Coronavirus disease 2019 (COVID-19) is caused by a novel coronavirus now called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The most serious complication of COVID-19 is a type of pneumonia that’s been called 2019 novel coronavirus-infected pneumonia (NCIP). COVID-19 pneumonia presents as an atypical pneumonia, with diffuse bilateral lung involvement. Severe cases present with acute lung injury, and acute respiratory distress syndrome (ARDS).
Potential risk factors for severe COVID-19 pneumonia include age above 65 years, diabetes, hypertension, chronic obstructive pulmonary disease, immunosuppression, pregnancy, overcrowding. In addition, some laboratory parameters such as elevated C-reactive protein and D-dimers and low lymphocyte count have also been associated with increase disease severity with a poor prognosis.
This is a case of fulminant COVID-19 pneumonia in a 53-yr-old know diabetic and hypertensive, who had markedly elevated C-reactive protein and D-dimers and low lymphocyte count during COVID-19 infection.
COVID-19, Viral pneumonia, Disease severity, Risk factors, Cytokine storm
SARS-CoV-2: Severe Acute Respiratory Syndrome Coronavirus 2; COVID-19: Corona Virus Disease 2019; WHO: World Health Organization; NCIP: Novel Corona Virus-Infected Pneumonia; SARS: Severe Acute Respiratory Syndrome; HIV: Human Immunodeficiency Virus; HBV: Hepatitis B Virus; HCV: Hepatitis C Virus; CRP: C-reactive Protein; CT: computed tomography; ARDS: Acute Respiratory Distress Syndrome; ACE2: Angiotensin-Converting Enzyme 2
Coronavirus disease 2019 (COVID-19) is caused by a novel coronavirus now called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which was first identified in Wuhan City, Hubei Province, China. The Chinese authorities reported an increasing number of cases of pneumonia in Wuhan City, which they later identified the causative organism to be a corona virus. It was initially reported to the WHO on December 31, 2019. On March 11, 2020, the WHO declared COVID-19 a global pandemic [1], its first such designation since declaring H1N1 influenza a pandemic in 2009. The disease has so far spread to 212 Countries, and by May 11 2020, 4,006,257 cases have been reported globally with 278,892 deaths. The African continent so far is the least hit by the COVID-19 pandemic with a total of 44,533 cases and 1415 deaths [2].
The estimated mean incubation period of SARS-CoV-2 is 1-14 days. Fever is often the major and initial symptom of COVID-19. Other symptoms include dry cough, sore throat, shortness of breath, muscle ache, diarrhea, nausea, dizziness, headache, rhinorrhea, chest pain, and vomiting. The disease is usually mild in about 80% of cases while 20% progress to severe disease [3,4]. In severe cases, patients quickly progressed to develop acute respiratory syndrome, septic shock, metabolic acidosis, and coagulopathy.
Being primarily a respiratory infection, COVID-19 is transmitted mainly through inhalation of infected droplets which are generated when an infected person coughs, sneezes, talks, sings. Measures to limit the spread of the infection have been put in place by many Countries since the beginning of the pandemic. These measures include social lockdown, social distancing, restrictions on travels, use of face mask and frequent hand washing or use of alcohol-based hand sanitizers. In places where these measures have been implemented, they have been shown to be beneficial in slowing down the infection rate [5,6].
Risk factors for severe COVID-19 disease include older adults age above 65 years, people of all ages with underlying diseases such as diabetes, hypertension, cardiovascular disease, chronic obstructive pulmonary disease, asthma, sickle cell disease, malignancy, chronic kidney disease, HIV/AIDS, as well as other causes of immunosuppression [7-9].
The most serious complication of COVID-19 is a type of pneumonia that’s been called 2019 novel coronavirus-infected pneumonia (NCIP) [10]. COVID-19 pneumonia presents as an atypical pneumonia, with diffuse bilateral lung involvement. Severe cases present with acute lung injury, and acute respiratory distress syndrome (ARDS).
We present a case of fulminant COVID-19 pneumonia in a 53-yr-old known hypertensive/diabetic patient.
Patient was a 53-year-old man who was a known hypertensive and diabetic on antihypertensive and oral hypoglycemic agents. Patient was amlodipine 10 mg and metformin 500 mg 12 hourly for his hypertension and diabetes control respectively. His pre-COVID blood pressure and sugar control were unknown.
He presented with a two week history of fever, dry cough, shortness of breath, diarrhea, headache and sore throat. On account of the above symptoms, he presented to a private hospital where he was managed with antibiotics and antimalarial with no improvement. Nasopharyngeal and oropharyngeal swabs were taken for PCR test for COVID-19 which turned out positive. Patient was referred to the isolation center at the University of Abuja Teaching Hospital for further management.
On arrival at the isolation center, patient was in respiratory distress with a respiratory rate of 40 breathe/min, oxygen saturation was 83% on room air, temperature was 36.4 °C, pulse rate was 106 beats/minute, blood pressure was 140/90 mmHg. The random blood sugar at presentation was 7.2 mmol/L. An assessment of severe COVID-19 pneumonia was made.
The following investigations were done: chest radiograph, Full Blood Count, blood culture, electrolytes, urea and creatinine, fasting blood sugar and gene expert to exclude pulmonary tuberculosis, Nigeria being endemic for TB disease. He was commenced on intravenous Ceftriaxone 1 gram 12 hourly, Hydroxychloroquine 400 mg 12 hourly on day 1, then 200 mg 12 hourly subsequently; Zinc sulphate 220 mg daily, Azithromycin 500 mg daily, Lopinavir/ritonavir 400 mg 12 hourly, Vitamin C 200 mg 8 hourly. Intranasal oxygen was commenced at the rate of 5 liters/min. He was also commenced on subcutaneous low molecular weight heparin at 40 mg daily.
The full blood count showed a white blood count of 11.6 × 109/L with a differential neutrophil count of 66% and lymphocyte count of 14%. He had thrombocytosis with a platelet count of 581 × 109/L. The liver function and renal function tests were essentially normal. Blood culture showed no bacterial growth. Gene expert was negative for Mycobacterium tuberculosis; HIV, HBV and HCV screen were all negative. Fasting blood sugar done the following morning was 10.4 mmol/L and he was commenced on soluble insulin 6 IU pre-meal. C-reactive protein was 212 mg/L (normal range 0-5 mg/L). D-dimer was > 5 μg/ml (normal value < 0.5 μg/ml). Chest radiograph showed bilateral ground glass opacities in both lung fields (Figure 1).
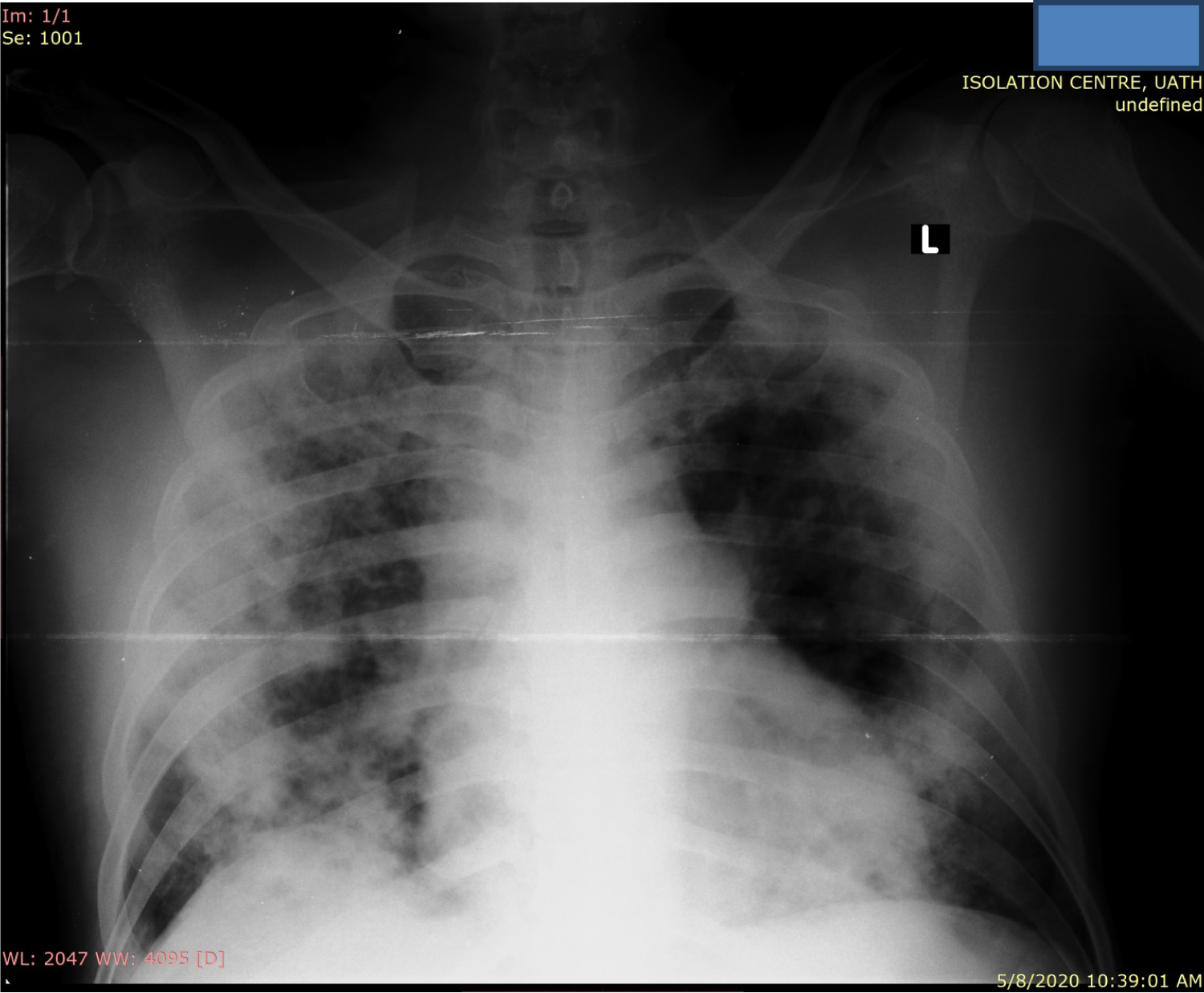 Figure 1: Chest radiograph showed bilateral ground glass opacities in both lung fields.
View Figure 1
Figure 1: Chest radiograph showed bilateral ground glass opacities in both lung fields.
View Figure 1
Patient continued to deteriorate despite above measures with persistently low oxygen saturation below 92%. Oxygen delivery was switched from use of intranasal catheter to non-rebreather mask. He continued to deteriorate and died 48 hours after he was brought into the isolation ward.
Doctors and Scientists all over the world are learning about COVID-19, the disease caused by the novel coronavirus, SARS-COV2. Amid the coronavirus pandemic, pneumonia has become of greater concern because it's a common and potentially deadly complication of COVID-19. Severe cases present with acute lung injury, and ARDS. When ARDS happens there is uncontrolled inflammation characterized by the release of a series of cytokines (cytokine storm) including TNFα, IL-1β, IL-2, IL-6, IFNα, IFNβ, IFNγ, and MCP-1 [11]. This causes fluid accumulation in the alveoli and progressive fibrosis which severely compromises the gas exchange. In addition, both type-I and type-II pneumocytes become dysfunctional, leading to decreased levels of surfactant and reduction in the ability of the lungs to expand [12]. Abnormalities in chest radiography include bilateral patchy shadows or ground glass opacity in the lungs [13]. The worse the chest X-Ray findings, the more severe the disease.
This patient presented with severe COVID-19 pneumonia. The underlying diabetes and hypertension were the most likely risk factors for the disease severity. He had markedly elevated C-reactive protein (CRP) levels. A high level of CRP in the blood is a marker of inflammation. The markedly high levels in this patient (more than 42 times the upper limit of normal) is a pointer to the extensive lung injury and disease severity that eventually lead to the death of this patient. CRP levels have been shown to correlate with disease severity in patients with COVID-19 pneumonia [14,15]. CRP has also been shown to correlate with computed tomographic (CT) findings and predicts severe COVID-19 pneumonia [16]. Though CT was not done in this patient, his chest X-Ray showed extensive lung damage.
Many patients with severe COVID-19 present with coagulation abnormalities that mimic other systemic coagulopathies associated with severe infections, such as disseminated intravascular coagulation (DIC) or thrombotic microangiopathy [17]. The most typical finding in patients with COVID-19 and coagulopathy is an increased D-dimer concentration. D-dimer is a fibrin degradation product, a small protein fragment present in the blood after a blood clot is degraded by fibrinolysis. Various studies in patients with COVID-19 have shown a very strong association between increased D-dimer levels and severe disease/poor prognosis [18]. A four-fold increase in the protein is a strong indicator of mortality in those suffering from COVID-19 [19]. Our patient had markedly elevated D-dimer levels greater than 10 times the upper limit of normal that was an indicator of disease severity and subsequent mortality.
Contrary to what is seen in other viral infections, COVID-19 pneumonia is associated with lymphopenia. Lymphocytes play a decisive role in maintaining immune homeostasis and inflammatory response throughout the body. Some studies have shown that a low lymphocyte count is an indicator of the severity of disease among hospitalized patients with COVID-19, and that Patients who died from COVID-19 are reported to have had significantly lower lymphocyte counts than survivors [20,21]. Many mechanisms that lead to lymphocyte depletion in severe COVID-19 have been postulated. One of such mechanisms is the direct destruction of lymphocytes by the coronavirus that binds on the ACE2 receptor on the lymphocytes. Our patient had a low lymphocyte count of 14% that was associated with the disease severity.
Though COVID-19 present as a mild disease in about 80% of cases, an atypical viral pneumonia known as COVID-19 pneumonia may develop. Patients with COVID-19 pneumonia may progress to a more severe and systemic disease, characterized by acute lung injury with acute respiratory distress syndrome (ARDS), shock, coagulopathy, and multiple organ dysfunctions, associated with substantial mortality. We present the case of fulminant COVID-19 pneumonia in a 53-year-old man with underlying diabetes and hypertension who had blood markers consistent with severe inflammation and thrombosis.
The authors declare no competing interest.
VK conceptualized, and developed the manuscript. ZH, TY, AF, BA, and AA reviewed the manuscript.
The authors wish to acknowledge the management of the University of Abuja Teaching Hospital for the enormous support given to the COVID-19 management team. The authors also wish to acknowledge the support of the Federal Capital Territory Administration, The Nigerian National Petroleum Corporation and the Mainstream Energy Solution Limited for their generous donations to the University of Abuja Teaching Hospital Isolation Center.