metabolism profile, with the levels of serum calcium (Ca), phosphorus (P) and parathormone (PTH), were also analyzed.
The administration of FCM (Ferinject®, Vifor Pharma) in a single dose was carried out in 250 ml of 0.9% sodium chloride solution. At present, FCM is accepted that presented minimal immunogenicity and very limited release of labile iron to the circulation, so a higher dose can be safely administered in a single infusion [21]. The usual dose was 1000 mg, without exceeding 15 mg of iron per kg of body weight. In case of lower weight (< 70 Kg), the total dose was 500 mg. Although the summary of product characteristics (SMPC) states that the infusion time can be 15 minutes, in our unit it was established a time of 60 minutes for the full dose. The administration was carried out by the nurses of the nephrology continuing care unit in a room adjoined to the PD consultation. The dose of i.v. FCM was administered on the same day as the consultation.
Mean and median are shown with standard deviation (SD) and their range respectively. As the data analyzed present a normal distribution (Kolmogorov-Smirnov test), parametric tests were used. Results were compared by Students T test for paired data. The comparison of percentages was made by chi-square test. A P value of less than 0.05 was considered statistically significant.
The demographic data of the patients are shown in Table 1. Twenty-four patients were identified. Four patients did not reach six months of follow-up as three of them received a kidney transplant (KT) and the fourth patient had to transfer to HD due to non-therapeutic compliance. The initial dose of FCM administered was 1000 mg in 16 patients and 500 mg in the rest. There were no adverse reactions to the infusion of the FCM. Delayed affects after 24 hours such as arthralgia and myalgia were not observed. All but one of the patients remained in PD throughout the follow-up. For the final analysis, only the data of the remaining 20 patients have been included. The mean age was 63 ± 12 years. The mean time in PD at the beginning of the study was 10.4 ± 9 (SD) months. Presence of hemoglobin (Hb) levels less than 10 g/dl, serum ferritin levels less than 200 ng/dl and Transferrin Saturation (TSAT) < 20% were reasons for the indication of i.v. FCM in PD patients. After i.v. iron administration, oral iron was suspended. The dose of ESA was adjusted every 2 months with the aim of maintaining Hb levels according to those accepted in the clinical guidelines (11-12 g/dl) [1,2]. The ESA administered in all patients was subcutaneous darbepoetin (Aranesp®, AMGEN).
Table 1: Patient characteristics at baseline. View Table 1
The levels of Hb, hematocrit, TSAT and ferritin are shown in Figure 1. The Hb and hematocrit levels increased with respect to the baseline control and were maintained at six months. Baseline Hb: 10.7 ± 1 g/dl vs. 11.2 ± 1 at 2 months, 11.5 ± 1.3 at 4 months and 11.2 ± 1.1 at six months (P = 0.05, 0.03 and 0.02 respectively versus baseline). Hematocrit levels presented a similar response, baseline hematocrit: 33 ± 3 vs. 35 ± 4 at 2 months, 35 ± 4 at 4 months and 34 ± 4 at six months (P = 0.03, 0.02 and 0.08 with respect to baseline control). The levels of ferritin and TSAT were also increased, with statistical significance throughout all the follow-up with respect to baseline control. The basal ferritin was 242 ± 122, at 2 months: 485 ± 105, at 4 months: 406 ± 165 and at 6 months: 462 ± 252 (P: < 0.001 in all controls). The baseline TSAT was: 20 ± 8, at 2 months: 28 ± 11, at 4 months: 34 ± 16 and at 6 months: 30 ± 8 (P: < 0.001). Weekly doses of ESA were reduced throughout the study but were not statistically significant. Basal dose of ESA: 20 ± 18 mcg/week vs. 15 ± 10 at 2 months, 16 ± 11 at 4 months and 16 ± 12 at 6 months. The rest of the analytical parameters, nor the liver nor the bone metabolism profiles, showed significant changes (Table 2). Table 3 shows several studies with different i.v. iron guidelines in PD.
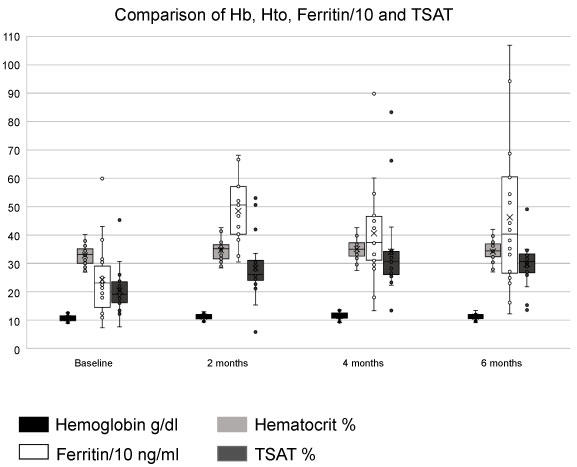 Figure 1: Comparison of hemoglobin (Hb), hematocrit, ferritin, and transferrin saturation (TSAT) at baseline, 2, 4 and 6 months. View Figure 1
Figure 1: Comparison of hemoglobin (Hb), hematocrit, ferritin, and transferrin saturation (TSAT) at baseline, 2, 4 and 6 months. View Figure 1
Table 2: Baseline, 2, 4 and 6 months parameters. View Table 2
Table 3: Different studies with i.v. iron therapy in PD patients. View Table 3
Two patients received a new dose of i.v. iron before 6 months, in one case due to persistence of high levels of resistance to erythropoietin and in the another patient due to clinical worsening and Hb levels < 10 g/dl. No patient required transfusions in the follow-up period.
Anemia management in patients with renal disease remains a critical clinical issue [22,23]. PD patients require supplemental iron to maintain a response to erythropoietin, even more with the increasing emerging concerns of stroke, thrombosis, and cancer risk with the liberal use of ESAs [24,25]. In our unit, given the well-known oral iron inconveniences, i.v. administration of iron with FCM was introduced. Our results show a favorable analytical response, with absence of immediate complications.
The formulation of iron is usually based on local recommendations and clinician preferences. Oral iron absorption is markedly impaired in PD patients as compared with healthy control subjects [26]. Although the guidelines suggests oral treatment is acceptable, i.v. treatment has demonstrated better results. The effectiveness of oral iron supplements is limited by poor bioavailability, poor patient compliance due to gastrointestinal side effects, the need to time the medication away from meals, and the magnitude of the iron deficiency in PD. Nevertheless, there are well described risk with parenteral iron preparations, acute anaphylactic, labile iron reactions, effects of oxidative stress, possible increased risk of infections, risk of vascular calcifications, and risk of iron overload [27,28]. FCM iv-treatment option was included because of the potential benefits, contrasted in previous studies in renal patients [15-17]. As in these studies, in the non-dialysis and hemodialysis population, we have also observed an increase in the levels of Hb, hematocrit, ferritin and TSAT.
The results with i.v. iron in PD are scarce and with methodological limitations. Richardson, et al. administered sucrose iron to 81 PD patients and, although there was not control group, they observed a favorable response of Hb and ferritin levels, but not in reduction of ESA requirements after a follow-up of 13 months [29]. The same results were found in other studies (Table 3) [5,10,30-32]. In contrast, Ahsan, et al., in their studies in 1998 and in 2000, observed an increase in analytical parameters and a reduction in the needs of ESA [33,34]. We have also observed a favourable analytical response, but we have been unable to demonstrate statistical significance in the reduction of ESA. Although the tendency is to decrease the requirements, our sample is probably not of sufficient size for definite confirmation.
Another relevant aspect is the form of i.v. iron administration. To date, the iv-iron prescribed in other studies required trial doses and was not free of risk of anaphylaxis, with the need for administration of a prophylaxis. Ahsan, et al., administered iron dextran in 13 patients on PD, and their protocol included prophylaxis prior to i.v. iron administration [29]. In the study of Li, et al., with sucrose iron or that of Prakash, et al. with saccharate iron, a trial dose was given before the full dose [8,10]. Fear of adverse reactions has precluded administration of large doses of parenteral iron, and oral iron continues to be the common form of therapy in PD patients despite its marginal efficacy. However, Solak, et al. showed in 167 PD patients that iron dextran administration had a safety profile similar to that of sucrose iron with conventional precautions [35]. FCM did not require a trial dose and prophylaxis prior to infusion should not be performed in our series. Our results are similar with the showed in the study of Sivakumar, et al., Treatment of Iron Deficiency Anemia (FIRM) study, Ferumoxytol versus Ferric Carboxymaltose, demonstrated a 0.6% - 0.7% incidence of moderate to severe hypersensitivity reactions with exposure of 1,997 patients to ferric carboxymaltose or ferumoxytol [36,37].
In short, FCM configuration allows a high dose in a single dose, with fewer punctures and a shorter administration time, quickly reaching recommended levels, as a recent meta-analyzes has demonstrated in HD and CKD stages 3-5 [38].
Apart from the well-known described immediate effects and the need for loading doses in the classic formulations of i.v. iron, many doubts persist about the suitability of its administration. Although the activation of the inflammatory response is different according to the iron modality, the potential long-term repercussions require a cautious attitude with them all. Several studies suggest intravenous iron treatment produces oxidative stress, increasing levels of lipid peroxidation products in plasma due to a direct effect of iron sucrose [39]. Nevertheless, FCM has showed less inflammatory activity. Prats, et al. showed in their study in 45 predialysis CKD patients treated with high doses of FCM that FCM has no proinflammatory effect and does not alter levels of adhesion molecules [40]. In our study, this issue is not analyzed due to the impossibility of carrying out these tests. In contrast, we reviewed the levels of phosphorus, since in several studies of FCM administration in anemia patients with normal renal function, a tendency to a hypophosphatemia has been observed [41]. We did not observe hypophosphatemia, as in other studies of FCM in the renal population [19,42].
Our study presents the limitations of a retrospective study, without a control group and with a reduced number of patients. In turn, the criteria for follow-up and control of iron deficiency have been classically described as ferritin and TSAT, which have already known limitations [43,44]. However, the study describes six months follow-up of the experience of FCM application in a PD unit during the last three years. Although the application of FCM in patients on ESRD is not new, as far as we know our experience is the first one described in PD patients.
FCM is effective to reduce the iron deficiency in patients in HD and in a CKD stage 3-5. Its administration in PD patients seems to show efficacy, without evidenced side effects, at least in the short term. Larger and longer-term studies are necessary to confirm safety of i.v. iron therapy in this population. Although further studies are required to documented long-term safety, FCM may be considered in PD patients. Its application on a regular basis must be re-evaluated individually, given the lower experience in PD.