The aim of the present study was to compare of the effects of different dialysis modalities on the short-term survival rate of hemodialysis patients with AMI. We retrospectively analyzed 68 hemodialysis patients with AMI between January 2014 and April 2023. General clinical information were collected from patients. Kaplan-Meier plots was employed to analyze the impact of different dialysis modalities on short-term survival rate. Risk factors for short-term mortality rate were further analyzed using logistic regression. There was a statistically significant difference in survival at 14 days (22.22% vs. 60.98%, P = 0.0016), 30 days (51.85% vs. 70.73%, P = 0.0183) and 60 days (59.26% vs. 73.17%, P = 0.0335) between continuous venovenous hemofiltration (CVVH) modality and intermittent hemodialysis (IHD) modality. Our results indicate that CVVH modality may improve short-term survival rate of hemodialysis patients with AMI.
The incidence of cardiovascular disease in chronic kidney disease (CKD) patients is high, and the mortality rate caused by cardiovascular disease in dialysis patients is 10 to 30 times higher than in the general population [1]. Acute myocardial infarction (AMI) in dialysis patients is a catastrophic event associated with poor long-term survival. Previous reports have shown that the 1-year mortality rate of dialysis patients in the United States due to AMI is 59%, and the 2-year mortality rate is 73%. Even after reperfusion therapy, the 2-year mortality rate of AMI in dialysis patients is still 73% [2,3].
To date, there is a paucity of data concerning the impact of dialysis modalities on the prognosis of dialysis patients with AMI. K/DOQI Clinical Practice Guidelines point out that dialysis prescriptions should be adjusted to maximize benefits while reducing the risk of hypotension during this vulnerable period in the first 48 hours after AMI [4]. Due to the better hemodynamic stability of continuous renal replacement therapy (CRRT) compared to intermittent hemodialysis (IHD), and the fact that serum electrolyte does not under large fluctuations during CRRT, We switched the modality of first dialysis session for hemodialysis patients with AMI to continuous venovenous hemofiltration (CVVH) to minimize the impact of treatment on the patient's myocardial ischemia.
In this study, we reviewed the clinical data of hemodialysis patients with AMI in our hospital since 2014, analyzed the impact of different dialysis modalities on the risk of mortality, and explored the most suitable dialysis modalities for hemodialysis patients with AMI.
This study was approved by the Ethical Committee of the The Chonggang General Hospital Affiliated to Chongqing University of Posts and Telecommunications (ethics No.: 2023-SY-01). Written informed consent was waived duo to the retrospective study design and approved by Ethical Committee of the The Chonggang General Hospital Affiliated to Chongqing University of Posts and Telecommunications. We confirm that all experiments of the study were performed in accordance with relevant guidelines and regulations. The diagnosis of AMI required the following criteria: Symptoms were consistent with AMI, cardiac enzymes were elevated including Troponin I and/or creatinine kinase (at least a two-fold increase from the normal upper limit), and ST-segment elevation or depression in electrocar diograms compatible with AMI. In addition, the diagnosis of ST segment elevation AMI was defined as a new ST segment elevation at point J in at least 2 consecutive leads of 2 mm (0.2 mV); All others were defined as having no ST segment elevation.
Eligible patients were aged ≥ 18 years and were on hemodialysis for End stage renal disease (ESRD) ≥ 3 months. After the onset of AMI, all patients received appropriate treatment according to the requirements of the K/DOQI Clinical Practice Guidelines, including antiplatelet agents (aspirin and clopidogrel), beta blockers, angiotensin converting enzyme (ACE) inhibitors or angiotensin type-1 (AT1) receiver blockers and antibiotic therapy [4]. After communicating the necessity to patients and their families, PCI was performed according to their decision. Although there are no clear guidelines on which treatment modality is beneficial for hemodialysis patients with AMI, the Japanese Clinical Practice Guideline for acute kidney injury suggests that CRRT is more effective than IHD in critically ill AKI patients with hemodynamic instability [5]. Therefore, we attempted to use CVVH modality in the first dialysis session of hemodialysis patients with AMI, hoping to improve the prognosis of such patients. For dialysis patients with AMI, the treatment modality before 31 March 2020 was to continue IHD; After 1 April 2020, CVVH modality was employed for the first dialysis session (if the patient agreed) and then switched to IHD.
Hemodialysis patients with AMI between January 2014 and April 2023 were initially screened for enrollment in the retrospective study. Of the total 89 hemodialysis patients, Patients with malignant tumors, decompensated liver cirrhosis, lupus nephritis, crescentic glomerulonephritis, cardiogenic shock, sepsis, gastrointestinal bleeding, and the need for mechanical ventilation were excluded. Finally, 68 patients were enrolled.
Data are presented as mean ± standard deviation (SD) for normally distributed variables or median [IQR] for non-normally distributed variables. The normality of the distribution was determined using the Shapiro-Wilk test. Two continuous variables were compared using the unpaired T-test (normal distribution) or non-parametric test (Skewed distribution). χ 2 test or Fisher's exact test was utilized for categorical comparisons. Kaplan-Meier plots were utilized to assess survival impact over time. Logistic regression analysis was employed to further identify the factors affecting survival rate. A p value < 0.05 was considered statistically significant. All computations were performed using the SPSS 20.0 software (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp).
Shapiro-Wilk test showed that age, hemoglobin and albumin at the onset of AMI are normal distribution, and dialysis age are skewed distribution. There was no significant difference between CVVH and IHD groups in age (69.78 vs. 71.81, T-test, p = 0.317), dialysis age (42.89 vs. 33.65, Mann-Whitney U test, p = 0.221), sex (χ 2 test, p = 0.764), hemoglobin (101.00 g/L vs. 98.37 g/L, T-test, p = 0.801), albumin (36.68 g/L vs. 35.8 g/L, T-test, p = 0.294), vascular access (Fisher's exact test, p = 0.514), prevalence of diabetes (χ 2 test, p = 0.421), and prevalence of hypertension (Fisher's exact test, p = 0.421) , but the proportion of patients with ST elevation AMI in CVVH group was higher (χ 2 test, p = 0.002) (Table 1).
Table 1: Demographics. View Table 1
When comparing patients treated with CVVH versus IHD, there was a statistically significant difference in survival at 14 days (22.22% vs. 60.98%, P = 0.0016), 30 days (51.85% vs. 70.73%, P = 0.0183) and 60 days (59.26% vs. 73.17%, P = 0.0335) (Figure 1, Figure 2 and Figure 3). Logistic regression analysis further confirmed that the choice of first dialysis modality after AMI had a significant impact on the 14 days survival rate. Compared with CVVH, continuing to use IHD modality during the first dialysis session after AMI could increase the risk of death for hemodialysis patients within 14 days after the onset of AMI by 4.2 times (OR, 5.209; 95% CI, 4.6 to 6.0; P < 0.001). In addition, the age of the patient and the hemoglobin level at the time of AMI onset also had a significant impact on the 14 day survival rate. For every year of age increase, the risk of death within 14 days after the onset of AMI increased by 3.2%, while for every 10 g/L increase in hemoglobin, the risk of death within 14 days after the onset of AMI was reduced by 7%. No significant impacts of dialysis age or albumin level on short-term survival were found in this study (Table 2).
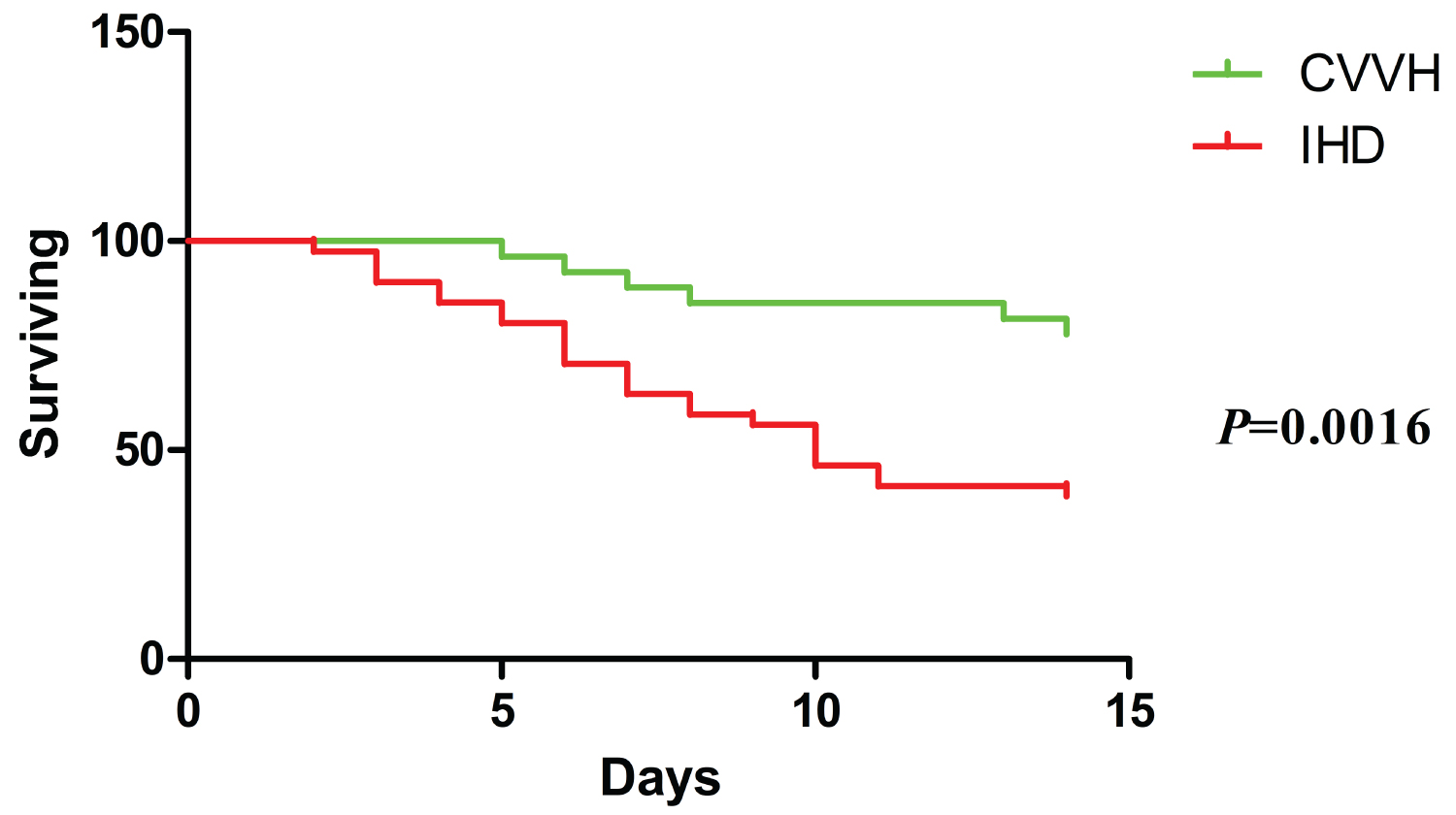 Figure 1: Kaplan-Meier analysis of patients with AMI at 14 days comparing survival of patients receiving CVVH to IHD. AMI: Acute Myocardial Infarction; CVVH: Continuous Venovenous Hemofiltration; IHD: Intermittent Hemodialysis.
View Figure 1
Figure 1: Kaplan-Meier analysis of patients with AMI at 14 days comparing survival of patients receiving CVVH to IHD. AMI: Acute Myocardial Infarction; CVVH: Continuous Venovenous Hemofiltration; IHD: Intermittent Hemodialysis.
View Figure 1
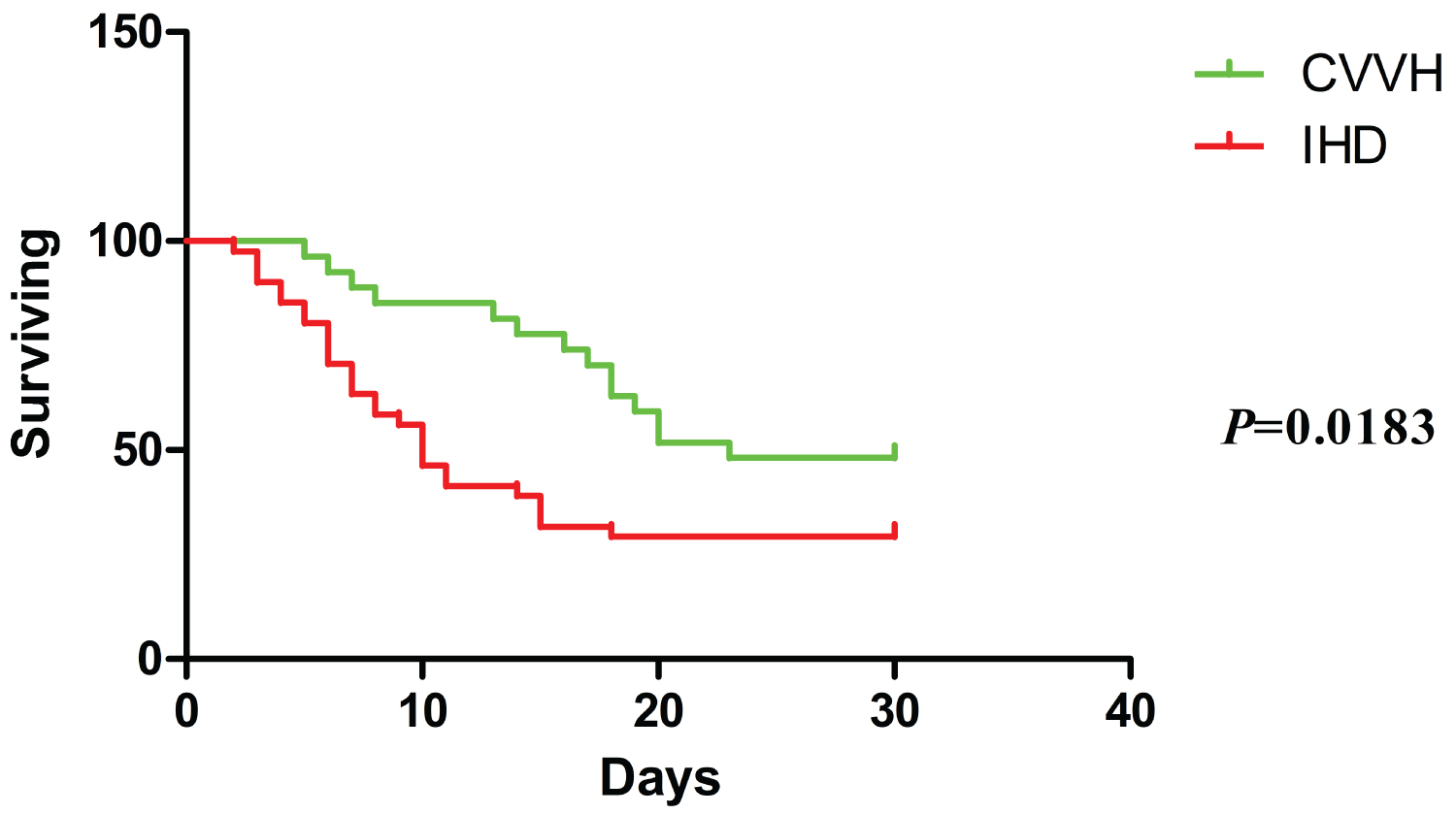 Figure 2: Kaplan-Meier analysis of patients with AMI at 30 days comparing survival of patients receiving CVVH to IHD. AMI: Acute Myocardial Infarction; CVVH: Continuous Venovenous Hemofiltration; IHD: Intermittent Hemodialysis.
View Figure 2
Figure 2: Kaplan-Meier analysis of patients with AMI at 30 days comparing survival of patients receiving CVVH to IHD. AMI: Acute Myocardial Infarction; CVVH: Continuous Venovenous Hemofiltration; IHD: Intermittent Hemodialysis.
View Figure 2
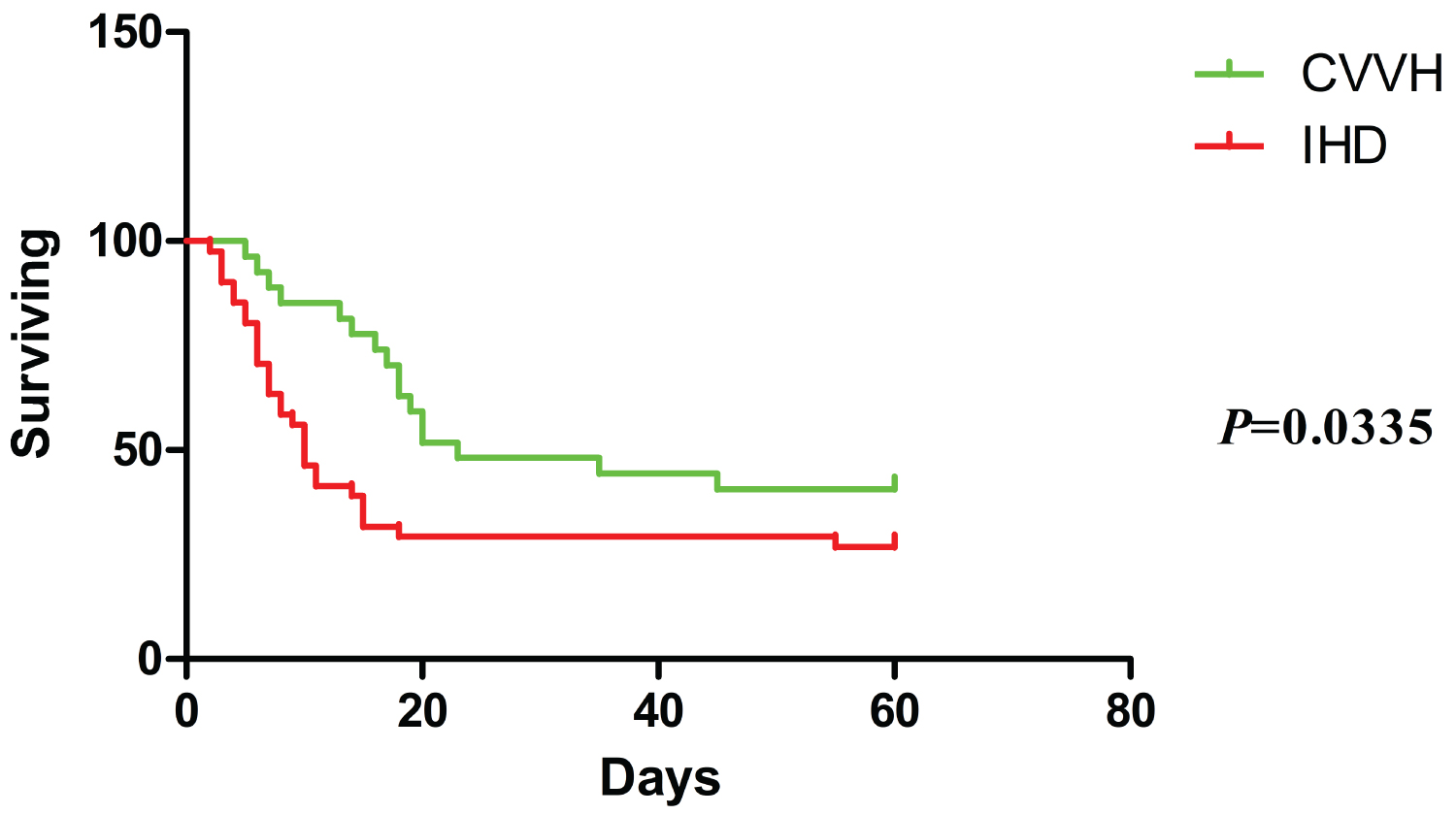 Figure 3: Kaplan-Meier analysis of patients with AMI at 60 days comparing survival of patients receiving CVVH to IHD. AMI: Acute Myocardial Infarction; CVVH: Continuous Venovenous Hemofiltration; IHD: Intermittent Hemodialysis.
View Figure 3
Figure 3: Kaplan-Meier analysis of patients with AMI at 60 days comparing survival of patients receiving CVVH to IHD. AMI: Acute Myocardial Infarction; CVVH: Continuous Venovenous Hemofiltration; IHD: Intermittent Hemodialysis.
View Figure 3
Table 2: The result of logistic regression analysis. View Table 2
This study investigated the effects of CVVH and IHD on the survival rates at 14, 30, and 60 days after onset of AMI in hemodialysis patients. Our results indicated that the dialysis modality chosen during the first dialysis session had a significant impact on the short-term survival rate of hemodialysis patients with AMI. The usage of CVVH modality (even if performed only once) could significantly improve the survival rate of dialysis patients at 14, 30, and 60 days after AMI.
IHD involves faster fluid and solute removal rates. This rapid clearance speed often exacerbates the instability of hemodynamics [6,7]. Several studies targeting renal failure patients treated with hemodialysis have shown that higher ultrafiltration rates might be associated with an increased risk of intradialytic hypotension, decreased microcirculatory blood flow and hypoperfusion of the heart, brain, kidneys and gastrointestinal tract [8-11]. CVVH involves the slow and continuous removal of water and solutes from plasma, and is currently the preferred method for treating patients with hemodynamic instability [7,12]. Therefore, theoretically, the CVVH may be more suitable for patients with organ ischemia.
Researches have also shown that dialysis treatment-related issues play a crucial role in the occurrence of sudden cardiac death, especially in patients with AMI, where the probability of sudden death is higher [13,14]. One of the reasons for dialysis treatment-related cardiac death is the fluctuation of serum potassium concentration during dialysis treatment. IHD restores potassium balance by removing potassium rapidly using dialysate baths with lower potassium levels. However, the use of 2 meq/L potassium dialysate (conventional potassium concentration) increases the risk of cardiac death in dialysis patients, especially in patients with AMI, who has a increased risk of malignant arrhythmias under low potassium conditions [15,16]. The potassium concentration in the replacement fluids used by CVVH is generally set at 4 meq/L, so hypokalemia will not occur during treatment. Therefore, during CVVH treatment, the probability of patients experiencing malignant arrhythmia or sudden cardiac death is greatly reduced.
Although multiple large-scale clinical studies have not found that CVVH is superior to IHD in improving the survival rate of critic patients with AKI [17-20]. However, survival may be improved if CVVH is chosen as the preferred modality in specific patient groups [21].
Generally speaking, the treatment time of CVVH needs to last for more than 24 hours, but prolonged overall treatment time will inevitably places a greater burden on the medical staff and poses a higher risk of hemorrhage and economic costs on patients than IHD [5]. Our results indicated that selecting the modality of CVVH for the first dialysis session after AMI, followed by switching to conventional dialysis treatment, not only significantly improved the short-term survival rate of dialysis patients, but also optimized medical resources and reduced the economic burden on patients.
Although the survival rate of patients treated with CVVH were still better than those of treated with IHD at 30 and 60 days, the benefits had already diminished compared to 14 days. In contrast, patients treated with IHD had the highest risk of mortality within 14 days, while survival rates at 30 and 60 days showed only a slight decrease. We are currently unable to fully explain this phenomenon. We speculated that the vast majority of critically ill patients treated with IHD had already died within the first 14 days, so the risk of death did not further increase in the following 30 and 60 days. Among patients treated with CVVH, the survival time of critically ill patients was briefly prolonged due to the better hemodynamic and electrolyte stability of CVVH. Later, due to the conversion of dialysis modality to IHD, the risk of mortality increased again, leading to a delay in the peak time of mortality in the CVVH group. Compared with our current treatment protocol, appropriately increasing the number of CVVH treatments after AMI may further improve the survival rate of dialysis patients, but it remains challenging in routine clinical practice to perform CVVH, especially in non-ICU units due to continuous treatment for more than 24 hours and expensive costs. Therefore, bridging the treatment gap with sustained low efficiency dialysis (SLED) may be a more reasonable treatment option and we will observe the efficacy of this method in future work.
It is worth emphasizing that there are several limitations to our study. First, although our research results showed that short-term survival rate of the CVVH group was better than that of the IHD group, we were unable to distinguish the severity of coronary artery disease between the two groups. In fact, there is currently a lack of effective methods for quantitative scoring of coronary artery disease internationally, which may resulting a problem of baseline imbalance. Second, choosing CVVH modality often meant that family members had a stronger willingness to treat, better economic conditions and greater support for patients, which may affect patients prognosis. Third, in this study, very few patients (3/68) underwent percutaneous coronary intervention (PCI). In fact, effective revascularization therapy could lead to lower risk of in-hospital mortality in HD patients after AMI [22]. Therefore, it is unclear whether our results can be applied to all hemodialysis patients with AMI.
In conclusion, to the best of our knowledge, the present study for the first time reveals that the CVVH modality may improve short-term survival rate of hemodialysis patients with AMI. Therefore, on the basis of sufficient drug treatment for patients, choosing CVVH modality as much as possible may improve their prognosis.
Not applicable.
No funding was received.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
JH designed the study and collected the data, analysis of the data and writing the manuscript with assistance of CM and FW. All authors have read and approved the final manuscript.
This study was approved by the Ethical Committee of the The Chonggang General Hospital Affiliated to Chongqing University of Posts and Telecommunications (ethics No.: 2023-SY-01).
Written informed consent was waived duo to the retrospective study design and approved by Ethical Committee of the The Chonggang General Hospital Affiliated to Chongqing University of Posts and Telecommunications.
The authors declare that they have no competing interests.
None.