Philippines is among the top southeast Asian country that is endemic to Dengue Fever based on DOH reported cases - from a reported 152,224 in 2017 to an increase in 216,190 in 2018. Most studies in the country are derived from the pediatric and/or young adult population hence, there is a dearth of data describing our elderly patient with dengue. This is a retrospective observational study of elderly individuals diagnosed with Dengue Fever admitted at St. Luke's Medical Center, E. Rodriguez, Quezon City from January 1, 2013 to December 31, 2018. A total of 142 elderly were recorded; 65% are females. Hypertension (53.8%) and Diabetes mellitus were the most common comorbid conditions. Aside from fever (98%), the elderly patients presented most frequently with arthralgia and/or myalgia at 38.46% followed by cough (35.66%), generalized body malaise (32.17%), decreased appetite (31.47%), headache (25.8%), loose bowel movement (15.38%), petechial rash (13.97%), chills (13.99%), and colds (11.19%). Serologic evidence of plasma leakage was seen in 20 patients (14%) while 77 patients showed leukopenia (53.8%) with the lowest recorded WBC count of 1.2/μL; 69% had thrombocytopenia though only 12% were transfused with either platelet concentrate or PRBC. The most common electrolyte imbalance was mild hyponatremia (36%) followed by mild hypokalemia (28.8%). Liver and renal failures were also seen in some patients.
Dengue, Elderly, Older adults, Laboratory, Clinical profile
ALT: Alanine Aminotransferase; AST: Aspartate Aminotransferase; CBC: Complete Blood Count; CKD: Chronic Kidney Disease; DENV: Dengue Virus; DFS: Dengue Fever Syndrome; DF: Dengue Fever; DOH: Department of Health; NS1: [Dengue Virus] Nonstructural Protein 1; PRBC: Packed Red Blood Cell Product; SE: Standard Error; SD: Standard Deviation; SLMC QC: St. Luke's Medical Center - Quezon City; WBC: Whole Blood Cell
Dengue is found in tropical and subtropical regions, predominantly in urban and semi-urban areas. The disease is caused by a virus belonging to family Flaviviradae that is spread by Aedes (Stegomyia) mosquitoes [1]. Since the first confirmed epidemic of DHF recorded in the Philippines in the 1950s, dengue fever has become a major health concern in the country.
Worldwide, incidence of Dengue Fever has increased 30-fold over the last 5 decades, is endemic in more than 100 countries including the Philippines, and causes an estimated 50 million infections annually [2]. The Department of Health (DOH) reported almost more than 110,000 cases of dengue yearly since 2013; 152,224 in the year 2017 and 216,190 in 2018 [3].
Dengue infection is a systemic and dynamic disease with an extensive clinical spectrum that includes severe and non-severe forms of clinical manifestations. The patients are classified according to the levels of severity as having dengue without Warning Signs, Dengue with Warning Signs, and Severe Dengue based on clinical manifestations with or without laboratory parameters. After the incubation period, the illness begins abruptly and will be followed by 3 phases: Febrile, critical and recovery phase [4].
Amidst hundreds of published and unpublished researches on Dengue in the Philippines, there are still knowledge gaps to be identified. The vast majority were descriptive short-term hospital- or community-based studies [5]. And while majority of these gathered cases belong to the younger group, the clinical and laboratory profile that were frequently studied belong to this said population. A study done at St. Luke's Medical Center in 2010 described the clinical and serological manifestations of DFS but it is of the pediatric group [6]. There is a scarcity of published data that describe the symptomatology and laboratory profile of elderly patients with dengue fever especially those who are in the Philippines. Dengue has a wide clinical spectrum ranging from asymptomatic to severe clinical manifestations. When this (elderly) vulnerable population contract DENV, their symptoms are more apparent and sometimes atypical. Elderly patients in India from June 2010 to May 2012 were studied and discovered other uncommon presentations of dengue fever [7].
It would still be unclear if there are differences in the clinical spectrum Dengue Fever occurring in the elderly population in the Philippines. Their comorbidities and physiologic changes could perhaps contribute to this [8-12] and so, management could be differently approached in the elderly vulnerable compared to the latter.
By 2050, the world's population aged 60 years and older is expected to total 2 billion, up from 900 million in 2015. And since the pace of population ageing around the world is increasing dramatically, studying dengue fever in this population is a very important issue [5]. Even basic dengue information such as this is vital to be communicated to policymakers, health workers, academics, and other stakeholders [13].
This study will center on the severity level, clinical and laboratory manifestations of elderly patients with dengue. A study of this magnitude on elderly cases with a longer time span, from 2013 to 2018, has not been studied in the Philippines.
The data collated will give emphasis on what is to be expected in the clinical and diagnostic background and/or sequelae of elderly individuals infected by dengue fever. Information collected hopes to contribute more to future research in the country, future government health programs for Senior Citizens and public awareness since it can characterize the burden and clinical spectrum of Dengue virus infection in the geriatric group.
To describe the clinical and laboratory characteristics of elderly patients diagnosed with dengue fever at St. Luke's Medical Center, Quezon City Philippines from January 1, 2013 to December 31, 2018.
This is a retrospective observational study of elderly individuals diagnosed with Dengue Fever admitted at St. Luke's Medical Center, E. Rodriguez, Quezon City from January 1, 2013 to December 31, 2018.
Charts of elderly patients reviewed for the gathering of information on the severity level, clinical and laboratory characteristics.
The subject must possess ALL of the following characteristics:
1) 60-years-old and above admitted in St. Luke's Medical Center, Quezon City from January 1, 2013 to December 31, 2018 with a final diagnosis of Dengue fever
2) CBC (leucopenia with or without thrombocytopenia) and/or with a positive IgM antibody for Dengue &/or Dengue NS1
Fever, Headache, Body malaise, Myalgia, Arthralgia, Retro-orbital pain, Anorexia, Nausea, Vomiting, Diarrhea, Flushed skin, Rash (petechial, Hermann's sign) and Laboratory test, at least CBC (leucopenia with or without thrombocytopenia) and/or dengue NS1 antigen test or dengue IgM antibody test [4].
Complete Blood Count with Platelet count
Serologic evidence of plasma leakage - A rise in the hematocrit equal to or greater than 10-15% above average for age, sex, and population and/or a drop in the hematocrit following volume replacement treatment equal to or greater than 10-15% of baseline [1].
Leukopenia - reduction in the circulating WBC count to ≤ 4000/μL [14].
Thrombocytopenia - platelet count 100,000 cells/mm3 or less [4].
Serum Sodium and Potassium [15]
Mild Hyponatremia- between 126-135 meq/L; Moderate Hyponatremia- between 120-125 meq/L; Severe Hyponatremia- less than 120 meq/L
Mild Hypokalemia between 3.00 to 3.50 meq/L; Moderate Hypokalemia: between 2.50 to 2.9 meq/L; Severe Hypokalemia- less than 2.50 meq/l
Kidney Injury - increase in serum creatinine up to > 1.4 mg/dL in a patient with original normal kidney function or doubling of the baseline serum creatinine value within 3 days if he or she has an underlying chronic renal disease [7].
Liver failure - AST or ALT ≥ 1000 [4].
Lives in or travels to dengue-endemic area, with fever lasting for 2-7 days, plus any of the following:
• Abdominal pain or tenderness
• Persistent vomiting
• Clinical signs of fluid accumulation
• Mucosal bleeding
• Lethargy, restlessness
• Liver enlargement
• Laboratory: Increase in Hct and/or decreasing platelet count within 24-36 hours
Clinical fluid accumulation was defined as the new presence of pleural effusion and/or ascites which was disclosed by chest radiography and/or ultrasonography [16].
Lives in or travels to a dengue-endemic area with fever of 2-7 days and any of the above clinical manifestations for dengue with or without warning signs, plus any of the following:
• Severe plasma leakage, leading to:
- Shock (manifested by tachycardia, poor tissue perfusion with weak pulse and narrowed pulse pressure (20 mmHg or less) or hypotension with the presence of cold, clammy skin and/or restlessness.)
- Fluid accumulation with respiratory distress
• Severe bleeding
• Severe organ impairment
- Liver: AST or ALT > 1000
- CNS: e.g., seizures, impaired consciousness
- Heart: e.g., myocarditis
- Kidneys e.g., renal failure
This is a retrospective observational study of elderly individuals diagnosed with Dengue Fever admitted at St. Luke's Medical Center, a 540-bed capacity tertiary hospital along E. Rodriguez, Quezon City, from January 1, 2013 to December 31, 2018. All adults aged 60 and above admitted at St Luke's Medical Center from January 1, 2013 to December 31, 2018 diagnosed with DENV Infection is the target population. Census was provided by SLMC Medical Records Section. The data gathered from the medical records included age, sex, clinical manifestations, complications, radiologic (Chest X-ray), hematologic (Complete Blood Count with Platelet count), and available chemistry studies such as serum sodium, potassium, ALT, Creatinine were documented from each patient. Mean duration of hospitalization was included as well.
The chief complaint of the patient, other symptoms, and complications related to Dengue Fever infection as mentioned in the Revised Dengue Clinical Case Management Guidelines 2011. DOH 15th Ed were identified. Among the symptoms, mean duration of fever was determined. Percent frequency of the common symptoms was also determined. This can either be patient-reported &/or Clinician-reported outcomes found in the medical records. Categorical data such as age group, sex, and discharge disposition is reported in percentage.
Hematologic (Complete Blood Count with Platelet count), and available chemistry studies such as serum sodium, potassium, ALT, Creatinine was summarized in standard deviation.
Percentage and total number (sum) of individuals under the different levels of severity as having dengue without warning signs, Dengue with warning signs, and severe dengue based on clinical manifestations with or without laboratory parameters; most common laboratory results, mean duration of admission day/s, and sum number case mortality due to dengue fever were determined.
Sample size was calculated based on the estimation of the population. A proportion of 0.5 was used since this will yield the largest sample size possible, there being no previous studies on this population. Assuming that this proportion of elderly with a clinical outcome is 50%, with a maximum allowable error of 6% and a reliability of 80%, the sample size required is 116.
From 2013 to 2018, St Luke's Medical Center had a total of 142 elderly patients diagnosed with Dengue Fever. The young old individuals aging 60 to 69-years-old at the time of admission belong to the majority of these elderly cases at 57.34%. Middle old or those belonging to the 70-79 years of age came in next to 23.78% then finally 18.18% of the elderly patients were 80-years-old and above. See Figure 1 for the Subgroups of Older Adults. Majority of the admitted cases were females at 65.03%. There are different ways to classify the population of older adults, but the authors decided to classify them between 60 to 69 years as young old, the middle old (70 to 79 years) and the very old (80 years and older) as mentioned in one article [17]. In a surveillance data done in Puerto Rico, the elderly had 2.4 times the risk of hospitalization as did youths, and 1.7 times the risk of adults [18]. Patients can be admitted either during their febrile phase while some during the critical and recovery phases. The mean days of admission are at 4.6 days (SD ± 2.5).
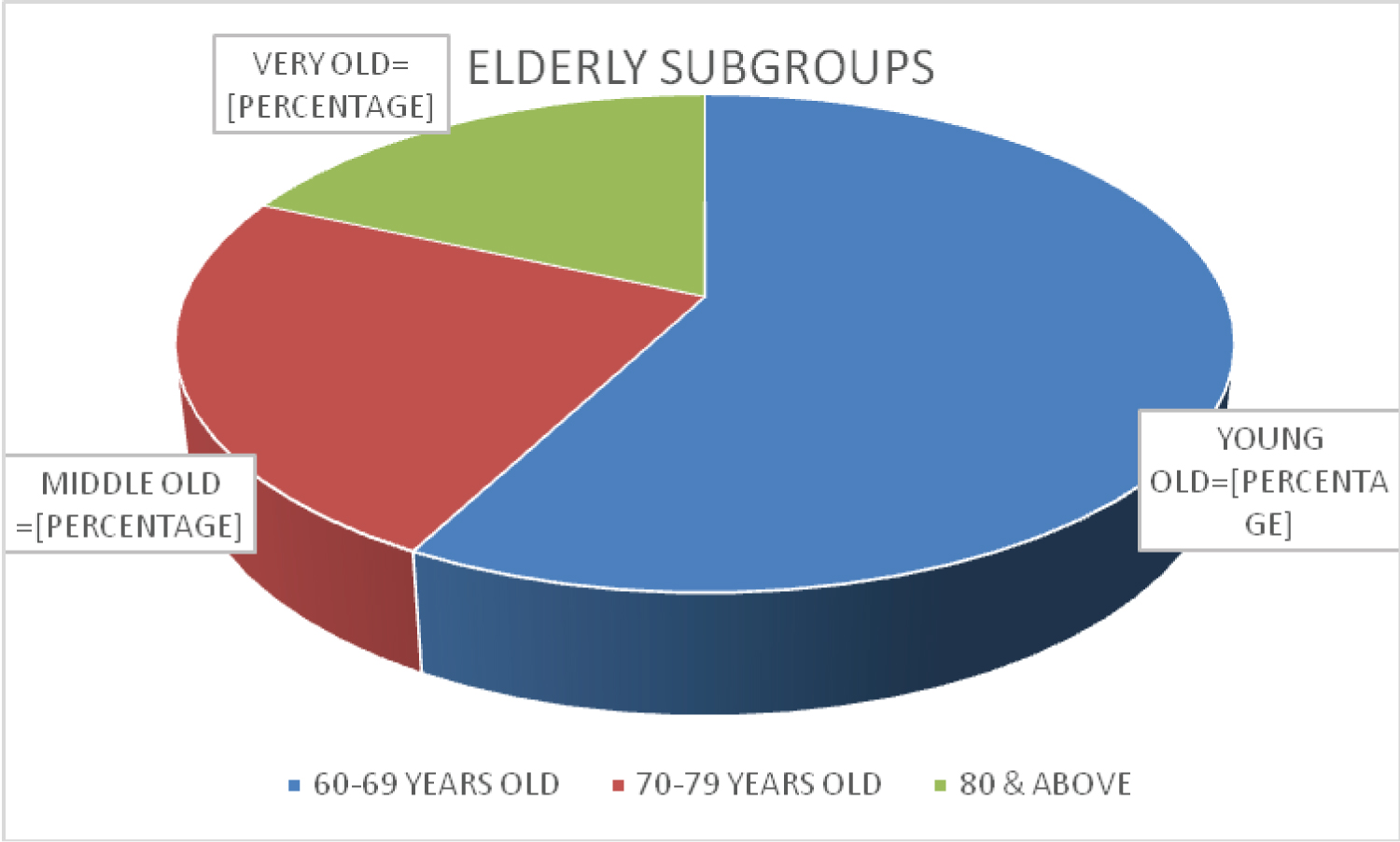 Figure 1: Elderly subgroups.
View Figure 1
Figure 1: Elderly subgroups.
View Figure 1
It should be noted that, there were certain individuals with only one, or two or more co-morbid conditions. Among these, Hypertension (53.8%) is the most common chronic condition or co-morbidity found. Other conditions recorded were Diabetes mellitus (20.28%), heart failure with or without coronary artery disease (14.69%), malignancy or cancer (4.9%), chronic kidney disease (3.5%), bronchial asthma or Chronic obstructive pulmonary disease (2.09%) and liver cirrhosis (1.4%). We believe that comorbidities are relevant to causing severe clinical dengue, and the management in our elderly patients, though challenging, should be individualized taking into consideration their accompanying comorbid conditions.
There is a variation of clinical manifestations of dengue which range from asymptomatic to undifferentiated fever to severe dengue or unusual manifestations including multi-organ failure [19]. Fever is the most common symptom presentation. The febrile period can last between 2 and 7 days [20]. In our observation, mean duration days an elderly patient is febrile was at 4.9 days (SD ± 2.6). Aside from fever, the elderly patients presented most frequently with arthralgia and/or myalgia at 38.46% followed by cough (35.66%), generalized body malaise (32.17%), decreased appetite (31.47%), headache (25.8%), loose bowel movement (15.38%), petechial rash (13.97%), chills (13.99%), and colds (11.19%). Fever, myalgia headache, and rash were also the major symptoms seen in a Taiwanese study, though, are at a lower frequency compared to the non-elderly [16]. In studying two hundred and ninety five aged 60 and above, it was found that elderly patients were less likely to present with symptoms of headaches (35.3% vs. 49.1%, P = < 0.001), rash (36.6% vs. 47.6%, P = < 0.001), nausea (48.8% vs. 56.1%, P = 0.014), and mucosal bleeding (12.5% vs. 24.2%, P = < 0.001) compared to the younger group [21]. In those aged 17-years-old or younger, the most common clinical manifestations were flushed skin, anorexia and abdominal pain [6].
Warning signs usually precede the manifestations of shock and appear towards the end of the febrile phase, usually between days 3-7 of illness [22]. Warning signs such as abdominal pain or tenderness are noted at 18.88%, while gastrointestinal bleeding (either melena, hematochezia or hematemesis) occurred at 1.4%. Hemorrhagic manifestations described as mucosal bleeding such as epistaxis, or bleeding gums was observed at 6.29%. As cited in a review [23], elderly patients with dengue tend to have fewer hemorrhagic manifestations than their younger counterparts [21,24,25].
Nausea (7.7%), bloatedness (6.29%), dizziness (4.19%), sore throat (3.5%) and shortness of breath (3.5%) were seen in a minority of the admitted. As observed, many of the patients fail to complain these symptoms when they transition from febrile to afebrile phase.
An elderly could sometimes present atypically - interestingly, three elderly individuals had no fever at all (2.1%) and two patients who were classified as severe dengue presented with delirium and decreasing sensorium. The atypical presentation can be likely due to age-related decline in immune function. Cell-mediated and humoral immunity resulting in impaired cytokine response could alter disease presentation [26] See Figure 2 for the Clinical Presentation.
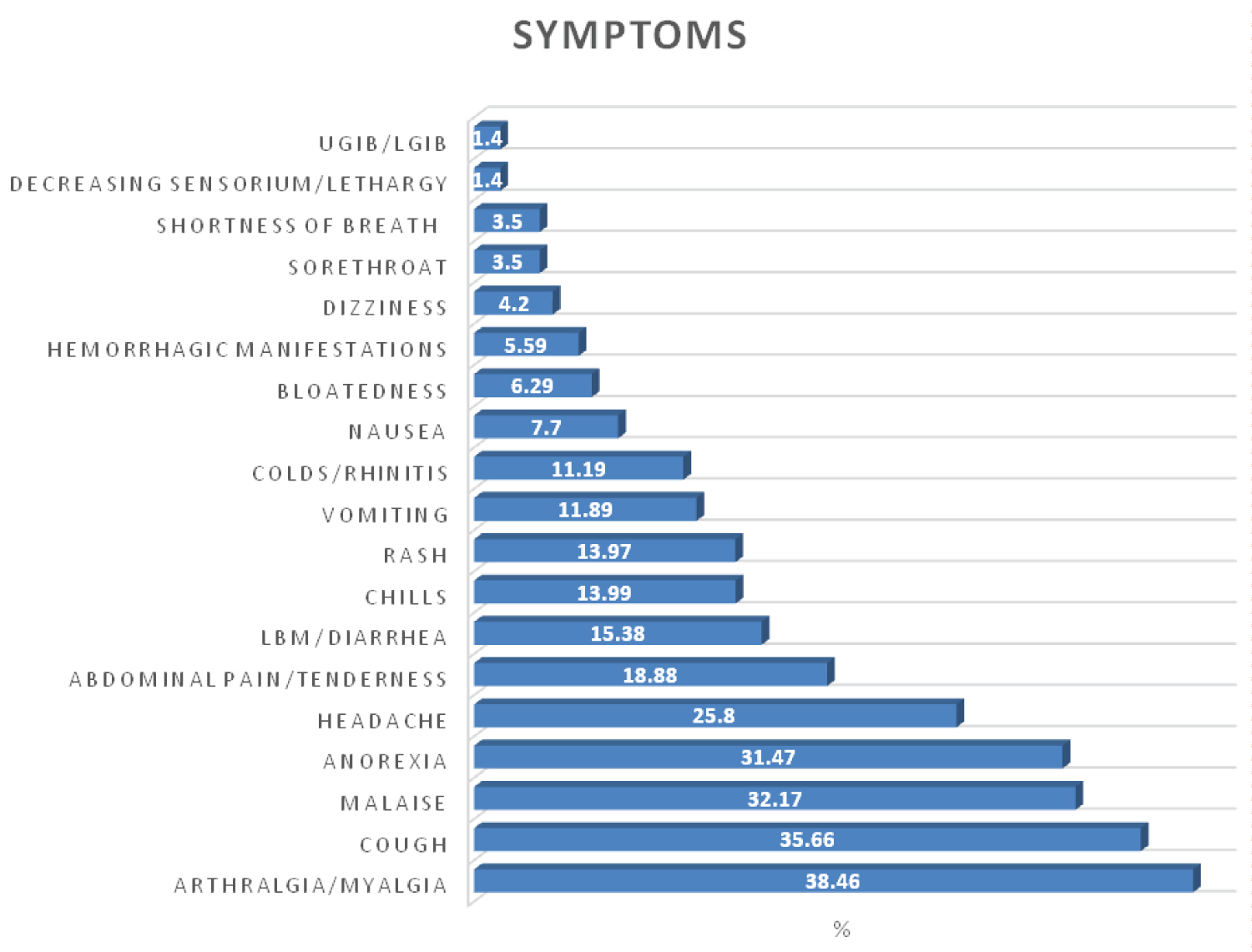 Figure 2: Clinical presentation/symptoms.
Figure 2: Clinical presentation/symptoms.
UGIB: Upper Gastrointestinal bleeding; LGIB: Lower gastrointestinal bleeding.
View Figure 2
The patients that tested positive for NS1 Antigen were only at 25% (N = 17) while a bulk of these cases at almost 86% tested positive for IgM. These assays were extracted at different days wherein patient was febrile which could account for why there are positive versus negative results. Anti-dengue IgM specific antibodies can be detected 3-6 days after fever onset. On average, IgM is detected in 50% of cases by days 3-5 after the onset of illness, this increasing to 95-98% for days 6-10 [22]. On the other hand, rapid NS1 antigen and NS1 ELISA showed the highest positivity on days 1-3 of fever with a sensitivity & specificity of 55.5% and 92% [27]. Also, the sensitivity of NS1 detection in the febrile phase as mentioned in an article by CP Simmons, et al. [28] is lower in secondary infections by 60 to 80%, reflecting an anamnestic serologic response. This can be due to a past dengue virus or related flavivirus infection [29].
In another study, thrombocytopenia (platelet count < 150 K/μL) (77.4%) (mean of 68.5 K/μL with SD of 49.6) was the major hematological abnormality followed by leukopenia (total white blood cell count < 4 K/μL) (mean 5.2 K/μL with SD 2.3) (52.8%) [7]. Out of the 142 individuals, serologic evidence of plasma leakage was seen in 20 patients (14%) while 77 patients showed leukopenia (53.8%) with the lowest recorded WBC count of 1.2/μL. Surprisingly, 31% of the elderly did not show thrombocytopenia during the course of their confinement.
Sixty five patients (45%) had warning signs and 71% of these patients (N = 46) were reported to have co-morbid conditions. It was also observed that majority (92%) of these elderly with warning signs were on the febrile period during their stay in the hospital. All had normal vital signs except for one patient who had hypotension but was reversed with adequate fluid challenge.
In adults, a platelet count of 5 × 109 L-1 and packed cell volume > 50 are significantly associated with bleeding manifestations [30]. Seventeen patients were transfused with either platelet concentrate or PRBC. Five of these patients who were transfused presented with clinical signs of active bleeding such as epistaxis, bleeding gums, and GI bleeding; two with generalized body weakness, one patient with concomitant malignancy, and the other with decreasing sensorium. All of the seventeen had thrombocytopenia with 4,000 cells per mm3 as the lowest recorded platelet count. Most clinical guidelines recommend that platelet transfusions be given if with serious hemorrhagic manifestations or very low platelet counts falling below 10-20 × 109 L-1 without hemorrhage or 50 × 109 L-1 with bleeding or hemorrhage. Consequently, those who received transfusion had a higher frequency of pulmonary edema and increased length of hospitalization [31]. There were no reports of pulmonary congestion after transfusion in our observation.
Aging is associated with extensive changes in body composition that alter water and electrolyte distribution and predispose older adults to the development of fluid and electrolyte abnormalities [32]. Among other serologic laboratory results (Table 1), 36% had mild hyponatremia and 28.8% had mild hypokalemia. Average serum Sodium observed is at 135 mmol/L (SD ± 4.3) and serum potassium at 3.7 mmol/L (SD ± 0.52). One study in India involving the elderly observed an incidence of hyponatremia (serum sodium < 135 mEq/L) was higher (50.9%) (mean 129.8 with SD of 14.66) with 13.2% of the patients developing significant hyponatremia (< 125 mEq/L). More than half of the hyponatremic elderly patients are symptomatic [7]. Another study says that hyponatremia followed by hypokalemia were frequently seen in patients with DF especially among Dengue hemorrhagic fever and Dengue shock syndrome [16]. Hyponatremia is the most common electrolyte abnormality in dengue; the lowest sodium levels are seen in patients with DF [33,34]. The prevalence of hyponatremia is about 10 times more common among dengue patients compared to non-dengue febrile infections [35]. The hyponatremia may be due to: Excess water from increased metabolism, the influx of sodium into cells due to a dysfunction of the sodium-potassium pump or a combination of these factors [18]. The most common cause of hyponatremia in older individuals is the syndrome of inappropriate ADH secretion (SIADH). [32,34]. Other factors such as low solute intake, vomiting, or diarrhea may contribute. A combination of mechanisms may be responsible for the hypokalemia seen in dengue infections. Hypokalemia in dengue is more likely to be due to a transient functional impairment rather than due to structural renal damage or could also result from increased renal excretion due to activation of the renin angiotensin and aldosterone system (RAAS) secondary to volume depletion [20]. And since majority of the older adults have comorbidities warranting intake of maintenance medications such as diuretics, including the basic serum electrolytes to blood exams is recommended.
Table 1: Laboratory profile of confined patients with dengue fever. View Table 1
Aside from serum sodium and potassium, serum creatinine should also be included as well in an elderly with DF. Renal dysfunction was observed in 15.1% of elderly patients in one study [7] which is similar to the findings we observed. Amid the elderly who had acute kidney injury during their hospital stay (15.3%), one underwent hemodialysis because of acute renal failure. Elderly people have the highest risk of Acute Kidney Injury compared to other age groups because of more comorbid conditions, higher prevalence of CKD, polypharmacy, and structural, functional, and hemodynamic age-related changes affecting the ability of the kidney to withstand insults as well as cellular changes to renal tubular cells rendering them more vulnerable [36].
Liver cells are one of the targets of dengue viruses [37]. One patient developed liver failure exhibiting symptoms of anorexia, abdominal pain and weakness similar in patients with liver disease. The liver dysfunction was mild to moderate, presenting primarily as elevations of hepatic transaminases; patients with pleural effusion and/or ascites had significantly higher AST elevation [38,39]. The average levels of AST ranged from 93.3 U/L [38] to 174 U/L [40], while ALT from 86 U/L [38] to 88.5U/L [40] in various studies - these data though were taken from a combined pediatric and adult population. The number of the patients in this paper who had a record of their AST levels however is very limited, thus we only reported the ALT levels which showed an average of 104.06 U/L.
Signs of fluid accumulation such as pleural effusion were observed in 19 elderly patients (20%) with only one patient requiring thoracentesis. Five had concomitant ascites which were noted to be minimal. Perhaps the number of individuals with pleural effusion and/or ascites could have been contributed by the majority of the patients having co-morbid conditions and hypoalbuminemia. Mean albumin was at 2.8 g.dL. As cited by CP Simmons, et al., hypoalbuminemia and proteinuria are observed during dengue infection; proteins up to and including the size of albumin are preferentially lost; this is consistent with a small but crucial change in the filtration characteristics of the glycocalyx [41].
The potential for dual infection in the aged population especially those who are already frail and had waning immunity should be considered. There are also cases observed (28%) wherein patients had to be started with antibiotics. The most common co-infection was pneumonia (60%) followed by Urinary Tract Infection (20%). Pneumonia and UTI was also observed in elderly patients with DF in another study [21]. Concurrent bacteremia was more common in elderly DHF patients (17.4%) compared with nonelderly DHF patients (3.4%) in Taiwan [42]. Hospital acquired infection occurred at greater frequency in the elderly (13/295, 4.9%) versus the adults (66/6694, 1.2%) [21]. Elderly individuals with a dengue virus infection are more likely to develop a critical condition, and were at risk for acquisition of bacterial coinfections [43].
A retrospective case-control study showed that the mortality rate in DF patients aged > 65-years-old, admitted from September to December 2015 was at 4.3%. The independent predictors to predict the mortality were severe coma, bedridden, severe hepatitis (AST > 1000 U/L), and renal failure (serum creatinine > 2 mg/dL) [44]. Fortunately, there were no reports of mortality due to DFS during the six years.
Aside from fever as prevalent symptom (98%), the elderly patients presented most frequently with arthralgia and/or myalgia at 38.46% followed by cough (35.66%), generalized body malaise (32.17%), decreased appetite (31.47%), headache (25.8%), loose bowel movement (15.38%), petechial rash (13.97%), chills (13.99%), and colds (11.19%). Serologic evidence of plasma leakage was seen in 20 patients (14%) while 77 patients showed leukopenia (53.8%) with the lowest recorded WBC count of 1.2/μL; 69% had thrombocytopenia though only 12% were transfused with either platelet concentrate or PRBC. The most common electrolyte imbalance was mild hyponatremia (36%) followed by mild hypokalemia (28.8%). Liver and renal failures were also seen in some patients.
As a retrospective study, there are limitations to be considered. The number of cases gathered could not represent the general population of geriatric patients in the country since it was conducted in a single medical center.
Taking into consideration the effects of immunological senescence, comorbid conditions, reduced physiologic reserves, and the elderly's risk for polypharmacy, the clinical management of dengue infection should be handled differently and with greater caution [23]. Especially, knowing that they are more vulnerable and are more prone to dual infections, complications, falls, and poorer outcomes due to infection, the authors suggest careful assessment of their cardiac and functional status prior to management. The efficacy and safety of future vaccinations for this population should also be well-studied.
The authors cannot give definite conclusions since data could be heterogeneous for exposures and outcomes. We recommend analytical studies comparing the data between younger adults and the elderly with dengue fever in the country. We also encourage prospective studies with a larger population and perhaps compare the data from this study to other Philippine-based centers where dengue fever is highly endemic.
The study abided the Principles of the Declaration of Helsinki (2013) and is conducted along the Guidelines of the International Conference on Harmonization-Good Clinical Practice (ICH-GCP). The clinical protocol and all relevant documents were already reviewed and approved by the SLMC Institutional Ethics Review Committee. Patient confidentiality was respected by ensuring anonymity of patient records. Each patient is CODED and does not contain any identifying information in order to ensure confidentiality. All study data were recorded and the investigators are responsible for the integrity of the data i.e accuracy, completeness, legibility, originality timeliness and consistency.
A Census from 2013 to 2018 with patients diagnosed with Dengue fever was provided by SLMC Medical Records section with the permission from the department's manager and approval from the Office of Medical Education & Training. Because this is a retrospective observational study, informed consent from the patients was waived and the welfare of the patients was not affected.
Personal data such as patient's name and addresses were strictly kept confidential within the hospital's records section and collection of pertinent information related only to the study such as laboratory and clinical finding/s were ones recorded and analyzed as data.