Objective: The prevalence of Human Immunodeficiency Virus (HIV) and Hepatitis B Virus (HBV) infections and their co-infection are rarely reported among undergraduate Nigerians. This study sought to provide data in the said direction and discuss policy imperatives.
Methods: A population of 4,876 undergraduate students of the Alex Ekwueme Federal University, Ndufu-Alike (AEFUNAI), Nigeria (52.7% females; mean age: 20 ± 2 yrs, females; 20 ± 3 yrs, males) was studied. Standard procedures were used for collection and analysis of peripheral blood specimen.
Results: HIV prevalence was found to be 0.0-0.34% (females) and 0.0-0.61% (males). There was a 34-folds increase in prevalence over the 4-year period irrespective of sex. HBV prevalence was found to be 0.8-1.8% (females) and 2.6-3.8% (males), with a clear decline in prevalence among males and a marginal accent in prevalence among females, over the years. HIV/HBV co-infection prevalence was very low, as no female and only 0.09% of all males studied had both HIV and HBV at the same time.
Conclusion: Though HIV and HBV prevalence rates were low, the rate of increase (for HIV) and sex-related differences in trend (for HBV) is worrisome. Further studies to unravel the drivers of these phenomena and the low co-infection rates are warranted. The intensification of appropriate health education in secondary and tertiary institutions is advocated.
Human immunodeficiency Virus, Hepatitis B virus, Co-infection, Undergraduates, Nigeria
One major cause of mortality from liver disease world-wide is hepatitis B virus (HBV). It affects 5-8% of adults in sub-Saharan Africa [1]. In Nigeria, double digit prevalence rates have been reported [2,3]. HIV/AIDS is a serious public health issue globally, but particularly in sub-Saharan Africa, where prevalence rates are as high as 25.8%. In Nigeria, the prevalence of HIV is put at 1.8-4.1%, depending on cultural, educational, and socioeconomic differences [4,5]. The National Agency for the Control of AIDS (NACA) in Nigeria however reported a prevalence of 1.5 percent among adults in 2018 [6].
Human Immunodeficiency Virus (HIV)/Acquired Immune Deficiency Syndrome (AIDS) patients have a 6-folds higher likelihood of having HBV [7]. Indeed, approximately, 10% of all HIV infected patients worldwide have chronic HBV co-infection [8]. Both HBV and HIV are contacted through body fluids thereby placing sexually active youths at higher risk of the diseases. Yet screening for HBV and HIV among undergraduate students is not routine in Nigeria. Considering that accurate estimates of the prevalence of HIV and HBV are critical for evidence-based policy formulation and action, the Alex Ekwueme Federal University, Ndufu-Alike (AEFUNAI), Nigeria, began the screening of new students for the said diseases in 2015. Here, we present the initial data for the 2015/2016 to the 2018/2019 academic years.
All apparently-healthy newly admitted students for the 2015/2016 to the 2018/2019 academic years, who gave an informed written consent were recruited for the study. Exclusion criteria for this study included: Awareness of being positive for HIV or HBV and presence of physical deformity making anthropometry difficult.
Self-reported age was recorded per subject. Their heights and weights were measured using standard protocol; and their body mass index (BMI) calculated. Peripheral venous blood samples (3 ml) were obtained from each subject and HIV antibodies were screened for using a national serial algorithm process, involving different rapid diagnostic test kits [Determine-HIV 1&2 (Alere Inc., Massachusetts), Uni-Gold™ Recombigen® HIV-1/2 (Trinity Biotech, Wicklow) and Stat-Pak-HIV-1&2 (Chembio Diagnostic Systems, Inc. Medford)]. On the same samples Hepatitis B surface antigen (HBsAg) rapid test, which is based on the principle of sandwich immunoassay for determination of the antigen in serum or plasma or whole blood, was used to screen for the presence of hepatitis B virus (HBV). Skytec rapid diagnostic test kits (ScyTec Labs., Utah) were used, while the ABON kits (ABON Biopharm Co. Ltd., Hangzhou) were used to reconfirm all sero-positive samples. All the rapid diagnostic kits used in this study have sensitivity and specificity values of > 95% according to their manufacturers.
The protocol and design for this study was approved by the Human Research Ethics Committee of Alex Ekwueme Federal Teaching Hospital Health Research Ethics Committee (AE-FETHA/Rec/Vol 1/2020/679; Rec Protocol Number 14/02/2020-24/02/2020).
Differences between means were separated by One-Way ANOVA (continuous variables) and the Chi square test (or Fischer's exact test; categorical variables). A significance threshold of P < 0.05 was adopted for all analyses.
A total of 4,876 subjects (52.7% females) were effectively studied. The mean ages (years) for the subjects were 20 ± 2 (females) and 20 ± 3 (males). There were no significant differences (P > 0.05) in the BMI of the sexes at any time point. The studied population was lean by BMI standards (Table 1). This is not surprising as the prevalence of overweight/obesity is low among Nigerian undergraduates [9].
Table 1: Age and BMI of the subjects. View Table 1
The prevalence of HIV (irrespective of sex) increased 34-folds (61-folds among males) over the course of the 4 years. The rise in the trend line for males is clearly steeper than for the females (Figure 1) and the prevalence values for the males, from 2016 to 2018 were significantly higher (P < 0.05) than those for females.
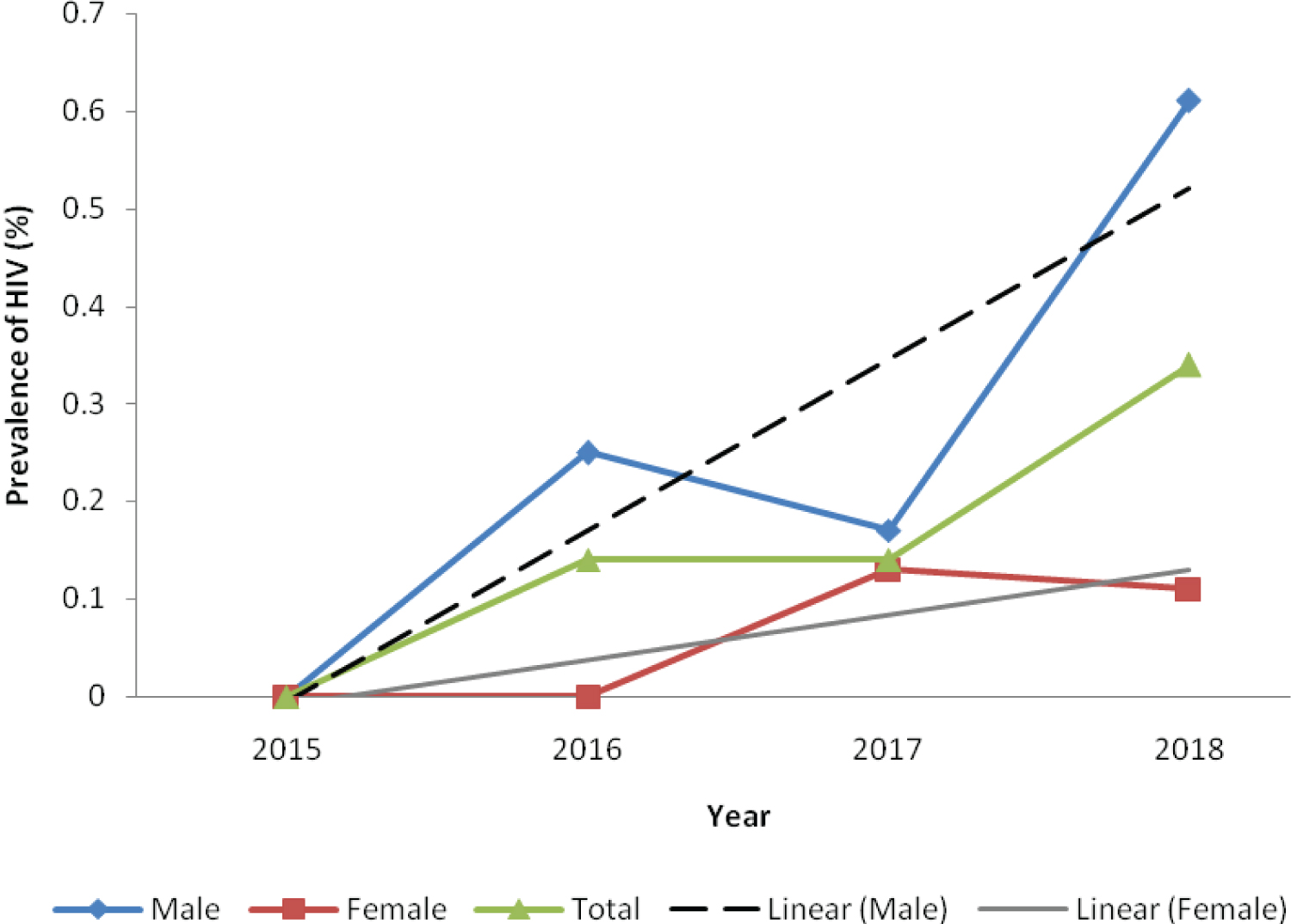 Figure 1: Prevalence of HIV among first year undergraduate students of AEFUNAI.
Figure 1: Prevalence of HIV among first year undergraduate students of AEFUNAI.
Data is for 513 students (F, 250; M, 263) in 2015, 1447 students (F, 658; M, 789) in 2016, 1394 students (F, 791; M, 603) in 2017 and 1522 students (F, 870; M, 652) in 2018.
View Figure 1
Considering the 1.5% prevalence reported for 15 to 49-years-old Nigerians in 2018 [6], the values reported in the present study are small [0.0-0.61% (males) and 0.0-0.34% (females)]. The increase in the prevalence suggests that more young persons (possibly in their teenage years) are being infected with the virus such that the disease burden among fresh undergraduates is rising. The drivers of such variations in the prevalence and trend require investigation.
HBV prevalence was markedly higher than HIV prevalence irrespective of sex and year. The value for males (2.6-3.8%) is close to the value reported in the region (5-8%) [1], while the females had lover prevalence values (0.8-1.8%). Akin to HIV prevalence, the prevalence of HBV was significantly higher (P < 0.05) in males than in females. Given the similarities in the modes of transmission of both HIV and HBV, it appears understandable that the males are affected more by HBV. However, whereas the trend line for the males shows a clear decline, that for the females show a marginally ascending pattern (Figure 2). Therefore, the drivers for HBV infection may be different from those driving HIV infection.
 Figure 2: Prevalence of HBV among first year undergraduate students of AEFUNAI.
Figure 2: Prevalence of HBV among first year undergraduate students of AEFUNAI.
Data is for 513 students (F, 250; M, 263) in 2015, 1447 students (F, 658; M, 789) in 2016, 1394 students (F, 791; M, 603) in 2017 and 1522 students (F, 870; M, 652) in 2018.
View Figure 2
Interestingly, HIV/HBV co-infection prevalence was very low as no female, and only 0.30% of males in 2018 and 0.09% of all males studied had both HIV and HBV compared to 10% reported elsewhere [8]. This suggests that the HBV found in this population is not an opportunistic infection, subsequent to HIV. It appears that both diseases are distinct but jointly point to conditions that predispose about 25 in every 1000 young persons studied to viral infectious diseases. This is more worrisome given that the population studied (with more than twelve years of formal education) is more educated than the average population in Ebonyi State and should therefore be more aware of the measures to be taken in preventing these diseases.
Given the variations in the diagnostic tools used by different authors and other variables such as socio-economic factors, education, etc., that colour disease spread, the prevalence data presented here and the comparisons to other data reported by previous authors require a cautious interpretation.
Finally, the nature of disease prevention messaging offered in secondary and tertiary schools may need examination for impact-enhancement. Efforts aimed at intensifying health education counselling, including curriculum adjustments where necessary are advocated. The current policy of the Alex Ekwueme Federal University, Ndufu-Alike on compulsory screening for these viral diseases is commendable and should be sustained. Efforts at replicating similar policies among other tertiary institutions in the country should be encouraged.
Approval was obtained from the Health Research Ethical Committees of Federal Teaching Hospital Abakaliki Health Research Ethics Committee: FETHA/Rec/Volc1/2017/479; Rec Protocol Number 14/02/2017-24/02/2017.
Informed written consent were obtained from all patients that participated in the study.
Not applicable.
Data-sets used and analyzed for the study are available and may be released by the corresponding author on reasonable request.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The role of the sponsors/authors include the study design, collection, analysis and interpretation of data; as well as in the writing and decision to submit the article for submission.
HEA conceptualized and designed the study and coordinated all the research activities including the writing of the manuscript; SOAO participated in drafting the initial manuscript; CN and MN coordinated the laboratory testing, as well as the data collection; CECCE analysed and interpreted the data and participated in the drafting of the initial manuscript and its revision. All authors reviewed the study's findings, read and approved the manuscript before submission.
We are most grateful to staff of the Medical Laboratory department of the Alex Ekwueme Federal University Medical Centre who assisted in the screening tests over a period of 4 years. We also acknowledge with thanks all the respondents who willingly gave their consent and participated in the study.