Disseminated tuberculosis is a leading cause of morbidity and mortality in developing nations. It could be a diagnostic challenge because of the nonspecific manifestations and sometimes atypical laboratory and radiologic findings. It results from haematogenous spread of Mycobacterium tuberculosis in 2 or more noncontiguous sites. Clinical features may include fever, weight loss, anorexia, anemia, pancytopenia, hepatosplenomegaly and most times, patients have elevated inflammatory markers like erythrocyte sedimentation rate (ESR). Delay in diagnosis and treatment could portend a poor clinical outcome for the patient. Therefore, a high index of suspicion is crucial for early diagnosis and management.
We present a case of a 52-year-old man who presented with a 5-month history of fever, 3-month history of weight loss with 6-week history of body weakness. Haematologic parameters revealed pancytopenia and abdominopelvic ultrasound showed hepatosplenomegaly. Erythrocyte sedimentation rate and chest X-ray were normal. Patient died after few days on admission and post-mortem examination was in keeping with disseminated tuberculosis, with liver, spleen, pancreas, para-aortic lymph nodes, pleural, omentum and stomach wall involvement.
Disseminated tuberculosis, Pancytopenia, Erythrocyte sedimentation rate, Granuloma
Tuberculosis (TB) is a chronic infectious disease, principally caused by the bacillus, Mycobacterium tuberculosis (Mtb) [1]. The World Health Organization (WHO) reported that approximately 10 million people were infected with Mtb in 2019; out of which about 1.2 million deaths occurred among human immunodeficiency virus (HIV)-negative people, with an estimated 208,000 deaths found to be related to HIV-positive individuals [2]. It is a leading cause of morbidity and mortality in developing countries, where about 7% of all deaths have been attributed to TB and amongst adult patients, TB is regarded as the most common cause of death from a single source of infection [1,3]. Two continents of the world, namely Asia and Africa account for 86% of all cases of TB [4]. Though it primarily affects the lungs, there could however be manifestation of the infection in different organs of the body [1,5]. Disseminated tuberculosis (DTB) results from haematogenous dissemination of Mycobacterium tuberculosis in two or more noncontiguous sites, either from a progressive primary infection or reactivation of a latent focus followed by a spread [5,6]. DTB accounts for < 2% of all cases of TB and up to 20% of all extrapulmonary TB cases in immunocompetent persons [5,6]. It could be a life-threatening disease, especially if diagnosis and treatment is delayed. DTB has been noted to be a major cause of morbidity and mortality in developing nations, particularly among children, but cases have been reported in developed nations and it could affect persons of different ages with immunosuppressive states like HIV infection/acquired immunodeficiency syndrome (AIDS), use of biologicals and immunosuppressive drugs for the treatment of medical conditions, increasing prevalence of organ transplantation, alcoholism, chronic liver disease, chronic haemodialysis, diabetes mellitus, malignancies, and silicosis [5-7]. Organs involved include liver, spleen, bone marrow, kidney, adrenals, eyes, and thyroid [5]. The clinical presentation of DTB is variable and could follow a subtle, insidious course and this together with delayed presentation of some of the patients make prompt diagnosis a challenge [5,6,8]. Patients may present with fever of unknown origin, weight loss, anorexia, hepatosplenomegaly and elevated erythrocyte sedimentation rate (ESR) [5,9,10]. Different haematologic abnormalities have also been reported including anemia, neutropenia, lymphopenia, leukemoid reaction but rarely pancytopenia [5,8,9]. There are scanty reports of pancytopenia in patients with DTB in sub-Saharan Africa. We report a case of an adult male with unusual clinical manifestation of disseminated tuberculosis, who presented with fever, weight loss, anorexia, with hepatosplenomegaly, pancytopenia but normal ESR and Chest X-ray.
A 52-year-old Nigerian male, Secondary school instructor, presented to the emergency department of the hospital with a 5-month history of high grade, intermittent fever, 3-month history of weight loss and 6-week history of progressive body weakness. There was associated anorexia, malaise and diaphoresis. There were no reports of chest or abdominal pain, change in bowel motions or painful urination. He had a mild transient unproductive cough at the onset of illness but this resolved spontaneously. There was no preceding upper respiratory tract illness, known COVID-19 or cough contacts and no hemoptysis.
Two months later, he noticed weight loss which was evidenced by loss of fitting of previously well-fitted clothings. He had no recurrent diarrhea, yellowish eye discoloration, anterior neck swelling or obvious glandular body swellings. He reported associated generalized body weakness which gradually worsened about 6 weeks prior to presentation. There was no difficulty with breathing, awareness of heartbeat, orthopnea or paroxysmal nocturnal dyspnea. He also noted mildly progressive abdominal swelling with early satiety and occasional dark-coloured urine but no pale bulky stools or body itchiness. There was no observed bleeding from body orifices or easy bruisability. He however reported an episode of passage of dark coloured stool about a week prior to presentation. He had two units of blood transfused in the referring hospital. The abdomino-pelvic ultrasound done showed enlarged spleen with a span of 22.3 cm and ascites.
He had no known intercurrent illnesses and denied use of herbal preparations. No exposure to petrochemicals and agrochemicals. The hepatitis B status as well as history of multiple sexual partners were unknown. He took about 18-20 units of alcohol per week for 25 years and smoked cigarettes for about 7 pack years. His genotype was AA. He was married in a monogamous setting with children. He was unaware of any family history of gastrointestinal or blood disorders. He reacted by itching to co-trimoxazole.
The findings on examination noted an ill-looking male who was febrile with temperature of 39 degrees celsius. He was pale, not icteric but had mobile non-tender medial axillary lymphadenopathy, palpable bilaterally with left epitrochlear lymph nodes (1.5 × 1 cm). There was mild bilateral pitting edema up to the lower third of the legs bilaterally. The abdomen was full, moved with respiration with no area of tenderness. The liver was palpable 6 cm below the right coastal margin with a span of 17 cm. The spleen was palpable 8 cm below the left coastal margin - firm and non-tender. Ascites was difficult to demonstrate clinically. The digital rectal examination was not remarkable. The pulse was 120 per minute, regular and of normal volume with blood pressure of 90/50 mmHg. First and second heart sounds only were heard. The respiratory rate was 36 breaths per minute; the remainder of the chest as well as neurological examination was not remarkable. The Complete blood count showed pancytopenia, other laboratory investigations are as shown in Table 1. The Chest roentgenogram was essentially normal. A repeat abdomino-pelvic ultrasound scan done 72 hours prior to this evaluation showed enlarged liver with echogenic parenchymal echotexture, enlarged spleen with markedly altered architecture and an 8 cm deep ascites in the pelvis. Initial assessment was that of haematologic malignancy (likely lymphoma), with differentials of chronic liver disease and disseminated tuberculosis.
Haematology consults documented absence of petechiae hemorrhages on review of the skin and integuments. The peripheral smear showed microcytes, hypochromic cells, macrocytes, elliptoid cells, pencil cells with red cell fragments. The neutrophils showed toxic granulations as well as Pegler Huet anomaly. At a Gastroenterology review, he corroborated a history of mild difficulty swallowing requiring passage of a nasogastric tube at the other hospital with subsequent improvement but there was no painful swallowing, regurgitation or halitosis. He was scheduled for an upper gastro-intestinal endoscopy. The repeat laboratory tests showed worsening of the tests of excretory as well as synthetic functions of the liver as shown in Table 1. The results of electrolytes, urea, creatinine were normal and tests for hepatitis B, hepatitis C and retroviral screen were negative. He was transfused with two units of fresh whole blood and one unit of fresh frozen plasma on account of raised international normalized ratio (INR). The Erythrocyte sedimentation rate obtained via the Westergreen method was 15 mm in the first hour. On the sixth day of in-patient care, he was noted to have clinically deteriorated - with laboured breathing and a blood pressure of 60/30 mmHg. Minutes later, he developed cardio-respiratory arrest. Resuscitation protocols were promptly instituted but proved futile.
Table 1: Shows the results of laboratory investigations done with their normal reference ranges, before and during hospital admission. View Table 1
Post-mortem examination done showed markedly enlarged spleen which weighed 1380 g (Normal: 40-135 g) and riddled with greyish white nodules of varying sizes. The cut surface showed multiple greyish white areas with intervening areas of congestion (Figure 1A and Figure 1B). Microscopy revealed distortion of the splenic architecture by extensive areas of chronic necrotizing granulomatous inflammation with numerous inflammatory type (langhan's and foreign body type) giant cells with marked expansion and congestion of the red pulp (Figure 1C and Figure 1D).
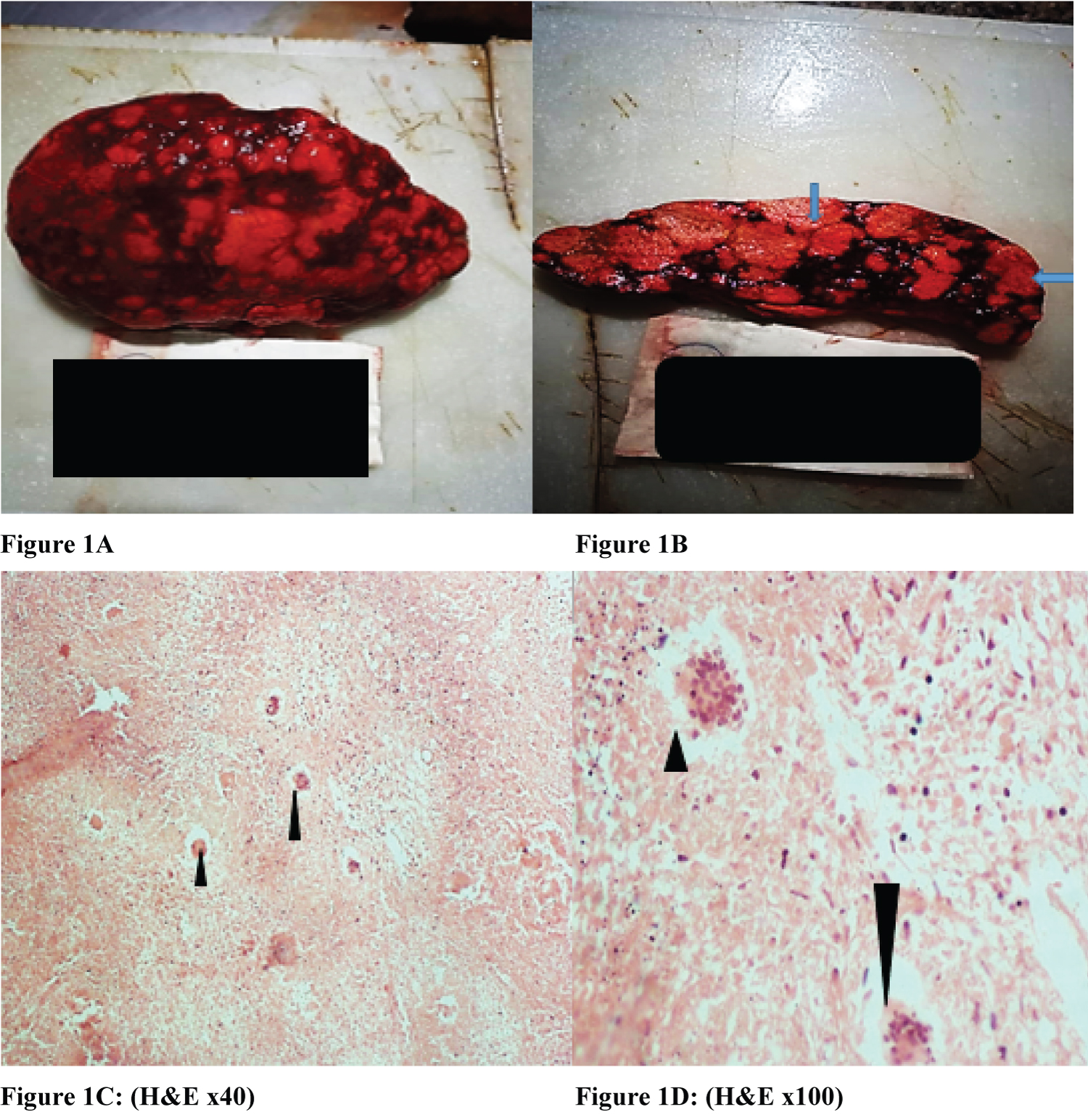 Figure 1: (A) Enlarged spleen with diffuse greyish white nodules of varying sizes; (B) Cut surface of the spleen showing multiple greyish white areas (arrows) with intervening areas of congestion; (C) (H&E x40) Arrowheads- Numerous inflammatory giant cells; (D) (H&E x100) Arrowheads- Numerous inflammatory giant cells.
View Figure 1
Figure 1: (A) Enlarged spleen with diffuse greyish white nodules of varying sizes; (B) Cut surface of the spleen showing multiple greyish white areas (arrows) with intervening areas of congestion; (C) (H&E x40) Arrowheads- Numerous inflammatory giant cells; (D) (H&E x100) Arrowheads- Numerous inflammatory giant cells.
View Figure 1
The liver was enlarged, with a weight of 2050 g (Normal: 1200-1600 g) and section showed areas of nodular aggregates of necrotizing granulomas and steatosis (Figure 2).
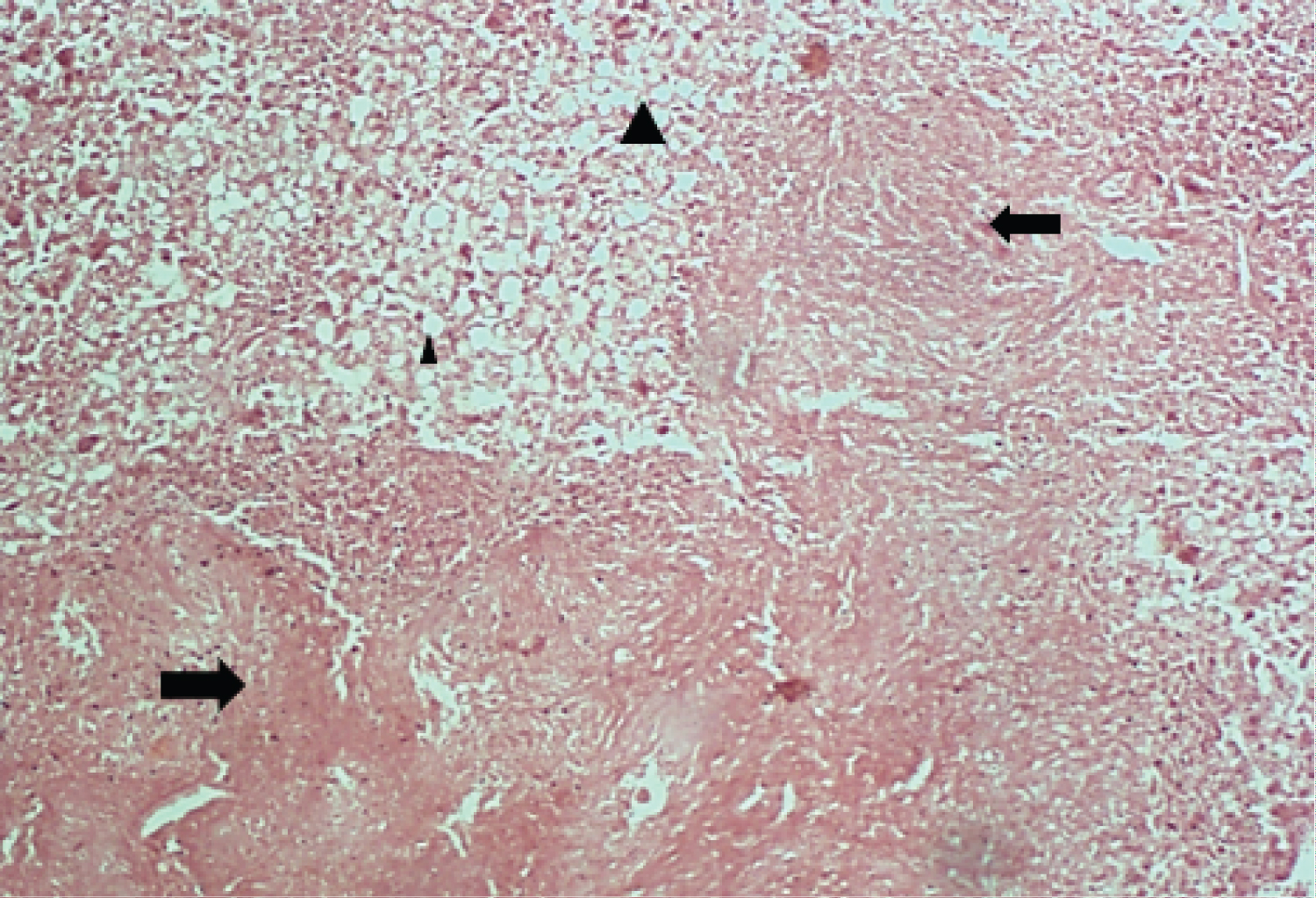 Figure 2: (H&E x 100)- Arrow- Nodular aggregates of necrotizing granulomas; Arrowheads- Steatosis. View Figure 2
Figure 2: (H&E x 100)- Arrow- Nodular aggregates of necrotizing granulomas; Arrowheads- Steatosis. View Figure 2
Also, there was enlargement of the para-aortic groups of lymph nodes and section of the lymph nodes showed complete distortion of the nodal architecture with replacement by nodular aggregates of necrotizing granuloma (Figure 3A and Figure 3B).
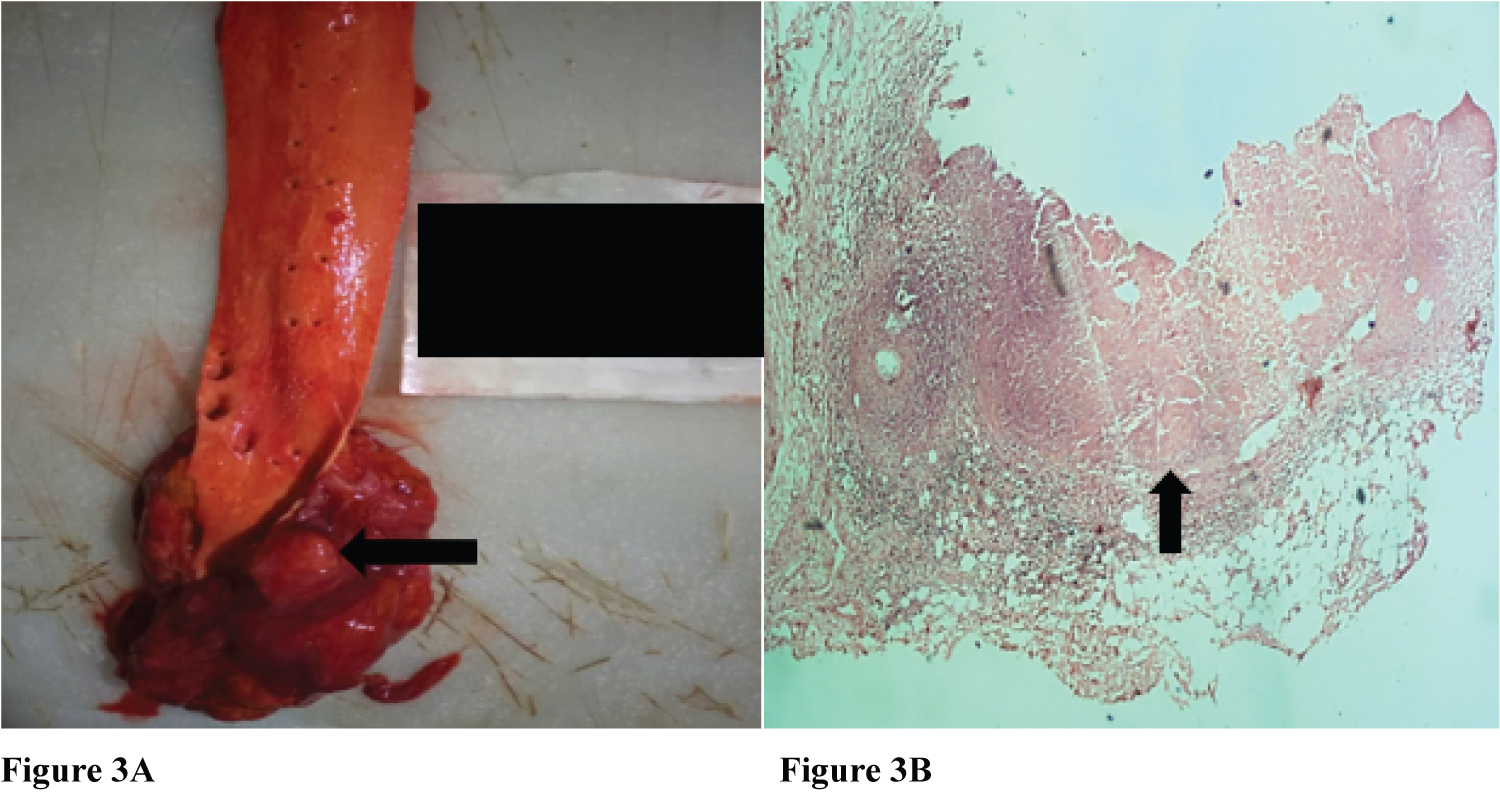 Figure 3: (A) (H&E x100)- Arrow: Enlarged para-aortic lymph node; (B) (H&E x100)- Arrow: Nodular aggregates of necrotizing granuloma.
View Figure 3
Figure 3: (A) (H&E x100)- Arrow: Enlarged para-aortic lymph node; (B) (H&E x100)- Arrow: Nodular aggregates of necrotizing granuloma.
View Figure 3
In addition, the right and left lungs were heavy and weighed 750 g (Normal: 280-500 g) and 775 g (Normal: 240-480 g) respectively. The cut surface of the left lung showed diffuse multiple tiny greyish white nodules with areas of oedema and congestion while examination of the right lung revealed congestion and oedema (Figure 4A and Figure 4B).
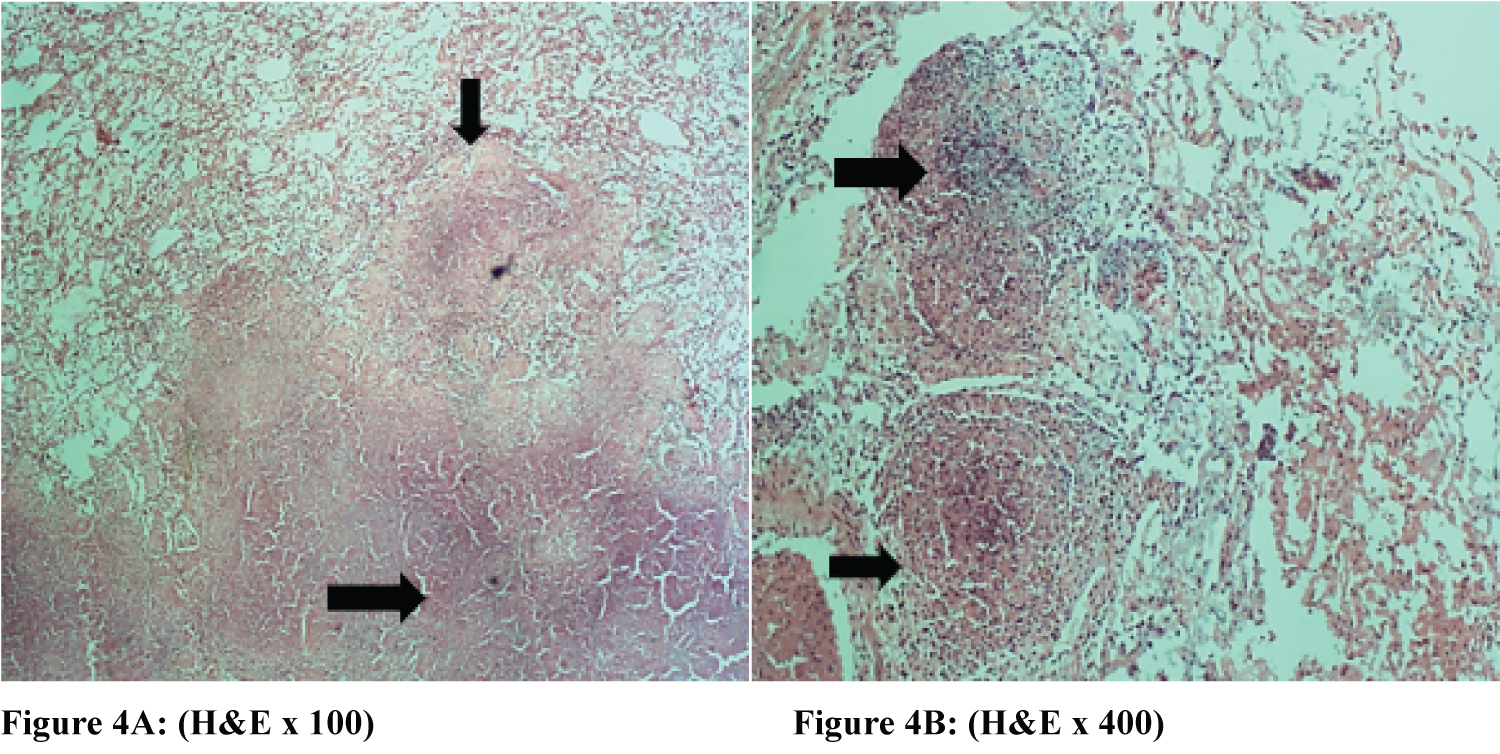 Figure 4: (A and B) (H&E x100)- Nodular aggregates of extensive necrotizing granulomas (arrows) and areas of mild interstitial and intra-alveolar spaces infiltration by inflammatory cells with intra-alveolar edema.
View Figure 4
Figure 4: (A and B) (H&E x100)- Nodular aggregates of extensive necrotizing granulomas (arrows) and areas of mild interstitial and intra-alveolar spaces infiltration by inflammatory cells with intra-alveolar edema.
View Figure 4
Disseminated TB is a chronic infectious condition in which there is dissemination of the Mycobacterium organism via haematogenous spread to 2 or more noncontiguous sites in the body [5,6]. The clinical presentation is sometimes nonspecific, and this could constitute a diagnostic quagmire. Disseminated TB is a known cause of fever of unknown origin [6,8-10], as also reflected in this patient who had history of fever for about 5 months. Symptoms and signs are variable and may relate to the organ systems affected [9]. Fever, anorexia, weight loss, anemia, hepatosplenomegaly, elevated ESR are some of the clinical manifestations of DTB. Other clinical findings like significant cough, haemoptysis, which could be found in PTB were absent in this patient similar to reports from other cases of DTB by Dalugama, et al. in Sri Lanka, Chandni, et al. in India, Alghamdi, et al. in Saudi Arabia, and Meira, et al. in Portugal [9-12]. DTB is not one of the known common causes of massive splenomegaly [13], which was an interesting finding in this patient. The presence of massive splenomegaly together with the haematologic picture of pancytopenia might have also promoted the consideration of haematologic malignancy like a lymphoma at the initial review of the patient. Haematologic findings in DTB include different types of anemia, leukemoid reaction, pancytopenia, disseminated intravascular coagulation [8-10]. A rare, life-threatening condition known as hemophagocytic syndrome could occur and this comprises anemia (100%), neutropenia (65%), thrombocytopenia (91%), pancytopenia (74%) with morphological evidence of macrophage phagocytosis of red cells, granulocyte and platelets [8].
Pancytopenia in the index case, similar to the case reported by Dalugama, et al. is an uncommon finding, that occurs in about 8% of cases and has been scarcely reported in cases of DTB in sub-Saharan Africa [8,14]. Explanations for pancytopenia in DTB include hypersplenism, histiocytic hyperplasia, maturation arrest, or infiltration of the bone marrow by caseating or noncaseating granulomas resulting in reversible or irreversible fibrosis [8-10].
Pegler-Huet anomaly (PHA), which is an abnormality of neutrophil, in this clinical context could be regarded as pseudo-Pegler-Huet anomaly (pseudo-PHA) that has been described in acquired conditions including tuberculosis [15]. A normal ESR, as found in our patient, is rarely seen in DTB unlike the findings in most other cases reported where ESR is typically elevated [5]. This seem to be unusual and contrary to reports by Dalugama, et al. and Alghamdi, et al. [9,11]. It has been mentioned that in most cases of fever of unknown origin, a relatively normal ESR may exclude a serious underlying disease [10], which was not the case with our patient as he eventually died within a week of hospital admission.
Chest X-ray was also normal in our patient similar to report by Dalugama, et al. and Chandni, et al. with about 10-15% of patients with DTB noted to have normal chest X-ray [5,9,10]. DTB with normal chest X-ray has been termed cryptic tuberculosis by some authors [5].
The pathognomonic tubercles described as chronic necrotizing granuloma with characteristic inflammatory type (langhan's and foreign body type) giant cells are usually seen at autopsy in organs of high blood flow like spleen, liver, lungs, kidneys and bone marrow [16]. In this index case, these lesions were noticed in the lungs, spleen, liver, pancreas, para-aortic lymph nodes, omentum and stomach wall.
It is important to note that most cases of DTB occur secondary to immunosuppressive conditions like HIV infection/AIDS, use of biologicals and immunosuppressive drugs for the treatment of medical conditions, increasing prevalence of organ transplantation, alcoholism, chronic liver disease, chronic hemodialysis, diabetes mellitus, malignancies, and silicosis [5-7,12]. There is possibility that our patient might have had an underlying liver disease, probably from the chronic alcohol ingestion, predisposing him to disseminated tuberculosis.
Disseminated tuberculosis is a life-threatening condition, with reported mortality of up to 30% [5]. Presentation could be atypical and DTB could present with normal ESR and chest radiograph with pancytopenia and massive splenomegaly in developing nations. Clinicians should therefore have a high index of suspicion so as to promptly diagnose the condition and offer appropriate treatment.
The authors hereby give the journal the consent to publish the article.
None.
Resident doctors and house physicians who were involved in the management of the patient during the hospital admission are hereby acknowledged.
Not applicable.
The manuscript has been read and approved for submission by the authors, who contributed equally. The requirements for authorship have been met and consent given to the journal for publication.