Neonatal sepsis is an independent risk factor for the development of central nervous system injury, so preterm newborn, who is more exposed to infections, has a higher neurological risk. This research wanted to examine whether and how sepsis could influence preterm newborns' neurodevelopmental outcome.
We conducted an observational retrospective study with case-control design, recruiting preterm infants with gestational age ≤ 32 weeks or birth weight ≤ 1500 g. 42 patients joined the study, 21 with diagnosis of sepsis (cases: with sepsis) and 21 without infections (controls: no sepsis). We compared the two groups (no sepsis; with sepsis) means with regard to the auxological and neurodevelopmental outcomes.
Neuroimaging and neurodevelopmental outcome data analysis shows that the comparison between the means in the 2 groups (no sepsis; with sepsis) was statistically significant (p-value < 0.05).
The results prove the role of sepsis in determining a greater neurocognitive impairment in this category of newborns. Anyway, this is a preliminary research which needs to be supported by further studies with a larger cross-section to confirm the hypothesis.
Preterm, Newborn, Sepsis, Follow-up, Neurodevelopmental outcome
VLBW: Very Low Birth Weight; AOUP: Azienda Ospedialiera-Universitaria Pisana; NICU: Neonatal Intensive Care Unit; EOS: Early-Onset Sepsis; LOS: Late-Onset Sepsis; SGA: Small for Gestational Age; BPD: Bronchopulmonary Dysplasia; NEC: Necrotizing Enterocolitis; CVC: Central Venous Catheter; CRP: C Reactive Protein; sd: Standard Deviation; PVL: Periventricular Leukomalacia
Today prematurity is still a topical and globally discussed issue: 15 million preterm infants are born every year in the world and about 1 million of them dies because of the complications linked to preterm birth [1]. In developed countries the largest part of these newborns survives but, because of the complications due to organs and tissues incomplete maturation, there is a high risk of developing long term disabilities [2]. In particular the studies in literature confirm that preterm neurodevelopmental outcome has greater problems compared to term infants [3,4], especially for babies born under 32 weeks of gestational age or those with birth weight under 1500 g (very low birth weight, VLBW).
Looking at the immune system, preterm birth entails a development deficit in all its parts (innate, specific and passively acquired immunity) and that means they have a greater predisposition for the development of infections which can be vertically transmitted from mothers during pregnancy or delivery or horizontally transmitted in NICU for invasive procedures [5]. Sepsis can represent a further risk factor for the development of central nervous system injury [6,7], because the systemic inflammatory state due to infection increases the oxidative stress in cells and in particular in the white matter, where the maturation of neurons and the myelination process interrupt [8].
Our research, conducted at the Neonatal Intensive Care and Neonatology Unit, Azienda Ospedaliera-Universitaria Pisana (AOUP), Pisa, wanted to explore whether and how neonatal sepsis could further worsen auxological and neurodevelopmental outcome in a population of preterm newborns with gestational age under 32 weeks or birth weight under 1500 g, monitoring their time trend through clinical follow-up as suggested by international follow-up networks whose studies are specific for preterm newborns [9]. In our Unit, neonatologists and child neuropsychiatrists examined auxological and neurodevelopmental outcomes in preterm infants and they followed international protocols for follow-up such as the Hammersmith Neurological Examination for the evaluation of psychomotor and neurological development [10].
The method we chose for this study was the epidemiologic observational retrospective one with case- control design: we compared 2 groups of preterm infants, the ones who presented sepsis during the hospitalization in the Neonatal Intensive Care Unit (NICU) (cases) and the ones who had not any infectious episode (controls).
The patients were selected analysing the medical records of infants who were hospitalized in NICU of AOUP born in the period between January 2014 and June 2016 with gestational age under 32 weeks or birth weight under 1500 g.
We examined 81 medical records of patients from our NICU, but we excluded 39 of them: 13 patients who died during the hospitalization, 19 who didn't observe the follow-up program and 7 cases of uncertain diagnosis of sepsis (i.e. with non-specific symptoms and negative blood tests and cultures). At least we included 42 patients in our research, 21 with diagnosis of sepsis (cases) and 21 without any infection (controls). Among the group of 21 patients with sepsis, we found out 7 cases of early- onset proven sepsis (EOS), 1 case of early-onset clinical sepsis (i.e. a clinical scenario which suggests the presence of sepsis, with altered indicators of systemic inflammation but negative cultures; temporally, it can be both early-onset and late-onset sepsis), 8 cases of late-onset proven sepsis (LOS) and 5 cases of late-onset clinical sepsis. The pathogenic microorganisms we most frequently found through cultures were Group B Streptococcus for EOS and Klebsiella pneumoniae for LOS. Moreover we analysed medical records of selected patients who were examined in follow-up clinics: in fact, after discharge, patients who present neurodevelopmental risk factors are included in a follow- up care program which establishes the periods for the execution of in-series examinations to monitor the auxological and neurocognitive development at 1, 3, 6, 12, 18 e 24 months' corrected age.
The variables analysed for each patient were:
- Physiological variables: gender, gestational age, birth weight, number of small for gestational age (SGA) infants (SGA: by the 10th percentile in Italian Neonatal Study growth charts), Apgar score at 5 minutes after birth;
- Comorbidities: presence of neonatal respiratory distress syndrome, patent ductus arteriosus, bronchopulmonary dysplasia (BPD), necrotizing enterocolitis (NEC);
- Hospitalization data: weight and cranic circumference at discharge, days of hospitalization, delivery room endotracheal intubation, days of mechanical ventilation, number of central venous catheter (CVC) changes, C reactive protein (CRP) measurement at time 0 (time of birth for EOS and time of sepsis diagnosis for LOS) and after 48 hours;
- Imaging: cranic ultrasonography scans. We performed 2 scans for each patient who joined the study, the first at time 0 (time of birth for EOS and time of sepsis diagnosis for LOS) and the second after 15 days from the first one. Three neonatologists performed the scans in our NICU and they referred to De Vries' score [11] for the evaluation of brain injury: this score is useful to assess the presence of periventricular leukomalacia (PVL) which is the most common form of brain injury in preterm newborns. The score we used for the scan assessment is showed in Table 1.
Table 1: Score for the assessment of ultrasound scans at time 0 and time 1 (after 15 days). View Table 1
- Follow-up clinics data: auxological development evaluation in terms of weight and cranic circumference at 12 and at 24 months' corrected age performed by neonatologists; overall neurodevelopmental outcome at 1, 3, 6, 12, 18 e 24 months' corrected age follow-up examinations. For the evaluation of neurodevelopmental outcome, we considered psychomotor development, neurological examination, vision and hearing assessment for each examination. The assessment of psychomotor development and neurological examination was performed by 3 child neuropsychiatrists who followed the Hammersmith neurological examination (Hammersmith Neonatal Neurological Examination for newborns and Hammersmith Infant Neurological Examination from 2 to 24 months' corrected age) [10] to evaluate these 2 areas: in fact, the international follow-up networks recommend a "comprehensive neurodevelopmental assessment" [9] to perform an all-inclusive examination looking at the different steps children are supposed to achieve at different ages. For the psychomotor area, we established a score considering the most important abilities (among gross motor, fine motor, adaptive, cognitive and language skills) for each age of examination: we choose 6 skills for each age giving a score of 0 points to a normal status and 1 point to pathological scenarios: from the sum, we got a score from 0 to 6 which correspond to situations of increasing seriousness. The assessment for the neurological examination (motor and sensitive areas) was: 0 points for a normal status; 1, some abnormal features; 2, pathological signs. For the evaluation of vision and hearing, we assigned 0 points to normal characteristics and 1 point to disabilities. The overall neurodevelopmental outcome was established thanks to the scores sum: 0 points for normal status; from 1 to 10 points for impairment of increasing seriousness.
The categorical data were summarized with the absolute and percentage frequency, the continuous ones with the mean and the standard deviation (sd).
Quantitative variables were compared to qualitative variable "sepsis" (no sepsis; with sepsis) using Student's t test for independent samples (two tails). Qualitative variables were compared to qualitative variable "sepsis" (no sepsis, with sepsis) using the Chi-square test. In order to analyse the time trend of stratified outcomes for sepsis, ANOVA was used for repeated measures. The significance was set at 0.05. All descriptive and inferential analysis were carried out using SPSS version 25 technology.
The cross-section resulted to be homogeneous about gender (p = 0.999), gestational age (p = 0.941), birth weight (p = 0.470) and SGA (p = 0.707) (Table 2). There wasn't a significant difference between the 2 groups referring to Apgar score at 5 minutes after birth (p = 0.357).
Table 2: Cross-section clinical features (patients: 42). Legend: frequency; mean (sd). View Table 2
For what concern comorbidities, we observed that the percentages of neonatal respiratory distress syndrome and patent ductus arteriosus were higher in the group of cases (neonatal respiratory distress syndrome: 95%; patent ductus arteriosus: 24%) compared to the group of controls (neonatal respiratory distress syndrome: 76%; patent ductus arteriosus: 10%), while there wasn't any difference for the percentage of BPD between the 2 groups (both 24%) and we had no cases of NEC in our cross-section.
Observing the hospitalization data, we noticed that, according to the statistic analysis, the number of hospitalization days (no sepsis mean ± sd: 66.38 ± 29.979 days, range: 25-153; with sepsis mean ± sd: 72.29 ± 34.858 days, range: 32-191; p-value: 0.559) and auxological data of weight at discharge (no sepsis mean ± sd: 2589.05 ± 399.956 g, range: 1996-3572; with sepsis mean ± sd: 2533.67 ± 699.492 g, range: 1725-4750; p-value: 0.754) and cranic circumference at discharge (no sepsis mean ± sd: 33.23 ± 1.448 cm, range: 30.5-35.5; with sepsis mean ± sd: 33.38 ± 1.856 cm, range: 31.5-39.0; p-value: 0.779) were not influenced by sepsis factor.
Also the number of CVC changes (no sepsis mean ± sd: 1.95 ± 1.465 changes, range: 0-5; with sepsis mean ± sd: 2.38 ± 1.596 changes, range: 1-5; p-value: 0.370), the days of mechanical ventilation (no sepsis mean ± sd: 1.48 ± 2.732 days, range: 0-8; with sepsis mean ± sd: 2.24 ± 3.846 days, range: 0-12; p-value: 0.464) and delivery room intubation did not significantly affect sepsis development.
Instead time 0 and time 48 hours CRP measurement means were effective in determining a significant difference between the 2 groups (no sepsis; with sepsis): p-value was 0.001 at time 0 (no sepsis mean ± sd: 0.56 ± 1.387 mg/dL, range: 0.10-5.09; with sepsis mean ± sd: 3.96 ± 4.028 mg/dL, range: 0.10-15.39) and under 0.0001 at time 48 h (no sepsis mean ± sd: 0.54 ± 0.731 mg/dL, range: 0.10-2.36; with sepsis mean ± sd: 3.57 ± 2.732 mg/dL, range: 0.10-10.05).
Looking at the results of cranic ultrasound scans, the data analysis showed that at time 0 there was not a significant difference between the 2 groups (no sepsis mean ± sd: 2.71 ± 0.561 points, range: 1-3; with sepsis mean ± sd: 2.81 ± 0.679 points, range: 2-5; p-value: 0.623). Anyway, over time the situation tended to be worse in the sepsis group but to improve in the other group (time trend p-value is 0.014). In fact, after 15 days from the first ultrasound scan the comparison between the means in the 2 groups was statistically significant (no sepsis mean ± sd: 2.19 ± 1.289 points, range: 0-4; with sepsis mean ± sd: 3.19 ± 1.289 points, range: 1-5) and p-value is 0.016.
Regarding the follow-up data, the statistical analysis showed that the auxological development of preterm infants who presented sepsis during the hospitalization was not worse than preterm newborns who did not contract any infection in NICU: we didn't found any significant difference comparing the two group means in terms of weight and cranic circumference measurements at 12 and 24 months' corrected age (p-value is greater than 0.05 for all comparisons we made).
In preterm infants with sepsis the neurodevelopmental outcome assessment was worse than the group of controls (Figure 1). In both groups we highlighted the same trend over time about the neurocognitive development (time trend of neurodevelopmental outcome: p > 0.05): even if the group with sepsis settled on worst outcome mean values, compared to the group that did not contract infections, we didn't detect any significant worsening or improvement in the outcome of one group over the other.
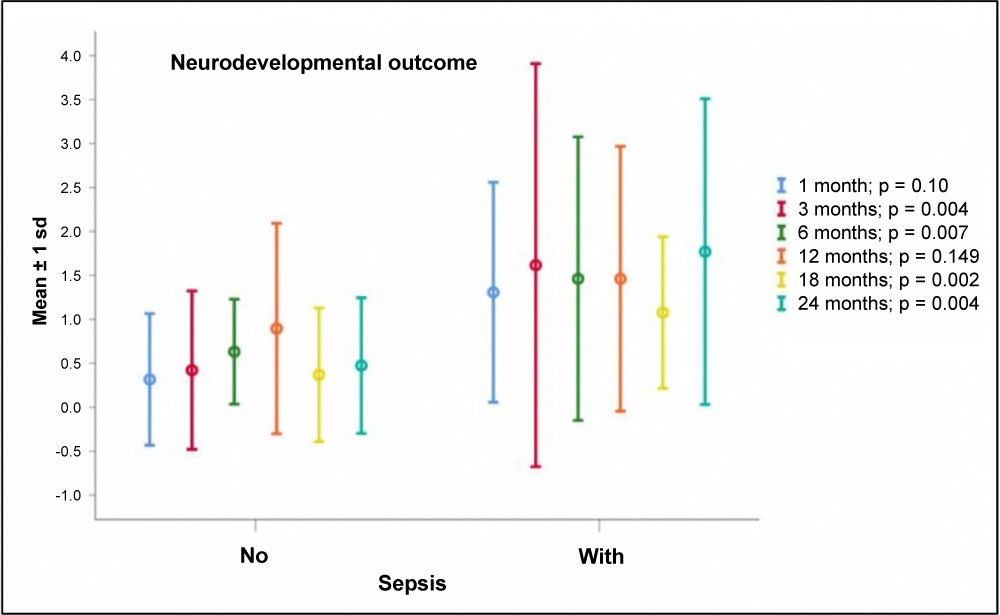 Figure 1: Neurodevelopmental outcome for each follow-up examination (1, 3, 6, 12, 18 and 24 months’ corrected age): comparison between the two groups means (no sepsis; with sepsis).
View Figure 1
Figure 1: Neurodevelopmental outcome for each follow-up examination (1, 3, 6, 12, 18 and 24 months’ corrected age): comparison between the two groups means (no sepsis; with sepsis).
View Figure 1
The comparison of the results obtained at follow-up examinations for each age range showed that the means of the group with sepsis were statistically higher than the control group means: at 1 month's corrected age p = 0.010 (no sepsis mean ± sd: 0.32 ± 0.749 points, range: 0-3; with sepsis mean ± sd: 1.31 ± 1.25 points, range: 0-4); at 3 months' corrected age p = 0.004 (no sepsis mean ± sd: 0.38 ± 2.322 points, range: 0-3; with sepsis mean ± sd: 2.09 ± 2.322 points, range: 0-6); at 6 months' corrected age p = 0.007 (no sepsis mean ± sd: 0.57 ± 0.598 points, range: 0-2; with sepsis mean ± sd 1.62 ± 1.431 points, range: 0-6); at 12 months' corrected age p = 0.149 (no sepsis mean ± sd: 0.86 ± 1.315 points, range: 0-5; with sepsis mean ± sd: 1.53 ± 1.867 points, range: 0-7), but the same trend was still present; at 18 months' corrected age p = 0.002 (no sepsis mean ± sd: 0.38 ± 0.740 points, range: 0-3; with sepsis mean ± sd: 1.30 ± 0.979 points, range: 0-3); at 24 months' corrected age p = 0.004 (no sepsis mean ± sd: 0.43 ± 0.746 points, range: 0-3; with sepsis mean ± sd: 1.65 ± 1.631 points, range: 0-6).
Furthermore, we analyzed the 4 items we used to investigate the neurodevelopmental outcome: we compared the means of the scores obtained for psychomotor development, neurological examination, vision and hearing assessment for each follow-up examination. Data analysis detected that psychomotor development was the area that most influences the statistical significance at 3, 6, 18, 24 months (3 months, p = 0.009; 6 months, p = 0.004; 18 months, p = 0.0001; 24 months, p = 0.001): the aspects of spontaneous and voluntary motility were not the only ones we investigated in this area, but also the behavior, the adaptive functions and above all the cognitive area, which seemed to be the most affected by development impairment in preterm infants [12]. Instead, at 1 month's corrected age the neurological examination was the area in which the difference between the two groups is most significant (p = 0.012) and this is relative to the fact that the neurological examination is the most valid instrument for the assessment of a 1-month-old baby, since psychomotor development becomes more complex with increasing age.
On the other hand, vision and hearing were not decisive factors for the overall neurodevelopmental outcome: among the patients we included in our study there were no cases of severe visual impairment (retinopathy of prematurity with loss of visual acuity) and the hearing loss was diagnosed in only 3 cases independently of the "sepsis" variable.
In conclusion, the preliminary data collected in this research confirmed the role of sepsis in determining a worse neurodevelopment outcome in preterm infants. This agrees with others studies where we can find that proven sepsis (with positive cultures) in preterm infants is associated with a poorer neurological outcome [7] and it takes to impairment of both mental and motor functions which can be assessed using Hammersmith neurological exam [6].
Ultrasound scans were useful to detect the worsening of time trend in preterm newborns with sepsis compared to controls that were improving. In literature authors affirm that the contraction of infections for a preterm infant is an independent risk factor for the development of periventricular leukomalacia (PVL) [13], a pathological status that is more frequently related to premature birth than to term birth [14] and linked to the oxidative stress which occurs in the septic systemic inflammatory status. Our study showed that patients who had diagnosis of sepsis in NICU presented a worsening at the imaging over time, with a prolonged persistence of periventricular echodensity often associated with the appearance of PLV signs [11], compared to the group of controls whose ultrasound scans were improving instead.
For what concern the other variables related to hospitalization, we did not found any statistical difference between the 2 groups about the number of hospitalization days and weight and cranic circumference at discharge: otherwise it seems to be related to the cross-section of our study because, in addition to the cases of EOS (which occur in the first 3 days of life), also the cases of LOS and late clinical sepsis occurred in a relatively early time, not significantly affecting the duration of hospitalization and auxological parameters at discharge. In fact, the groups with LOS and late clinical sepsis presented the infections on average around the 21st day of life, while the mean of the number of hospitalization days was clearly higher (on average each newborn was hospitalized for 73 days). Comparisons related to the number of CVC changes, days of mechanical ventilation and delivery room intubation were also not statistically significant: this seems to confirm the hypothesis that, in our NICU, the management protocols for invasive procedures were adequately applied and therefore the risk of nosocomial infections occurrence, linked to horizontal transmission through therapeutic equipment, was minimized. Instead CRP data confirm what we can find in literature about the use of inflammatory response markers for the infectious state assessment [15,16]: CRP is an early indicator of systemic inflammation useful for monitoring the presence and time trend of sepsis.
A weak point in our research is represented by the poor number of enrolled patients, which affected the statistical analysis of some variables: it is possible that the small number of patients influenced the non-statistically significant result about weight and cranic circumference, which is why studies with a larger cross-section will be necessary in the future.
As for future perspectives, this study could lay the foundations for subsequent studies about the role of sepsis in the development of preterm infants, in particular on the auxological aspects, which need to be further investigated. Another starting point to examine in depth this topic could be to assess whether and how the type of sepsis (proven EOS and LOS and clinical sepsis) correlates with the neurodevelopmental outcome of our patients.
The authors declare no conflicts of interest.
All authors have contributed equally to the manuscript. They provided critical feedback and helped shape the research, analysis and manuscript.
The authors received no financial support for the research, authorship, and/or publication of this article.