The proper use of Insecticides treated nets (ITNs) has been adjudged an efficacious and cost-effective method for curbing malaria. Despite the distribution of ITNs in Nigeria, malaria remains one of the major causes of morbidity and mortality, especially among children below 5-years-old. This systematic review was intended to document the factors mitigating the use of ITNs in Nigeria. Scholarly articles published from the year 2000 through 2018 were reviewed. Six (6) databases (Medline, PubMed, Cinahl Plus, Embase, AJOL and Malaria Journal) were searched for literatures related to the review title, out of which 17 studies were included in this systematic review. This study identified seven (7) themes that mitigate ITNs usage. These are; Heat, low mosquito activity, phobia for chemicals, lack of space and difficulty in hanging nets, preference for other preventive measures, ignorance and cultural beliefs. The heat generated from nets and perceived low activity of mosquitoes contributes to the non-use of ITNs. Also, the fear of chemicals used in the nets, ignorance of the nets, and methods of re-treatment of nets also mitigates the use of ITNs. The difficulties encountered in hanging nets, preference for insecticide sprays, mosquito coils, as well as beliefs (cultural) that malaria should be treated by traditional herbs were found to affect the use of ITNs in Nigeria. Therefore, continuous awareness campaign for malaria prevention with emphasis on the protective effects of ITNs is strongly suggested.
Malaria, Plasmodium species, Insecticide, Treated nets, Nigeria
Malaria is highly endemic in Sub-Saharan Africa, including Nigeria [1,2]. Malaria is a communicable disease, caused by microorganisms of the Plasmodium genus. Four main species of Plasmodium have been reported to cause malaria [2]. The world malaria report released by the World Health Organization (WHO) in 2018 reported an estimated 219 million cases with 435000 deaths globally [1]. With an estimated population of 198million people, Nigeria has the largest population in Africa and the world at large at risk for malaria [1]. This is evidenced by data from the WHO which showed that Nigeria had the highest number of cases and deaths (19%) from Malaria in 2017 [1]. Several studies have shown the burden of Malaria in Nigeria [3-5]. Malaria transmission to humans occurs when an infected female anopheles mosquito bites an uninfected person. The persistent endemic nature of malaria is attributed to climatic conditions which are ideal for breeding of the mosquitoes [6]. The use of insecticide-treated bed nets (ITNs) has proven to be an effective method of reducing malarial attack and mortality associated with the disease [7].
The proper use of ITNs has been adjudged to be an efficacious, cost-effective and efficient method of controlling malaria [8]. Lengeler [8], in a review of studies conducted in different malaria settings reported that, the use of insecticides treated nets led to a 17% percent in mortality, in five randomized control trials. Also, the use of insecticides treated nets in areas of high malaria endemicity, resulted in a 50% reduction of new cases of uncomplicated malaria, compared to settings that did not use nets [8]. Similarly, when compared to settings that used or are using untreated nets, ITN use led to a 39% reduction in incidence of uncomplicated malaria [8]. As part of a larger preventive programme, Insecticides treated nets use aids in reducing malaria episodes in regions, settings and countries where malaria is endemic [9]. The evidence of the cost effectiveness of ITNs explains the robust efforts by the Nigerian Government and Non-Governmental organizations towards provision and supply of ITNs to vulnerable groups, and the entire population at large [10]. This has led to an increase of 69% in coverage of ITNs in Nigeria in 2016 [1].
However, there is an increase in malaria incidence and mortality in Nigeria irrespective of the wide distribution of ITNs [5]. Despite a wide range of studies on ownership of ITNs in Nigeria, there is limited evidence on barriers and difficulties with the use of ITNs. In addition, several studies have examined the effectiveness of ITNs in preventing malaria and some data have reported poor compliance with its use [11-14]. ITNs might have been identified as a cheap and acceptable method of reducing morbidity and mortality caused by malaria, but the factors that determine compliance to use of ITNs must be taken into consideration. Therefore, it is important to review and know why people are not using ITNS. This will go a long way in assisting policy makers, non-governmental organizations, the Government and everyone involved in the fight against malaria in developing behavioural change interventions and campaigns geared towards encouraging and improving the use of ITNs in Nigeria.
Although several or many researches has been carried out in other parts of Sub Saharan Africa on the effects of socio-cultural factors and perception on use of insecticides treated nets, these issues continue to be pertinent and crucial, as Nigeria has embark upon the largest distribution of ITNs in Africa. Also, the relatively low 55% use rate of ITNs in Nigeria, which fell short of the WHO target and recommendation, is a concern. Therefore, it is important to find out the deterrents to regular and constant use of insecticides treated nets in Nigeria. This systematic study was set up to review studies in different parts of Nigeria only from 2000 to 2018, and across different groups to identify the challenges to ITNs usage.
Using six databases (PubMed, CINAHL, Medline, Embase, AJOL and Malaria Journal), a comprehensive review of the literature published since 2000 to 2018 was performed. Publications were searched for keywords including malaria, long-lasting treated bed net, insecticide-treated bed net, ITN prevalence, ITNs usage and challenges in Nigeria. This process identified 265 articles. Out of this number, fifteen (15) studies were from PubMed, fifty (50) from CINAHL, Forty-Six (46) from Medline, Forty-one (41) from EMBASE and One Hundred and thirteen (113) from AJOL. Furthermore, seven (7) studies were identified from reference harvesting, while five (5) studies were identified from the malaria Journal.
Inclusion and exclusion criteria were employed to select articles to be used for this review. The inclusion criteria include: Studies done in Nigeria, peer-reviewed studies, studies carried out and reported in English Language, human studies, and full text studies. Also, this review has an eighteen years (18) time frame starting from 2000, therefore, only studies done from 1st January 2000-10th November 2018 were included. Another inclusion criterion was primary studies with empirical or qualitative data on factors or challenges responsible for the non-use of ITNs in Nigeria. On the other hand, the exclusion criteria were studies not done in Nigeria, studies without full text available, studies done in other languages aside English, animal studies and studies with no empirical or qualitative data on factors responsible for the non-use of ITNS in Nigeria. At the end of the selection process, 17 full texted articles were included and critically appraised for this systematic review (Figure 1).
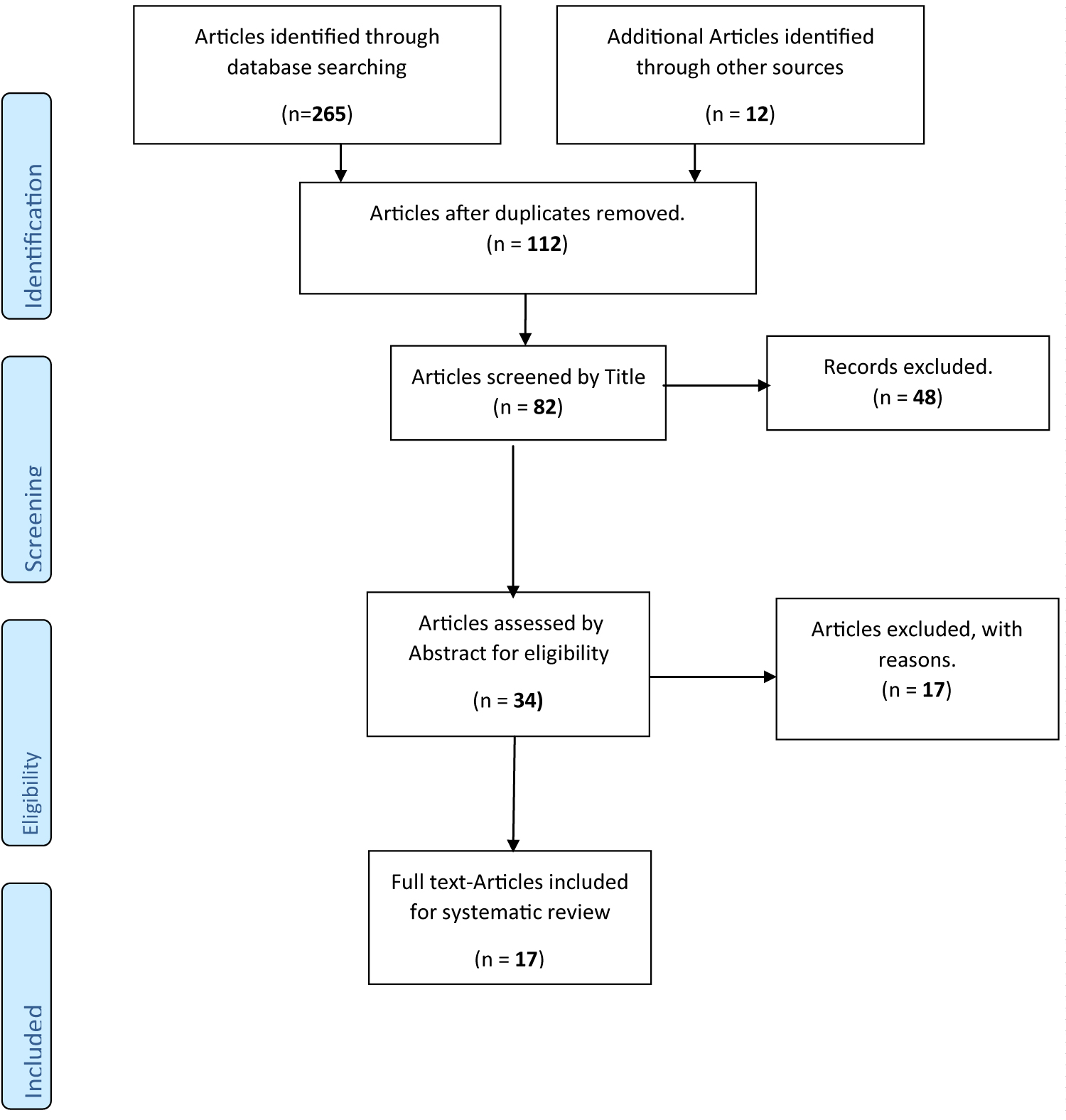 Figure 1: Methodology of searching for and selecting studies to include in systematic review.
View Figure 1
Figure 1: Methodology of searching for and selecting studies to include in systematic review.
View Figure 1
Critical appraisal was done for the seventeen (17) eligible studies using the CASP checklist for qualitative studies. The CASP checklist for qualitative studies contains 10 questions, designed to enhance systematic appraisal of studies [15]. The 17 studies were individually appraised; a score of 8 and above was used as the benchmark for inclusion in the review. At the end of the critical appraisal process, a total of 13 studies with clearly stated aims, correct and right methods, consistent and relevant findings, had a score of 10. A further, 3 articles [3,16,17] had a score of 9. Also, one article [4] had the least score of 8 because, although the research aim(s) was known, it was not clearly stated in the study. This study sought for approval from the Anglia Ruskin University, United Kingdom. The stage one Research Ethics Application Form was completed and submitted to the Faculty of Medical Science Research Ethics Panel (FREP) for approval according to guidelines with reference number FMS FREP17/18221. The data gathered was analysed using the Narrative analysis. This forms the basis for the textual/words analysis. Narrative analysis was adopted for this review because the included articles have different study design; this makes the use of statistical tools difficult.
Out of the seventeen included articles, fifteen were cross sectional studies [2-5,11,12,14,16-23], one study [13] was a randomised controlled trial and one prospective study [24] was also included.
A total of six included studies [4,5,16-18,23] were conducted in the South West, while four were carried out in the South East region of Nigeria [11,13,14,22]. Also, five reviewed studies [2,12,19,21,23] were conducted in the South South Region, while one study each was carried out in Central Nigeria [19] and North West [3] (Table 1).
Table 1: Characteristics of included studies. View Table 1
Furthermore, mean sample size used for this systematic review was 6,439. Israel, et al. [5] had the highest (1020) sample size, while Aribodor, et al. [13] had the lowest (100). In addition, four studies [19,22-24] had children as their study population, accounting for 17% of total sample size, while 25% of total sample size examined the factors mitigating ITNs use among caregivers of under 5 children [4,5,11]. Also, one study [12] used Youth Corp Members as study population (10%), while 4 (22%) studies utilised pregnant women [2,16,17,20]. Similarly, four studies [3,13,14,21] used the general population, while one study [18] used health workers, accounting for 22% and 4% of total sample size.
Key findings from the synthesis of data presented in Table 2 showed some factors mitigating the use of ITNs in Nigeria. These factors formed challenges and themes for this study as follows:
Table 2: Findings from individual Articles. View Table 2
• Heat or hot night temperature
• Low mosquito activity
• Lack of space/difficulty in hanging nets
• Phobia for chemicals
• Preference for other preventive measures
• Cultural beliefs
• Lack of knowledge
Heat or the quality or feeling of being hot due to high temperature, especially at night, was reported by 11 studies to affect ITN use in Nigeria. In addition, the perceived non-availability of mosquitoes at certain times, or low mosquito activity was found to be another factor mitigating ITN use. This was reported by 4 studies. Also, the lack of space in households and difficulty in hanging the nets was analysed to have constituted barriers to ITN use in Nigeria, as reported by 9 studies. Although both triangular and square nets exist, most of the distributed nets in Nigeria are square. The sense of danger/harm caused by chemicals used for treatment of ITNs was analysed to be a major factor for non-use of ITNs. This was reported by10 studies. Furthermore, analysis of data from studies recognised the preference for insecticide sprays and other preventive methods as another factor mitigating ITN use, as reported by 7 studies. The beliefs, thoughts and experiences acquired during growth and interaction within the social environment (cultural beliefs) also constituted challenges to ITN use. This was reported by 2 studies. Finally, the lack of knowledge and information on malaria, as well as the protective effects of ITNs, as well as ways of displaying, hanging and usage mitigated ITN use, as reported by 5 studies.
This systematic review using only literatures published since 2000 provides a comprehensive review on the challenges of using insecticide treated nets for malaria prevention in Nigeria. Challenges identified include, heat or hot night temperature, low mosquito activity, lack of space for hanging, phobia for chemicals, preference for other preventive methods, lack of knowledge on preventive effects of ITNs and cultural beliefs. This is in consonance with findings from other studies [17,25,26].
The identification of heat as one of the major challenges of using ITNs by this study is similar to reports from other researchers [11,19,27]. Nigeria has a tropical weather condition and temperature of about 22 °C-37 °C, according to the Nigerian Meteorological Agency (NIMET) [28]. The unavailability of power/electricity, especially at night in most part of the country, coupled with the hot temperature has reportedly resulted in non-use of ITNs as reported by 12 out of the 17 included studies [2,3,5,11,13,14,16,17,20,22,23,29]. Studies from different countries reported similar findings [27,30]. In contrast, a study of communities in Mestizo, Peru found out that ITN users' enjoyed the fact that it made/kept them warmth at night this may be due to their cold climate condition in the country [31].
This systematic review observed that low mosquito activity was associated with non-use of ITNs in Nigeria. Mosquitoes were perceived to be seasonal in Nigeria, with low activity during the dry season, which has led to the non-use of ITNs during that period [19]. However, findings from the present study showed no seasonal difference in mosquito activity. This is evidenced by the fact that, 2 out of the 4 reviewed studies that reported low mosquito activity as a reason for non-use of ITNs were carried out during the wet or rainy season [5,23], while one was carried out during the dry season [19]. In relation to endemicity, low mosquito activity was reported in reviewed studies where malaria endemicity was reported to be moderate or Mesoendemic [19,21]. In contrast, low mosquito activity was less of a problem in studies where endemicity was high [13,20,24]. This can be attributed to the fact that such areas and environments with high endemicity are habitable for mosquitoes, and have mosquito breeding areas [13,20]. The finding of low mosquito activity as a factor mitigating ITNs use in Nigeria, in the present study showed consistency with similar studies. A study in Vanuatu observed that the low activity of mosquitoes was a major challenge of using ITNS in the area [32]. Also, Iwueze, et al. [30] reported that 1.0% of participants did not use ITN because of low mosquito problem. Similarly, a review of literature and a community-based study in Calabar (South-Southern Nigeria) reported low mosquito activity as a challenge of using ITNs [21,25]. In contrast, Gobir, et al. [3] found no association between low mosquito activity and ITNs use.
Findings from this study showed that lack of space in households and difficulties in hanging as a challenge of ITNs usage. This finding is supported by studies in Nigeria, Cameroon and Ghana [4,29,30,33].
This study discovered phobia for chemicals as a major factor responsible for non-use of ITNs. Some ITN owners' feared perceived danger and harm associated with coming in contact with chemicals or insecticide (for example, permethrin) used in ITNs, and therefore, chose not to use the nets. The fear of intoxication and harm from chemicals used in ITNs was also reported in several studies in Nigeria [5,13,18,27,29]. Furthermore, a study in Western Kenya reported that participants said they are not using ITNs because they were concerned that, the insecticide (chemical) may be toxic [27]. Therefore, it can be adduced that this finding contributes greatly to the non-use of ITNs in Nigeria.
The present study found that some ITNs owners do not use it because they prefer other measures of prevention available in the area. These include use of insecticide sprays, mosquito coils, and chemical sprays. This is consistent with findings from some studies [12,17,29,34,35]. Therefore, it can be said that this challenge of ITN use is down to interest and choice. Although, other preferred methods might also be effective, ITNs can be promoted as being a more protective and cheaper method to encourage use. This study also discovered that lack of and poor knowledge of malaria, protective effects of ITNs, ways of displaying/hanging and re-treatment as a challenge to non-use of ITNs in Nigeria. Several studies correlate with the finding in Nigeria [20,36]. A study in Uganda by Uwaha, et al. [37] discovered poor knowledge among participants as being responsible for non-use. Similarly, findings from a study in Ghana found that participants had little to no knowledge on malaria and how to use ITN, this in turn affected use [38]. Pettifor, et al. [39] stated that higher knowledge on malaria and ITN was significant to use. This finding was not in agreement with a study by Natalie, et al. [40] which stated that knowledge of malaria and ITNs had no effects on use.
This study discovered that cultural beliefs posed challenges to ITN use in Nigeria. These include beliefs that malaria occurs as a result of witchcraft and therefore, should be prevented and treated by native doctors, as well as traditional herbs [2]. Other beliefs are that malaria cannot kill a child whose parents have no enemy, hence, no need for using ITNs [41]. The belief that neglecting the gods and committing "taboos" result in illnesses also contributed to the non-use of ITNs, as people who believed they were living right saw no need for ITNs [24]. Also, the inherent belief in parts of the country, that the African man is immune to diseases played a huge role in the non-use of ITNs [41]. Some studies support this finding. For example, a study in a rural community in Nigeria reported culture as a challenge of using ITNs, participants stated that their fore-fathers used herbs as remedy for malaria, hence their non-use of ITNs [2]. Jombo, et al. [42] found out that cultural belief (10.6%) was responsible for non-use of ITNs in Makurdi, Benue State. Akogun and John, [43] reported that reliance and holding on to the belief that witches, and wizards were responsible for malaria mitigated the non-use of ITNs for prevention in North Eastern Nigeria. A community-based study among caregivers of < 5 children in South-Eastern, Nigeria however reported no relationship between culture and ITN non-use [11].
Although, malaria remains endemic in Nigeria, the coverage and challenges of the use of insecticides treated nets (ITNs) for prevention and control remains low. This review has reported the factors, reasons and challenges that affect ITNs usage in Nigeria. Difficulty in displaying or hanging nets, fear of chemicals and inherent cultural beliefs in parts of the country are some of the identified mitigators of ITNs use in Nigeria. In addition, most of the identified challenges of using ITNs were found to be related to behaviour and choice. Therefore, malaria prevention education and continuous distribution of ITNs by creating more channels to enhance the use of ITNs are recommended.