The efficacy of Ivermectin (IVM) against SARS-CoV-2 has been demonstrated in vitro, while several clinical studies suggest that it is efficacious and safe in reducing morbidity and mortality. Hydroxychloroquine (HCQ, Quinoric®), IVM and Azithromycin (AZM, Zithromax®) (HIA therapy) is being used in several low- and middle-income countries (LMIC) where more expensive medications such as Remdesivir are out of reach. In this study, we set out to compare the efficacy of IVM monotherapy with HIA combination therapy.
Methods: This was a single-blind, randomized control trial, of 2 parallel groups of COVID-19 Positive Nigerians. Thirty (30) patients received Ivermectin (Mectizan®) 200 mcg/kg daily for five days, while 31 patients received HIA triple therapy. Viral cycle threshold (Ct) at pre-treatment baseline, and days 2, 5, 14 and 21 were measured for E- and N-genes (Envelope and Nucleocapsid genes respectively). SpO2 (percentage saturation of oxygen in the blood) was assessed on a daily basis, while inflammatory markers such as Erythrocyte Sedimentation Rate (ESR), C-Reactive Protein, and D-dimer and Neutrophil/Lymphocyte Ratios (NLR), were assessed at baseline and day 7 post treatment. Clinical status was self-assessed daily on a Likert scale.
Results: 2-way Repeated measures Analysis of Variance (RMANOVA) did not show any difference between the two groups. However, there was a significant time effect (improvement over time) for SpO2, Ct N-gene, Ct E-gene and clinical status in both groups, and significant reductions in inflammatory markers by day 7 (P < 0.0001).
Conclusions: AZT + HCQ may be redundant adjuncts in COVID-19 therapy. Improvements noted are likely due in large part to Ivermectin virucidal and anti-inflammatory actions.
The World Health Organisation (WHO) declared a COVID-19 pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus on March 11, 2020 [1]. Since then, there have been global and massive disruptions in economic, transportation, social interaction, political, and health care delivery that is unprecedented and unparalleled in recent human history. As of September 2021, more than 223 million people have been infected with more than 4.6 million deaths [2]. Robust measures including vaccinations [2] have become available to stem community transmission of the SARS-CoV-2 virus and especially the more contagious Delta variant of SARS-CoV-2 [3]. Recovery from the pandemic has, however been slower than anticipated, owing to a combination of vaccine hesitancy in high income countries, and also by resource limitation and vaccine insufficiency for the eligible population in the low- and middle-income countries (LMIC). Other measures, in addition to public health modalities, including chemoprophylaxis, and continued treatment of COVID-19 with a variety of repurposed drugs or their combinations have therefore been employed. We have previously reported on the beneficial effects of Ivermectin in mild to moderate COVID-19 patients in a randomized controlled double blind, dose response study [4]. We have also hypothesized on the putative utility of an additive combination Ivermectin with novel antiviral drug, molnupiravir [5]. After the publication of Gautret, et al. [6] and Raoult, et al. [7] among others, doctors in many LMICs, including in Nigeria, prescribed a cocktail of Ivermectin (IVM, Mectizan®) combined with Hydroxychloroquine (HCQ, Quinoric®) and Azithromycin (AZT, Zithromax®) to treat early or mild COVID-19 patients. Other studies have however suggested that HCQ is not useful as post exposure prophylaxis and may be associated with ECG anomalies in a proportion of patients [8,9].
Ivermectin has an in vitro IC50 for SARS-CoV-2 in Vero-SLAM cells of 2.4 uM [10] and exerts inhibitory SARS-CoV-2 effects by multifarious mechanisms, including blocking viral entry, inhibiting viral nuclear transport by Importin alpha and beta, and inhibiting RNA dependent, RNA polymerase (RdRp) [11].
Chloroquine (CQ) and HCQ have an IC50 for inhibition of SARS-CoV-2 in vitro of 42- 56.8 uM, and 9.2-11.2 uM respectively [12] but CQ does not inhibit SARS-CoV-2 infection in human lung cells [13]. The mechanisms of SARS-CoV-2 replication inhibition by CQ/HCQ include blockade of viral cell invasion, via lipid rafts, interference with viral endocytosis, binding to angiotensin-converting enzyme 2 (ACE2) and viral spike protein, blockade of endosomal acidification, and sequestration of Zinc ions which block SARS-CoV-2 RdRp [14].
Azithromycin is a macrolide antibiotic, which has been reported to inhibit SARS-CoV-2 in vitro in Vero cells and in Caco-2 cells (human colorectal adenocarcinoma cells) [15]. AZT has an IC50 of 2.1 uM, which is not dissimilar from the molar value for IVM [16]. It is a weak base, and thus inhibits the acidic dependent uncoating and endocytosis of the SARS-CoV-2 virus. AZT binds the spike protein S, thereby reducing binding to ACE2 receptor, limiting viral entry. The drug amplifies host anti-viral defense, through increase in Interferon (IFN) and inhibition of IL-6 production [17].
There are reports of the additive or synergistic combination of AZT + HCQ in clinical trials in COVID-19 [6], even as other clinical trials, such as the RECOVERY Collaborative Group showed no efficacy of HCQ in hospitalized COVID-19 patients [18]. These disparate findings make it imperative to assess the additive or synergistic actions, if any, of the combinations of repurposed drugs, used in COVID-19 treatment.
The purpose of the present study was to examine and compare the clinical, virological and anti-inflammatory effects of Ivermectin alone, compared to Ivermectin + HCQ + AZT triple therapy (HIA triple therapy or IVM+), in RT PCR, SARS-CoV-2 positive patients with COVID 19 in a randomized controlled trial.
Null hypothesis (H0): A combination of Ivermectin plus Hydroxychloroquine plus Azithromycin is not more efficacious in the treatment of patients with virology proven COVID-19 disease compared to Ivermectin alone.
Alternative Hypothesis (Ha): A combination of Ivermectin and Hydroxychloroquine plus Azithromycin is more efficacious in the treatment of patients with virology proven COVID-19 disease.
Approval to carry out the research was obtained from the University of Abuja Health Research Ethics Committee. The study adhered to the tenets of the Declaration of Helsinki. (https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/).
Cases were enrolled between the 2nd of May until the 11th of June 2021.
Consecutive COVID-19 positive patients of all ages and gender notified to the Federal Capital Territory COVID-19 Control Center based in Gwagwalada were eligible for inclusion in the trial, provided informed consent was not withheld.
Were Lack of a positive COVID-19, refusal to give informed consent, pregnancy, history of heart disease and known or reported allergy to any of the trial medications.
This was a single-blind, randomized, parallel group study, of 2 groups of COVID-19 Positive Nigerian patients with 30/31 subjects in each treatment arm. These are designated arms 'A' and 'B'
A. 30 patients received Ivermectin 200 mcg/kg daily for five days
B. 31 patients received HIA triple therapy
a. Hydroxychloroquine 200 mg per day for three days
b. Ivermectin 200 mcg/kg daily for five days,
c. Azithromycin 500 mg per day for three days.
All three are together referred to as HIA triple therapy.
Average weight in the trial was 69.3 kg, ranging from 51-86 kg. Based on the weight, the patients required an average of 5 tablets of 3 mg of Ivermectin (15 mg) daily. (Range 12-21 mg daily).
Patients across the board were also availed Standard of Care for COVID-19 patients in Nigeria including Zinc Sulfate, and vitamin C. The use of Ventilators and Oxygen was applied as needed. Three patients required oxygen therapy, one in the IVM group and two in the IVM+. They had baseline SpO2% (percentage saturation of oxygen in the blood) of 94, 78 and 89 respectively.
Patients were to have ECG done in case they developed palpitations. None of the patients required this.
A GeneXpert machine was used to measure quantitative Reverse Transcriptase Polymerase Chain Reaction (qRT-PCR). Two different RNA particles are measured: N-gene (Nucleocapsid) and E-gene (Envelope). A semiquantitative measure of cycle threshold (Ct) values was assessed. (Time to detection is quantified by the machine. The longer it takes, the lower the viral load) All two marker genes must be negative before a patient is deemed negative for SARS-CoV-2. A Ct of 38 or more is regarded as negative for the E-gene, while Ct of 40 or more is regarded as negative for the N-gene. (As suggested by the virology laboratory of the Abuja University Teaching Hospital. It is noteworthy that other laboratories use a lower cut-off point of 35).
The study was designed to detect a difference of 15% in the negativity rate by day 5 after dosing between the two arms [4], using the Wang and Chow formula [19], giving a total of 58 patients which was rounded up to 60. However, 65 patients were recruited in the end, of which 4 were dropped as a result of allergy to HCQ.
A standard clinical pharmacological randomization tool was applied. Sequential patients were assigned by chance to one of 2 treatments, A, B. Patients were asked to select from a pot of rolled papers labelled A or B. The numbers of papers labeled A or B were equal. This sequence was followed until the sample of 30/31 was attained in each of the 2 groups.
This was designed as a single-blind trial. The study was unmasked at the end of the trial after the analysis. However, arrangement was in place to unmask the trial in the event of a very Serious Adverse Event.
1. Viral load was assessed at enrolment (baseline) day 0, day 2, day 5, day 14 and day 21 after dosing. Proportion with negative PCR outcomes at days 2, 5, 14 and 21 were assessed for the two groups.
2. SpO2% was assessed using a pulse oximeter on a daily basis at approximately the same time of the day.
3. Symptom check list was assessed at baseline. These included the following:
• Respiratory symptoms: Cough
• GIT symptoms: Nausea, vomiting, diarrhea, abdominal pain
• CVS: Tiredness, lassitude, dyspnea
• CNS: Headache, Anosmia, Ageusia
• MSS: Myalgia
The following serious adverse events were monitored: Dizziness, diarrhea, vomiting, nausea, appetite loss, stomach pain, tiredness, others (to be specified)
4. Inflammatory markers were measured at baseline and day 7. These were Erythrocyte Sedimentation Rate (ESR), C-reactive Protein (CRP), and D-Dimer.
5. Hematological variables were measured at baseline and day 7, including Hemoglobin, White Blood Cells, Neutrophils, Lymphocytes and Platelet count. The Neutrophil/Lymphocyte ratio (NLR) was assessed as a measure of systemic inflammation.
Data was gathered into android tablets on JotForm platform and uploaded in real time unto the internet cloud, making it accessible by all researchers on the team. The data was ultimately translated into Excel and cleaned. Data was subsequently updated into STATA analysis package Stata/IC 16.1 for Mac (Intel 64-bit) and prepared for analysis.
Descriptive and inferential statistics (both parametric and non-parametric) was performed. Analysis of variance/Student t-test, and Chi-squared test were performed to assess effects of treatment on
1. Change in Viral load over time.
2. Change in Oxygen saturation over time.
3. Proportion negative at fixed end points.
4. Change in levels of inflammatory markers and hematological variables.
5. Change in clinical status over time using Likert scale: 1) Much worse/Very Bad; 2) Worse/Bad; 3) No change/average; 4) Improved/Good; 5) Much improved/Very good.
6. Disposition of patients was assessed on a daily basis with regards to whether 1. Treatment is maintained, 2. Patient is well enough to be discharged from active care, 3. Patient is referred for further treatment in Intensive care, or 4. The patient is deceased.
Repeated Measures Analysis of Variance (RMANOVA) was carried out to simultaneously measure Treatment (A v B) differences as Treatment effect and changes over time, as TIME effect. Time × Treatment interaction (whether treatment effects vary with time) was measured simultaneously on all test subjects at once for parameters indicated.
Statistical rejection of the null hypothesis was p < 0.05 and the 95% confidence Intervals quoted.
A Serious Adverse Event form was designed and completed for every case enrolled into the trial. Detailed clinical description of such adverse events was captured and evaluated. Immediate steps were taken to ameliorate such incidents.
The baseline values for both arms of the study were compared to assess the adequacy of randomisation (Table 1). The findings suggest that there are no significant differences in the two groups (Ivermectin only IVM and the HIA triple therapy (IVM+) group) with regards to all the variables. Age and sex were similar, as were dose of Ivermectin based on weight, need for supplemental oxygen, and need for ventilator. None of the patients had been vaccinated. Hematological indices such as hemoglobin, White Blood Count, Lymphocyte and Neutrophil count, and Neutrophil/Lymphocyte ratio, as well as Platelet count were comparable for both groups. There was also no difference with regards to viral load at baseline for both the N-gene and E-gene. Inflammatory markers such as ESR, C-reactive protein, D-dimer values were also similar in both groups. SpO2 was slightly higher for the Ivermectin only (IVM) group (93.8% versus 92.0%) but the difference was not statistically significant (p = 0.09). Clinical symptoms at baseline such as diarrhea (23.7%), anosmia (20%), ageusia (18%), dyspnea (25%), headache (50%) and cough (72.1%) were similar in both groups. Therefore, cough was the most common symptom with which patients presented, but was slightly less common in the IVM group.
Table 1: Baseline variables. View Table 1
Considering the two groups together, the average age of participants was 40.4 years, with more males (63%) than females. Figure 1 depicts the age distribution of the study participants. It indicates that the modal age group is between 25-30 years.
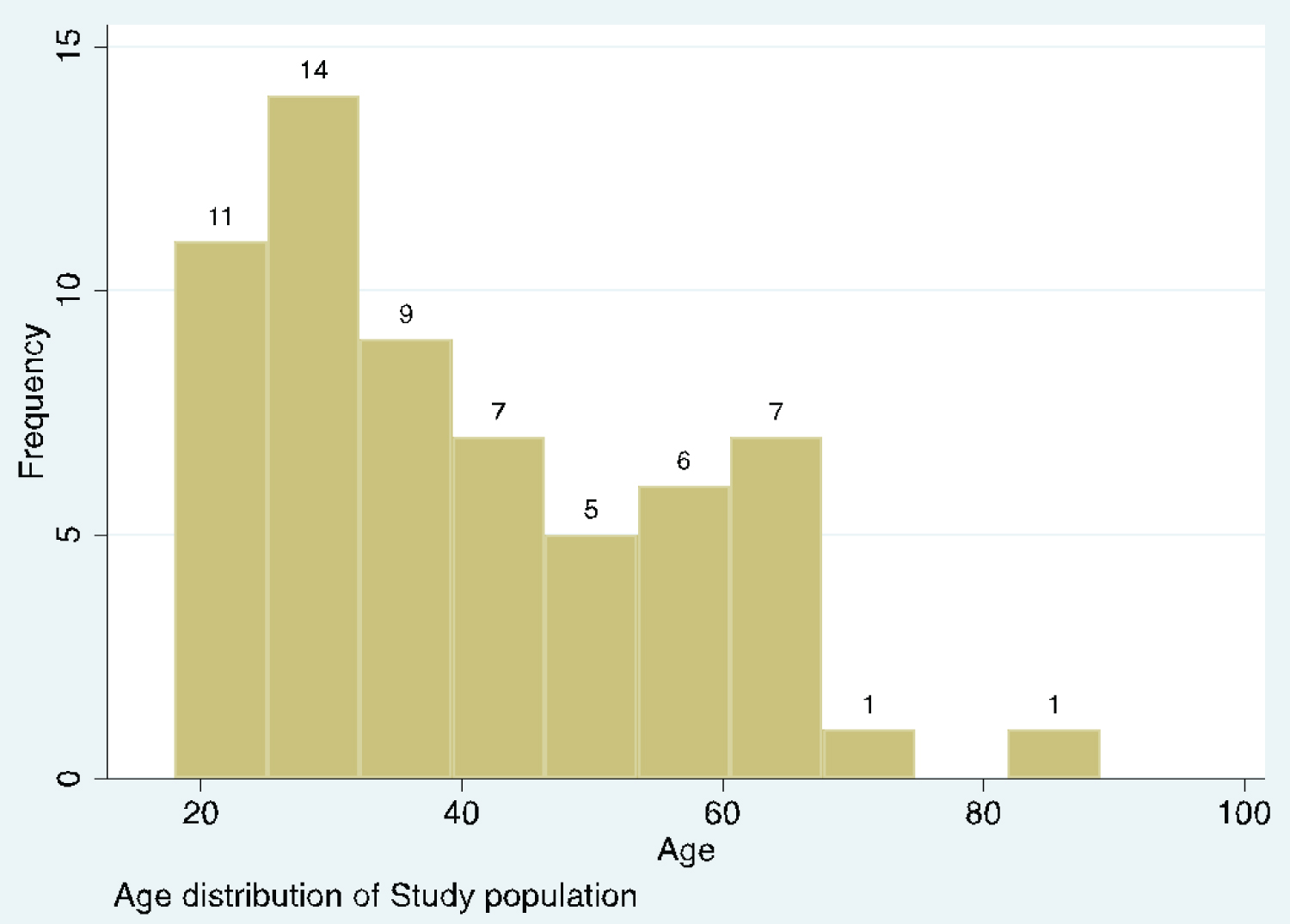 Figure 1: Histogram depicting age distribution of the patients.
View Figure 1
Figure 1: Histogram depicting age distribution of the patients.
View Figure 1
Based on the weight, the patients required an average of 5 tablets of 3 mg each (15 mg) daily. The hematological indices were within normal limits at baseline. These included Hemoglobin Hb, White Blood Cell count, Lymphocyte count, Neutrophil count, Neutrophil to Lymphocyte Ratio, and Platelet count. Viral loads at baseline were moderately high with mean CT counts of 26.5 and 21 for N and E-genes respectively. All these indices were similar in both groups.
With regards to the inflammatory markers, Erythrocyte Sedimentation Rate was within normal range, but the C-Reactive Protein was higher than normal at 14.6 mg/l, compared with a normal range of less than 10 mg/l.
D-dimer is the degradation product of factor XIII crosslinked fibrin. It reflects ongoing activation of the hemostatic system. The reference concentration of D-dimer is < 250 ng/mL.
A mean study D-dimer level of 222.2 ng/ml was thus within normal limits.
Mean entry SpO2% was low at 92.9%. Three of the patients had entry values of less than 80.
In the Federal Capital Territory (FCT) where this study took place, there are six Area councils (local governments). The most urbanized local governments are Abuja Municipal Area Council (AMAC) and Gwagwalada Area Council, where the teaching hospital and the main COVID isolation center is located. The majority of the patients come from these two urbanized area councils (Local Governments) (Figure 2).
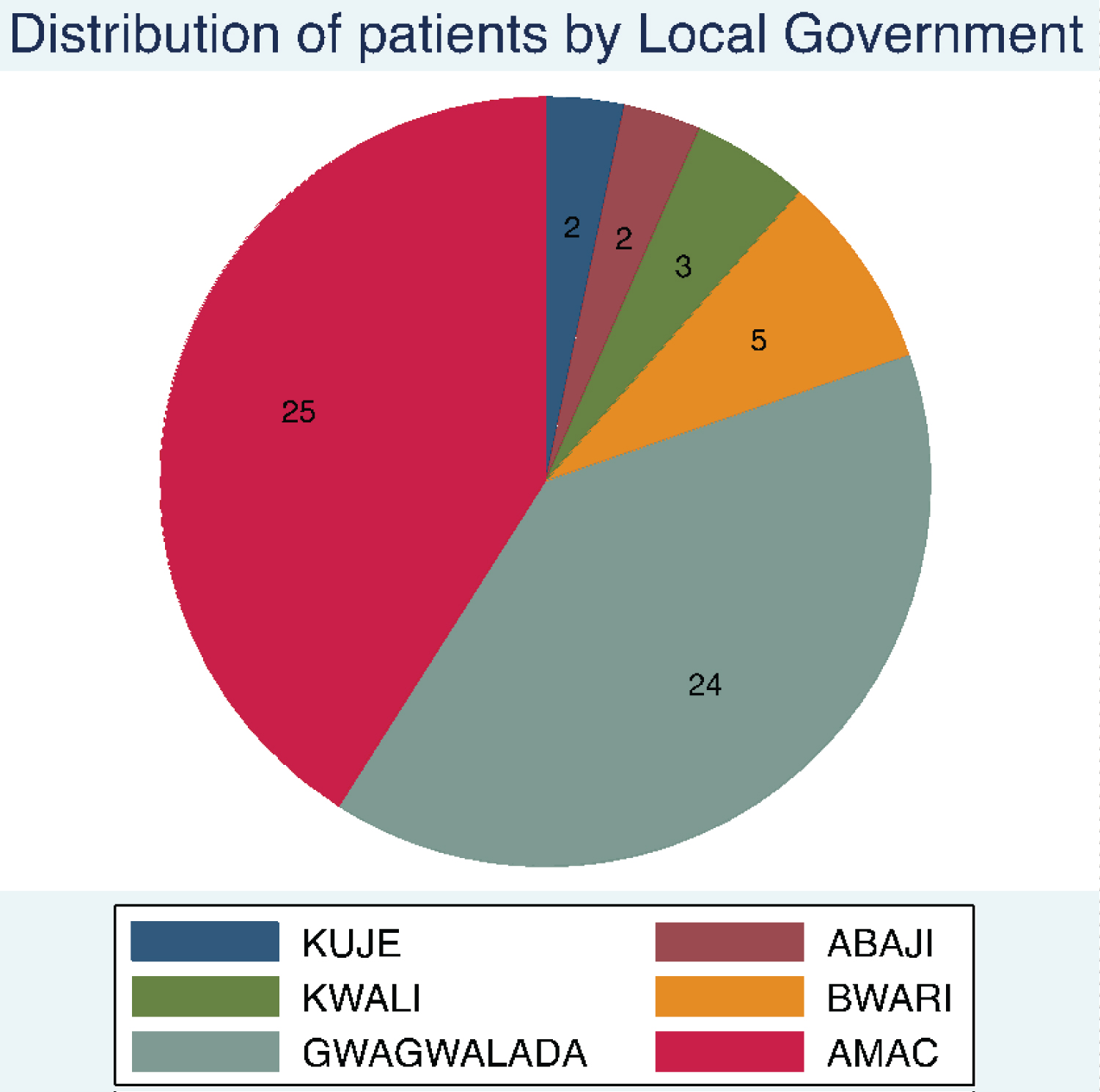 Figure 2: Distribution of patients by Area Council within the Federal Capital Territory. View Figure 2
Figure 2: Distribution of patients by Area Council within the Federal Capital Territory. View Figure 2
Table 2 quantifies changes over time, particularly between baseline and day 7. (Except for viral genes CT, which compares baseline and day 2).
Table 2: Changes in Laboratory parameters (mean values) in both arms of the study over time. View Table 2
A Repeated Measures Analysis of Variance (RMANOVA) was carried out on the cycle Threshold times for the N and E-genes respectively taking account of baseline (day 0), day 2, day 5 and day 14. There was a steady increase in CT values in both arms of the study. This increase was already significant by day 2 (p < 0.0001). Figure 3 and Figure 4 indicate change in N-gene and E-Gene cycle threshold respectively over time using adjusted predictions of treatment-by-day interaction with 95% confidence interval error bars. In both situations, there is no treatment difference between the IVM and IVM+ group. However, there is a significant time effect (p < 0.0001).
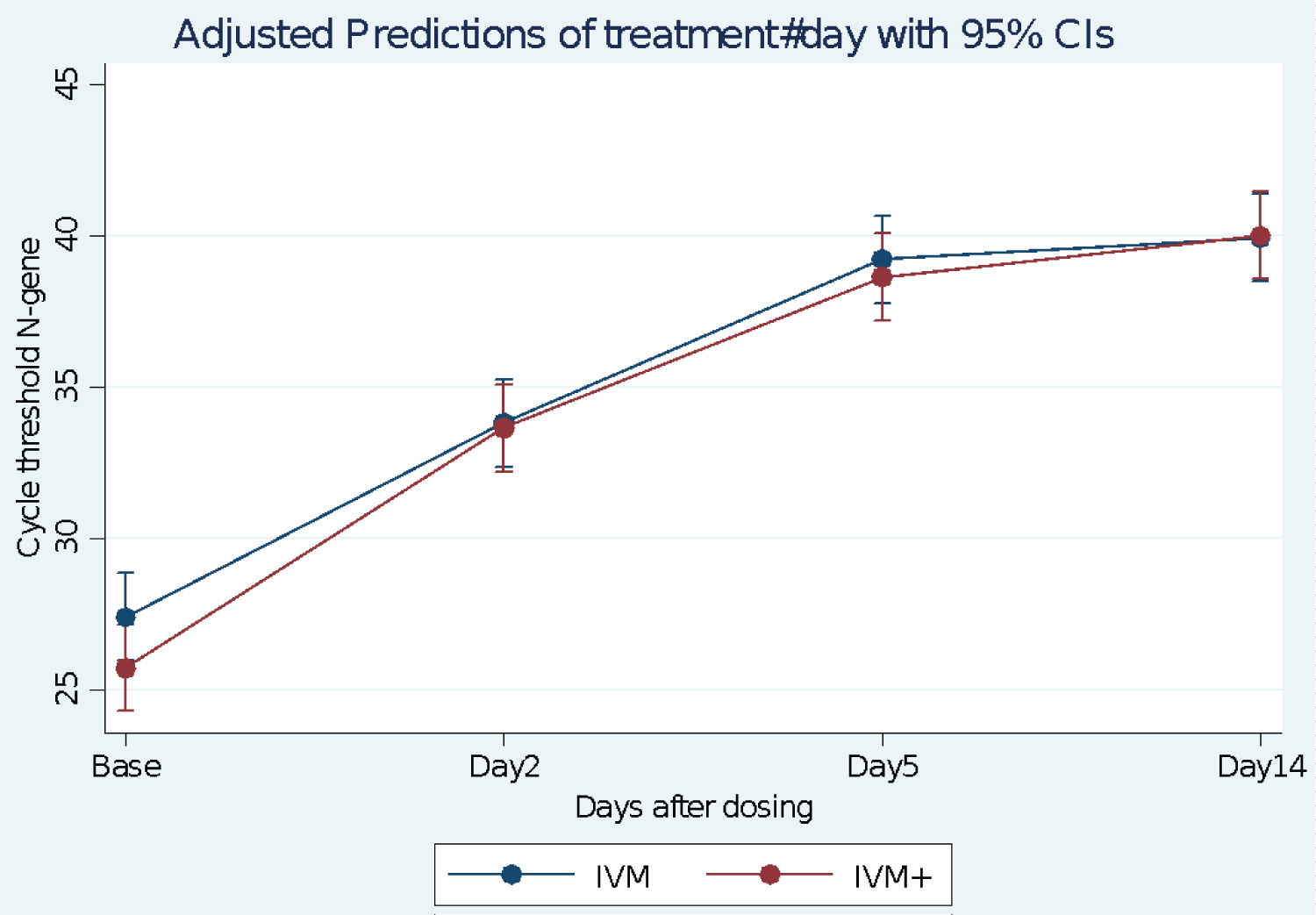 Figure 3: Change in N-gene cycle threshold over time using Adjusted Predictions of treatment-by-Day interaction with 95% Confidence Interval error bars.
Figure 3: Change in N-gene cycle threshold over time using Adjusted Predictions of treatment-by-Day interaction with 95% Confidence Interval error bars.
RMANOVA n = 30 No significant treatment effect, but a significant Time effect, p < 0.0001 ANOVA. There was no time-treatment interaction.
View Figure 3
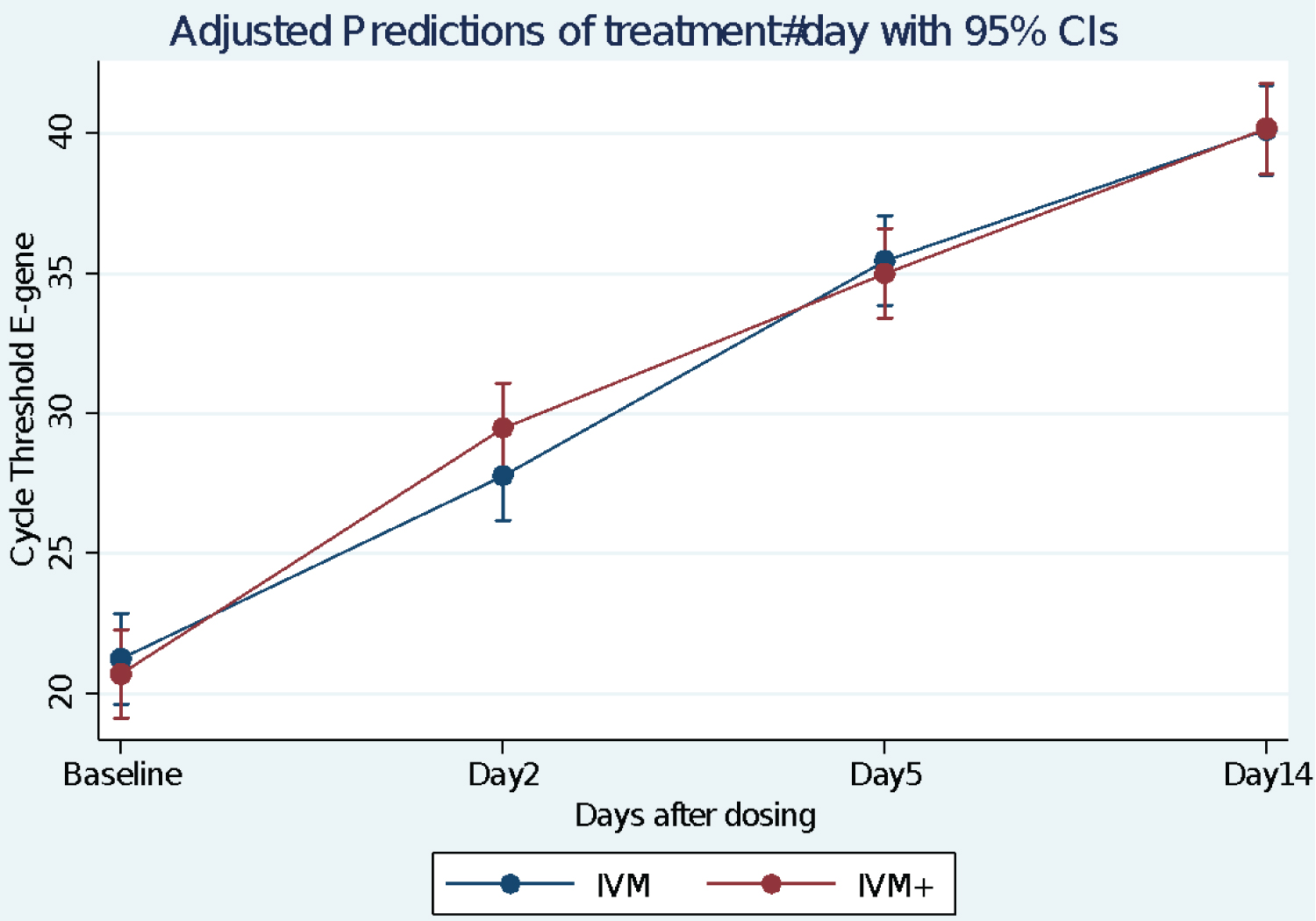 Figure 4: Change in E-gene cycle threshold over time using Adjusted Predictions of treatment-by-Day interaction with 95% Confidence Interval error bars.
Figure 4: Change in E-gene cycle threshold over time using Adjusted Predictions of treatment-by-Day interaction with 95% Confidence Interval error bars.
RMANOVA. n = 30. No Treatment Effect by 2-way repeated measures ANOVA. There was a significant Time effect, p < 0.0001 ANOVA. No time × treatment interactions.
View Figure 4
Table 3 indicates the progression of PCR test change from 'positive' to 'negative' as the days went by. This assumes a cutoff of N-Ct > 38 and E-Ct > 40. negative, one in each arm. (Other authors use a cutoff point of > 35 Ct as negative) RMANOVA of the N-Ct and E-Ct genes time-treatment interactions suggested that there was no treatment difference between the two arms, but there was a significant time effect in both arms, p < 0.0001. There was also minimal time × treatment interaction (Figure 3 and Figure 4).
Table 3: RT-PCR results (Positive/Negative) by Day in the study by treatment arm. View Table 3
Changes in SpO2%: RMANOVA analysis suggests that there is a significant time effect in both arms with a steady increase in SpO2%, p < 0.0001. There is a weak treatment × time interaction p = 0.10 from Likelihood Ratio Test. But there was no significant treatment difference between the two arms, p = 0.797 (Figure 5, Table 2 and Table 4).
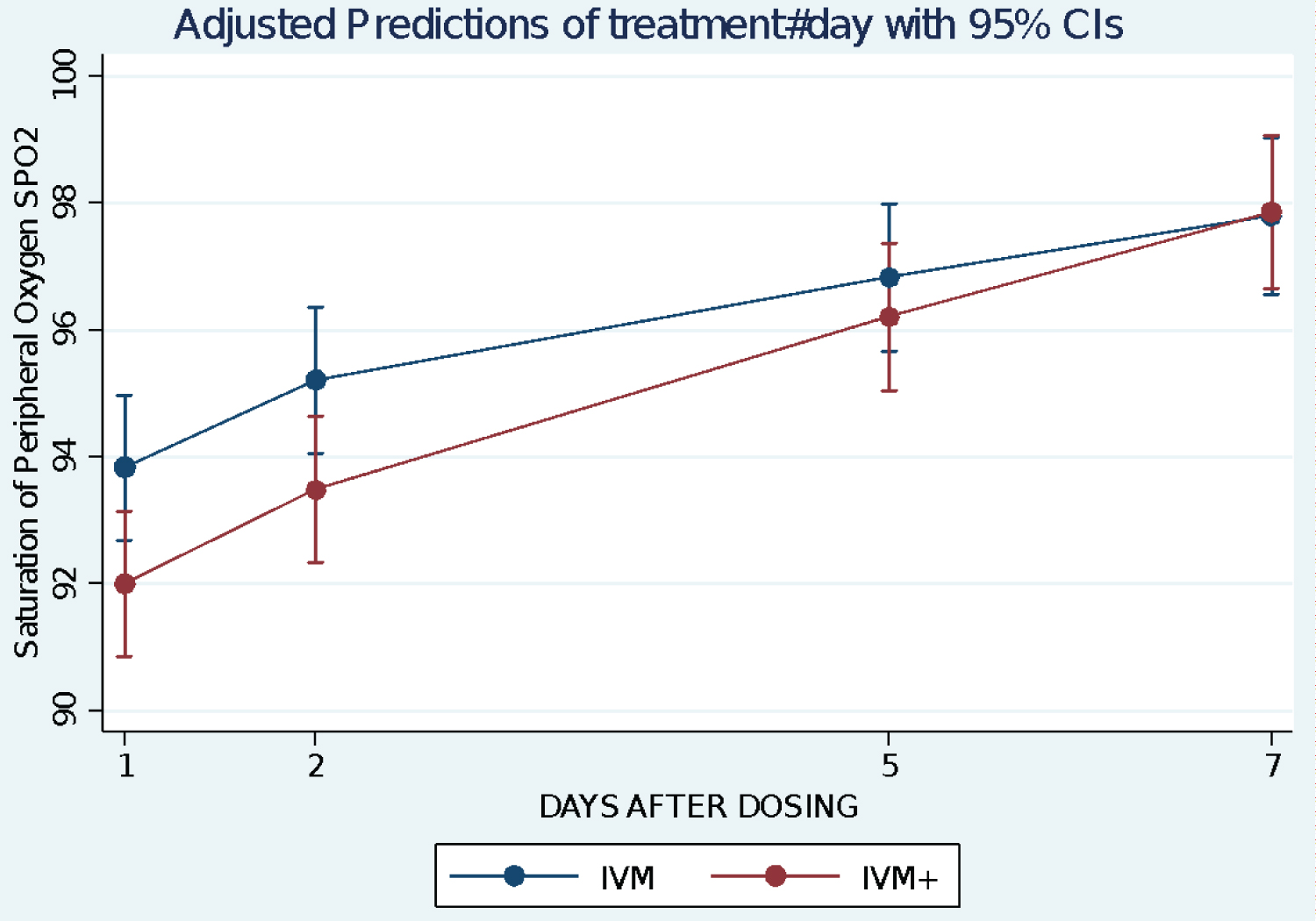 Figure 5: Change in arterial oxygen saturation SpO2 over time using Adjusted Predictions of treatment-by-Day interaction with 95% Confidence Interval error bars.
View Figure 5
Figure 5: Change in arterial oxygen saturation SpO2 over time using Adjusted Predictions of treatment-by-Day interaction with 95% Confidence Interval error bars.
View Figure 5
Table 4: Trend in Mean Percentage Saturation of Oxygen (SpO2%) by days after treatment. View Table 4
Inflammatory markers: For the two arms of the study, there was a statistically significant drop in the levels of all the inflammatory markers by day 7 relative to baseline. (ESR p < 0.0025, D-dimer p < 0.0001and CRP, p < 0.0001) (Figure 6, Figure 7 and Figure 8). The drop was steeper in the IVM arm (except for CRP where the drop was parallel), but the difference between the two groups was not statistically significant both at baseline and by Day 7.
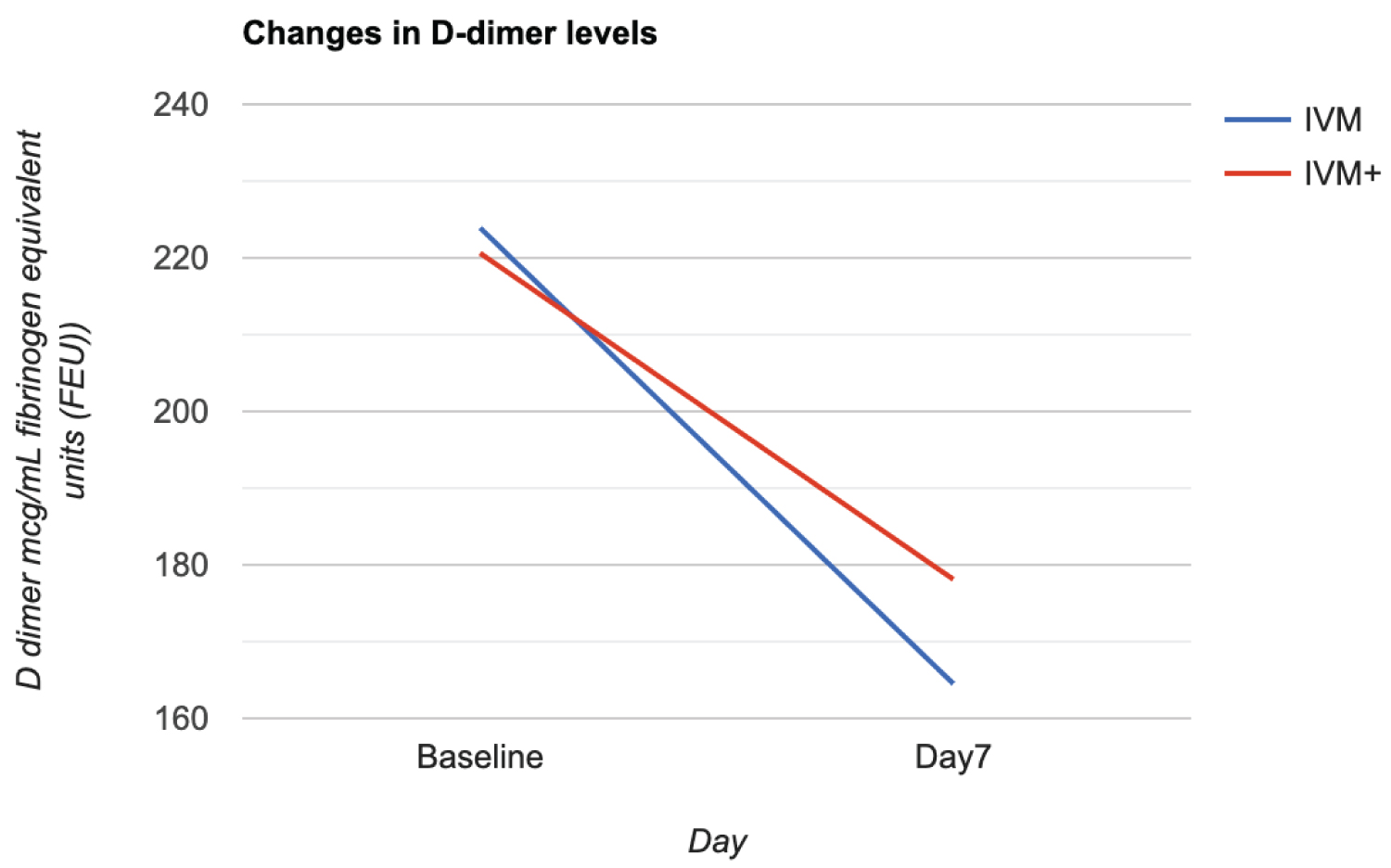 Figure 6: Change in D-Dimer levels from baseline to Day 7 in the two treatment arms IVM and IVM+.
View Figure 6
Figure 6: Change in D-Dimer levels from baseline to Day 7 in the two treatment arms IVM and IVM+.
View Figure 6
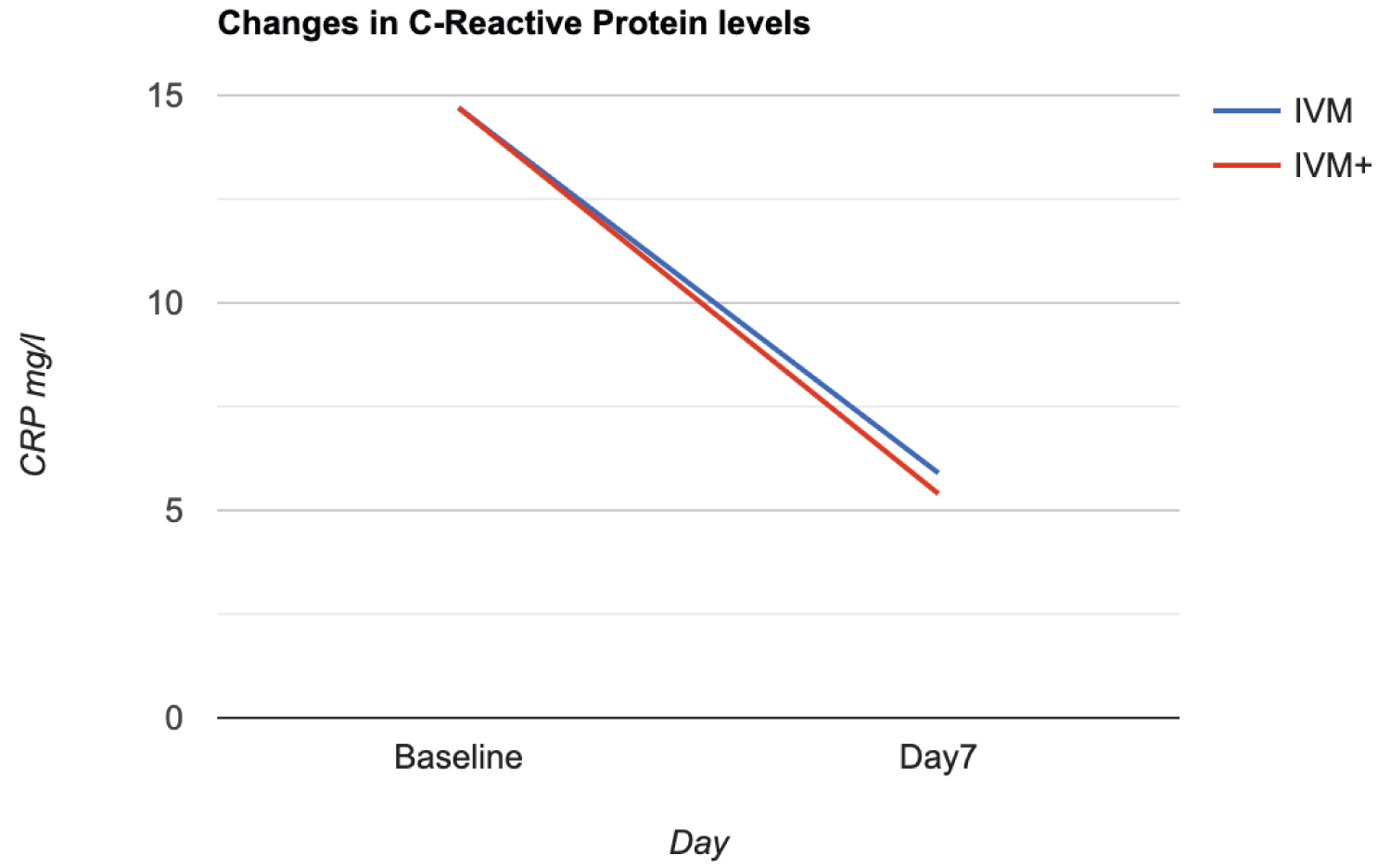 Figure 7: Change in C-Reactive Protein levels from baseline to Day 7 in the two treatment arms IVM and IVM+.
View Figure 7
Figure 7: Change in C-Reactive Protein levels from baseline to Day 7 in the two treatment arms IVM and IVM+.
View Figure 7
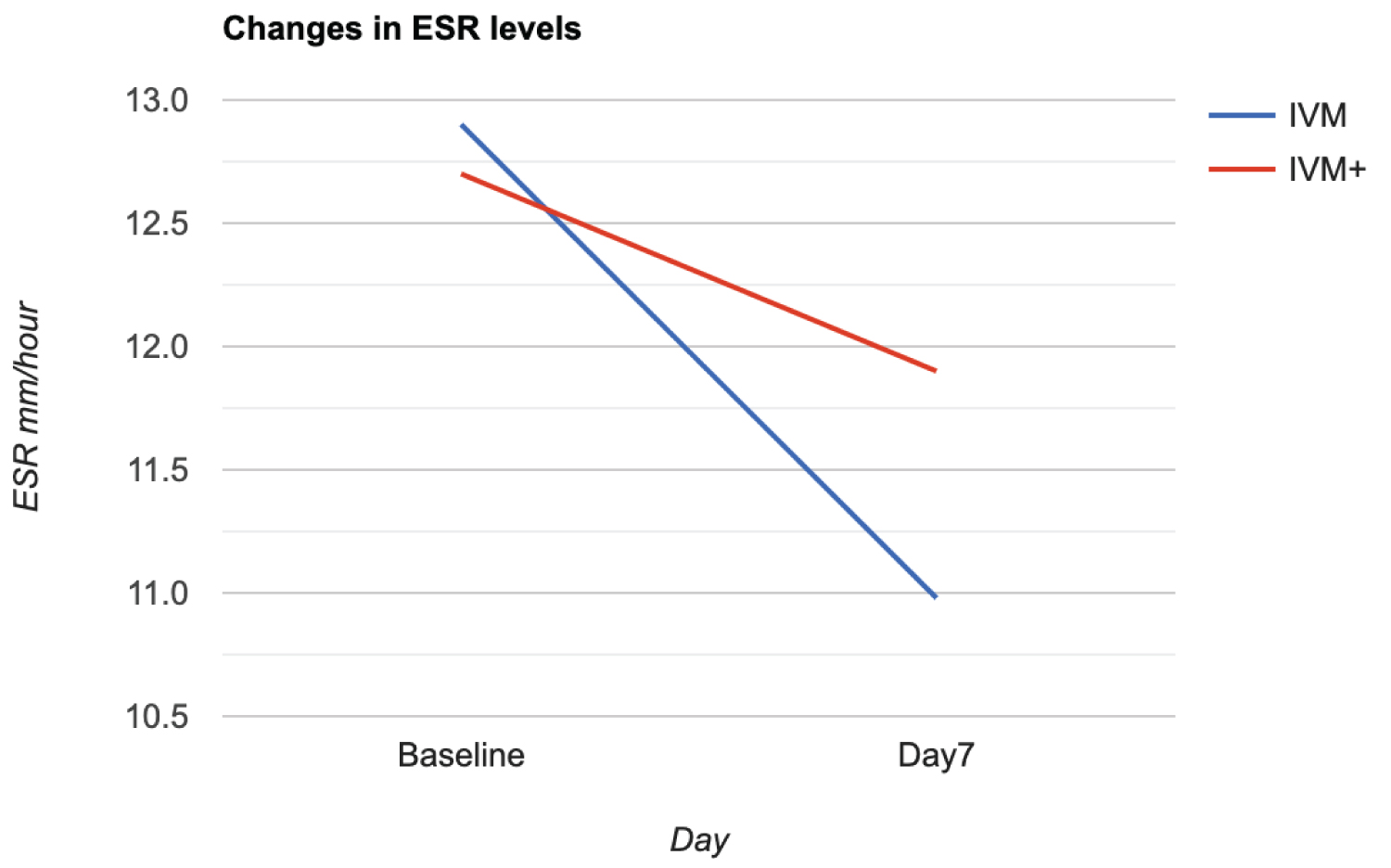 Figure 8: Change in ESR levels from baseline to day 7 p = 0.0025.
View Figure 8
Figure 8: Change in ESR levels from baseline to day 7 p = 0.0025.
View Figure 8
Hematological variables were assessed. There was an insignificant drop in Hemoglobin levels by day 7 in both arms P = 0.138. But there was a significant drop in the WBC count overall (p < 0.0002), with a similar degree of drop in both arms.
There was overall no statistically significant decrease in the lymphocyte count. However, there was a slight increase in the IVM arm of 0.27 × 109 cells/l as opposed to a decrease in the IVM+ arm (2.2 × 109). This difference in direction did not achieve statistical significance p = 0.233. Difference -3.16, 95% CI -8.42-2.49.
There was however a significant decrease in the Neutrophil count across both arms compared to baseline (p = 0.0006) with a consequent decrease in the Neutrophil to Lymphocyte ratios, more so in the IVM arm. 0.23 versus 0.08.
There was also a significant drop in the platelet counts across arms (p < 0.0001) more so in the IVM arm (47% drop) than the IVM+ arm (18.7% drop). However, the difference in percentage drop did not achieve statistical significance (p = 0.155). Figure 9 (Actual difference was 25.8 95%CI -10.0-61.8).
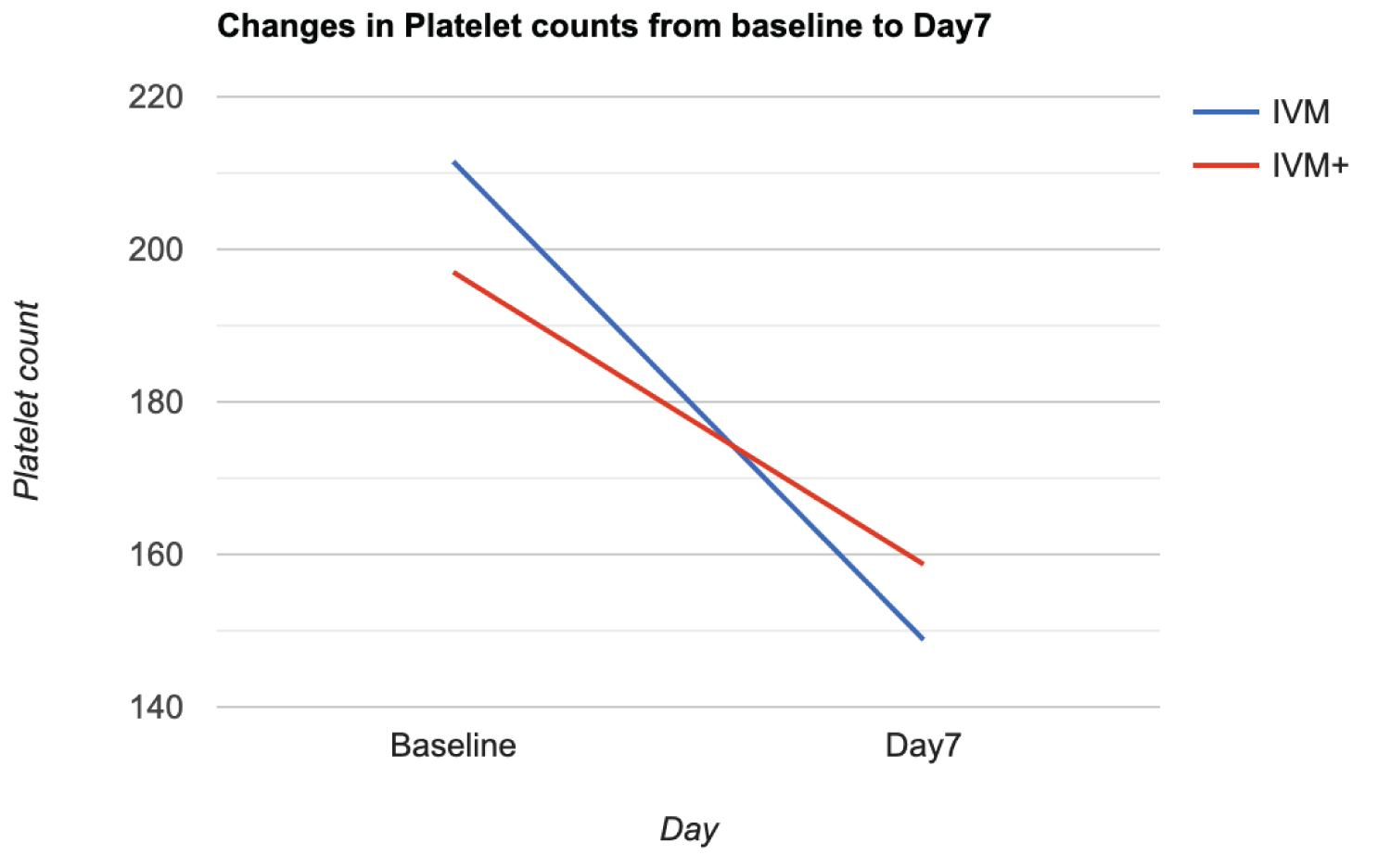 Figure 9: Changes in platelet count from baseline to day 7.
View Figure 9
Figure 9: Changes in platelet count from baseline to day 7.
View Figure 9
The clinical status was reported by the patients on a Likert scale in response to the question 'How do you feel today?' ranging from 1 (much worse) to 5 (much improved). Figure 10 indicates that in both arms there was a steady progress in mean wellness scores. Assuming no time treatment/interaction, there is no difference between the two groups p = 0.760. However, there is a significant improvement with time in both arms. p = 0.102 by day 2 and p = 0.000 by day 5. By day 11, average Likert scores was over 4.5 in both arms marginally higher in the IVM+ arm (p = 0.0731).
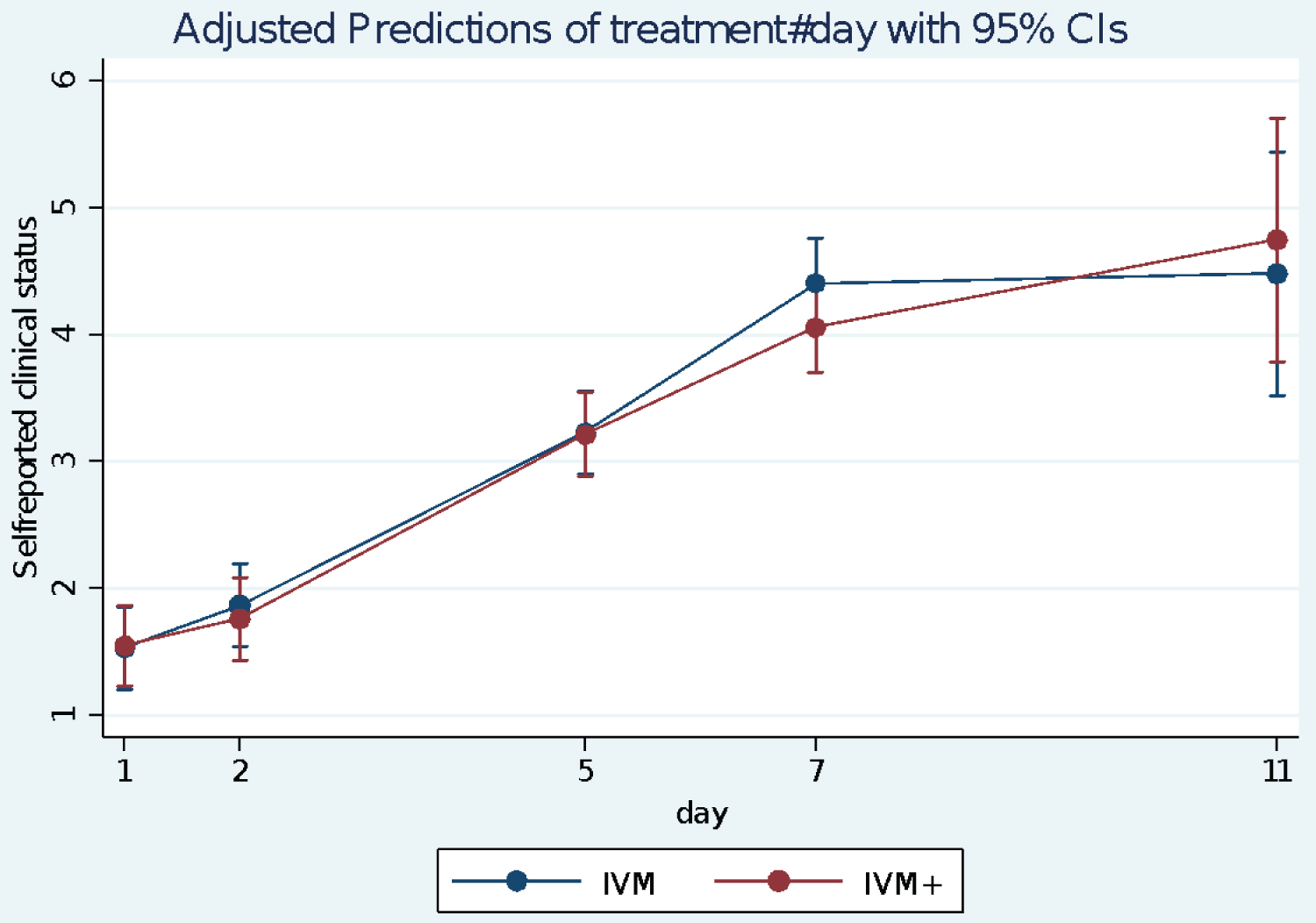 Figure 10: Self-reported Clinical status of patients over time using Adjusted Predictions of treatment-by-Day interaction with 95% Confidence Interval error bars. 1- Much worse/very bad; 5- Much improved/Very good.
View Figure 10
Figure 10: Self-reported Clinical status of patients over time using Adjusted Predictions of treatment-by-Day interaction with 95% Confidence Interval error bars. 1- Much worse/very bad; 5- Much improved/Very good.
View Figure 10
The likelihood of being discharged by day 7 in either arm of the study: Patients were discharged after negative PCR test, their perception of wellness, and the absence of concerning signs and symptoms such as fever, cough, myalgia and malaise. 63% of patients in the IVM arm were discharged as compared to 44% in the IVM+ arm by day 7. OR 2.13 (95% CI 0.63-7.27) p = 0.172. Thus, there is a weak suggestion that patients are more likely to be discharged by day 7 in the IVM arm, but this did not achieve significance (Table 4).
Complaints/Adverse events were recorded on a daily basis and depicted in Figure 11. It is difficult to know which complaints are due to the disease and which are due to the drug, but all are assessed together. A total of 11 patients had complaints of one form or the other on the first day of treatment, 8 in the IVM group and 3 in the IVM+ group. Complaints in IVM group included tiredness (4), and one each of stomach pain, nausea, vomiting and dizziness. Only 3 people had complaints in the IVM+ group, of stomach pain. By day 2, 4 people still complained of tiredness, and two of stomach pain in the IVM arm, while 3 people complained of tiredness in the IVM+ arm. There was an overall decrease in the number of complaints by day 5, by which time only 3 people complained.
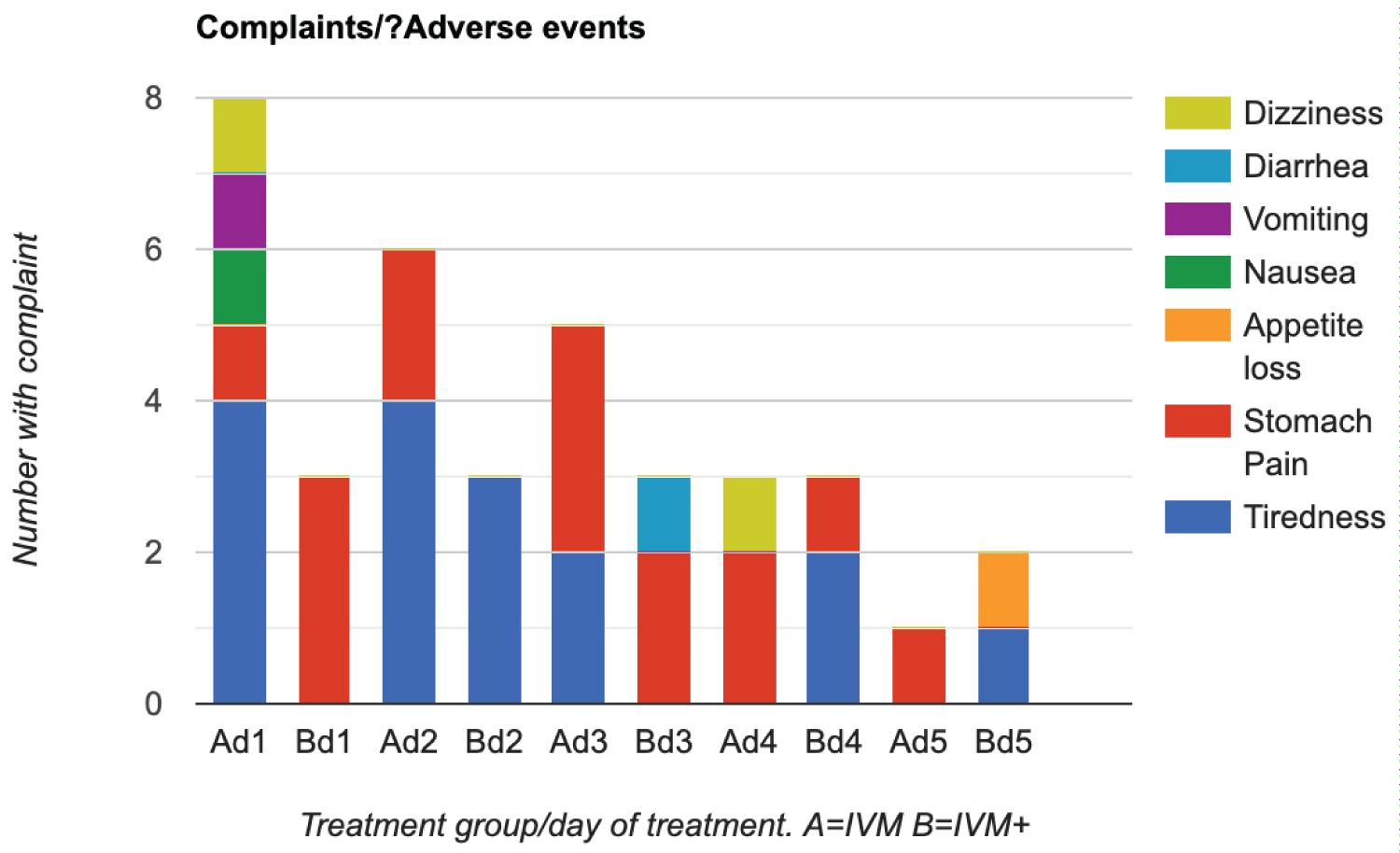 Figure 11: Occurrence of Adverse reactions/ main clinical complaints.
Figure 11: Occurrence of Adverse reactions/ main clinical complaints.
Key: Ad1 significant complaints on day 1 in IVM group
Bd1 significant complaints on day 1 in IVM+ group
Ad2 significant complaints on day 2 in IVM group etc.....
View Figure 11
Overall, there were 23 complaint events in the IVM group compared to 14 in the IVM+ group. However, four subjects in the IVM+ group had been dropped from the study because of reaction to HCQ, and do not form part of this analysis. Their reaction, mainly consisting of itchiness, had not responded to Loratadine. Two other subjects developed severe itching around the armpits attributable to HCQ, but were successfully treated with Loratadine, and so continued in the study and form part of this analysis.
The clinical, virological, inflammatory, and respiratory (SpO2%) comparative assessments, which are hard end points of our randomized controlled study, did not show a significant difference between IVM monotherapy and HIA triple therapy in the RT PCR positive COVID-19 patients. This finding indicates that a combination of AZT + HCQ did not confer any additive benefit to IVM in virucidal action against SARS-CoV-2. The results however, confirm and extend our earlier results on the anti-SARS-CoV-2 efficacy of Ivermectin alone [4].
In this study, we demonstrate further that Ivermectin alone, or with HIA rapidly increased the cycle time (Ct) of the N-gene (nucleocapsid) and the E-gene (envelope) of the SARS-CoV-2 and achieved significant COVID negativity on Day 7 on RMANOVA (Figure 3 and Figure 4).
The possible explanation of the lack of additional or superior efficacy of HIA over IVM is not clear. First, it can be postulated that, IVM with its multiple mechanisms of anti-SARS-CoV-2 actions [4,5], which incidentally includes the modes of action both of AZT and HCQ [6-9,14,15], early onset pharmacodynamics and near maximal efficacy, leaves no opportunity for enhanced efficacy for Azithromycin and HCQ, which have a higher IC50 for SARS-CoV-2 inhibition [12,13]. It is likely that drugs with divergent mechanisms of Anti SARS-CoV-2 such as Molnupiravir [5], may exhibit synergism in virucidal activity when combined with IVM.
Although some studies indicated the benefit of AZT + HCQ in COVID-19 [6,20], this is not a universal finding [21]. HCQ was discontinued in the RECOVERY study because of lack of efficacy and cardiac adverse effects [18].
Additionally, it has been reported that HCQ/CQ does not inhibit SARS-CoV-2 in human lung cells/Calu-2 cells [13].
HCQ is also less efficient in blocking viral cell entry in Vero-6 cells and in inhibiting viral replication in the lungs [12,22].
It is thus plausible that AZT + HCQ was effectively a placebo in the combination and did not exert any independent virucidal activity.
CQ/HCQ exerted no cardiac adverse effects which had been reported in other populations, as no patient had any cardiac dysrhythmic symptoms. This safe cardiac trend is compatible with the experience with chloroquine treatment of malaria in this hyperendemic zone for more than half a century. Inter-ethnic differences in QT elongation response to chloroquine has also been noted by Shah, et al. [23], who suggest that Africans may not be as prone as Caucasians to CQ induced cardiotoxicity.
IVM and HIA were associated with improved SpO2% over 7 days by RMANOVA (Figure 5). Although no treatment difference was discernible, the time effect of p < 0.0001 was likely due to the treatment with Ivermectin in both arms, as it was shown to increase SpO2% in our earlier study [4] . This is highly suggestive of a prevention or reversal of any respiratory vascular damage, which is a hallmark of COVID-19.
In addition, Osman, et al. and Annunziata, et al. have documented changes in SpO2 in non-ivermectin treated COVID-10 patients [24,25]. These two studies show unequivocally that there is an initial dip in SpO2 towards day 8 before a recovery towards day 14. This contrasts with our study in which SpO2 increases from day 1 on ivermectin and is at normal levels by day 7 in both arms of the study. The mechanism of this effect on SpO2 by ivermectin is a subject of ongoing investigations.
IVM and HIA were both associated with significantly reduced pro-inflammatory markers CRP, ESR and D-dimer (Figure 6, Figure 7 and Figure 8) indicative of antithrombotic and cytokine reduction effects of Ivermectin via STAT-3 inhibition as we have previously suggested [4].
Possible side effects of Ivermectin: As noted above, there was an overall decrease in the number of complaints by day 5. This suggests that the dose of Ivermectin used in this study is safe and efficacious.
Duration of treatment with ivermectin: In our previous study, we had utilized a twice weekly 12 mg dose of ivermectin. However, we felt that a five-day course would probably help in the build-up of ivermectin to therapeutic doses and hence utilized this regime in this study. Ahmed, et al. [26] had equally used a five-day Ivermectin regime and did not report serious adverse events of concern.
Inhibition of efficacy: We did not see evidence of inhibition of efficacy in this study. There appears to be a marginal increase in likelihood of RT-PCR negativity by day 5 in the IVM+ arm, but this did not achieve statistical significance. Reduction in level of inflammatory markers was less for the IVM+ group, but this did not achieve statistical significance.
We have had no non-ivermectin controls in this study for ethical reasons. Our own previous study [4] and meta-analysis by Kory, et al. [27], Bryant, et al. [28] and Hill, et al. [29], as well as information obtainable from the ivmmeta.com website [30], details the advantages of ivermectin over controls in terms of mortality, viral clearance, clinical recovery and prophylaxis. A summary of these improvements as obtained from the October 29 2021 edition of the ivmmeta.com website is detailed in Table 5. It suggests a 56% improvement in mortality, 52% improvement in recovery, 59% improvement in viral clearance and 86% improvement in prophylaxis. Hence, we felt justified in not using a non-ivermectin control in this study.
Table 5: Extract from Ivermectin treatment for COVID-19: real time meta-analysis of 64 studies. View Table 5
In conclusion, there was no significant treatment difference between IVM monotherapy and HIA triple therapy, thus suggesting that AZT + HCQ may be redundant adjuncts in COVID-19 therapy in Nigerians and elsewhere. There was a highly significant time effect (p < 0.0001 RMANOVA) indicating that the improvements in SARS-CoV-2 N and E-gene Ct, as well as the SpO2% are likely due in large part to Ivermectin virucidal and anti-inflammatory actions.
Tobi Babalola for work on the data collection platform. Professor Simon Cousens (LSHTM) for help with statistical analysis.
PACTR202108891693522.
This project was funded by the Central Bank of Nigeria Health Sector Research and Development Intervention Scheme.