Objective: To determine the seroprevalence of antibodies to SARS-CoV-2 in asymptomatic individuals in a blood bank in southern Brazil.
Methods: 1015 serological analyses were performed between November 2020 and March 2021 in Joinville, Brazil, to detect IgG and IgM antibodies against SARS-CoV-2, and the results were correlated with the participants' age, gender, city and neighborhood.
Results: The seroprevalence of total antibodies was 40.4%, with reagent IgM detected in 9.4% of cases, IgG in 18.5% and both immunoglobulins in 12.5%. The presence of antibodies was higher, but without statistical significance, in males, corresponding to 40.9% of the samples, against 39.7% in females.
Conclusions: Our data suggests a high seroprevalence for SARS-CoV-2 in asymptomatic individuals in the analyzed period. In this context, it is important to highlight the epidemiological moment as a relevant variable. Nevertheless, controlling the spread of the virus remains a challenge when considering the large number of asymptomatic carriers.
COVID-19, Antibodies, Asymptomatic carrier states, Asymptomatic shedding virus, Blood banks, COVID-19 serological testing, SARS-CoV-2
The COVID-19 pandemic, which started at the end of 2019, had its first epicenter in the city of Wuhan, located in the province of Hubei in the People’s Republic of China. With rapid advancement, the virus has spread on a global scale, causing respiratory infections with a broad clinical spectrum, including the Acute Respiratory Distress Syndrome (ARDS) [1].
Taking into account the epidemiology of the new coronavirus, in June 2021 more than 175 million people had already been infected, leading to around 3,800,000 deaths globally [2]. In Brazil, the number of infected is over 17 million, and about 487,000 deaths [3]. In relation to Joinville, the largest city in the state of Santa Catarina and the place where the research was carried out, of the 597,658 inhabitants, more than 90,000 have already tested positive for COVID-19, and 1,485 died [4].
A study carried out by Oran, et al. at the beginning of the pandemic demonstrated that approximately 40%-45% of SARS-CoV-2 infections occur by asymptomatic individuals and they are able to remain infective for a prolonged period, possibly for more than 14 days [5]. Other research has already shown that viral shedding in asymptomatic patients can last for 19 days [6].
Therefore, due to the potential high risk of silent dissemination by individuals without symptoms, it is considered essential to carry out population screenings in order to understand the prevalence of asymptomatic individuals [5,6]. Consequently, patients without signs and symptoms of COVID-19 should undergo laboratory testing for public health and infection control purposes.
The indication of large-scale serological screening can be a strategy to define the number of asymptomatic infections, clarify the epidemiological situation, calculate the absolute risks of infection and predict the rate of viral spread [7,8]. In this context, it can be said that asymptomatic and pre-symptomatic infections contribute to herd immunity, and can boost up to 50% in the strength of infection at the peaks of an outbreak, making tracking of this population substantially important [9].
Thus, the use of easy-to-handle diagnostic methods helps to identify asymptomatic patients, becoming an alternative for epidemiological surveillance. Furthermore, serological assays are useful tools for identifying potentially immune individuals within the community. In this sense, rapid diagnostic tests for IgM and IgG, alone or in combination, can be useful for detecting exposure to SARS-CoV-2 [10].
The use of blood donors as a population for studies has been around for a long time and has proven to be advantageous in studies of subclinical conditions, incidence and natural course of infectious diseases; in addition, these studies can help to assess the dynamics of virus circulation and the evolution of COVID-19 in the studied population [11].
The main objective of this particular study was to examine the seroprevalence of antibodies to SARS-CoV-2 in asymptomatic individuals among blood donors at HEMOSC, the main blood donation center in Joinville and region (Santa Catarina, Brazil). This is the second study carried out in Brazil on the seroprevalence of asymptomatic individuals for COVID-19 among blood donors.
This is a cross-sectional observational, prospective study, carried out in Santa Catarina, in the municipality of Joinville, between November 9, 2020 and March 4, 2021. Rapid quantitative tests were performed to detect IgG and IgM antibodies against SARS-CoV-2 in order to identify the seroprevalence against COVID-19 in asymptomatic individuals.
The base population of the study were blood donors at the Regional Blood Center of Joinville, which is part of HEMOSC (Hematology and Hemotherapy Center of Santa Catarina). All research participants underwent screening established by HEMOSC for blood donation, meeting all eligibility criteria for donation established by the National Ministry of Health. Those who did not meet the criteria were not approached for participation in the study. In addition, individuals under 18 years of age, or with a known prior infection with COVID-19 or who had symptoms of infection with the virus or a known history of the disease were not included. Individuals who did not fit any of the exclusion criteria were then approached by the local HEMOSC team, in accordance with the prerogatives of Resolution 466/2012 of the National Health Council, and general guidelines on the research were carried out. If the person agreed to participate, the Free and Informed Consent Form was signed and an additional collection of whole blood was performed. In addition, the Blood Center was responsible for centrifuging the samples to obtain the serum and storing it at the appropriate temperature to later allow the researchers to carry out rapid tests for SARS-CoV-2.
During the research period, there were 6019 blood donations, and about 15 donors were randomly approached per day. Thus, a population of 1015 individuals was obtained to perform the serological analysis.
Serological analysis for SARS-CoV-2 was performed specifically at the Regional Blood Center in Joinville. The additional sample collected was 5 mL in a vacuum blood collection tube with separating gel and 5 mL clot activator (Vacutainer®, BD). The collection for the study was obtained in the same puncture of blood donation, not requiring a new approach to the individual.
The rapid tests against SARS-CoV-2 were funded by the Municipal Health Department of Joinville and, according to the manufacturer's package insert (Basall), have a sensitivity of 95.83% for immunoglobulin IgM, 91.67% for IgG and specificity of 100% for both. The following batches were used: 21320707, 21320703 21320704 and 21770701. The study researchers were responsible for carrying out the rapid tests on the samples, without the participation of HEMOSC.
The results of the analyzes were computed and analyzed using Microsoft Excel® software, including the participants' age, gender, city and neighborhood of residence. The level of significance used was set at 5% (p < 0.05). Such analyzes are presented through tables and graphs.
This study was registered under CAAE n° 3754260.7.0000.5366 in Plataforma Brasil and approved by the Research Ethics Committee (REC) of the University of the Region of Joinville (Opinion n° 4.277.404) in September 2020, as well as by the REC at the co-participating institution - Hematology and Hemotherapy Center of Santa Catarina (Approval No. 4,350,744) in October 2020.
During the study period, the seroprevalence of IgM and IgG antibodies to COVID-19 in 1015 blood donors was analyzed. The overall prevalence of antibodies was 40.4% in the participants, with reagent IgM being responsible for 9.4%, IgG 18.5% and both immunoglobulins detected in 12.5% of cases. Among the individuals analyzed, there was a predominance of males, and more than half of them (52.4%) were between 30 and 49 years of age (Table 1).
Table 1: Profile of participants and results of serological analysis. View Table 1
Among the participants, 889 (87.6%) of them were residents of Joinville, with the rest of the donors from other cities in the metropolitan region. The results were analyzed by region of residence in the city of Joinville, as shown in Figure 1. There was a predominance of samples reactive to any immunoglobulin in the southern region (43%), followed by the district of Pirabeiraba (42.8%). The regions with the least positive results for antibodies were the West (34%) and North Center (35.6%) regions. Regarding IgM, there were a greater number of reagents in the Southwest (14.3%). Analyzing the IgG, the highest positive result occurred in the Northeast region (25%). Meanwhile, the highest concomitant positivity of IgG and IgM immunoglobulins occurred in Pirabeiraba (14.3%).
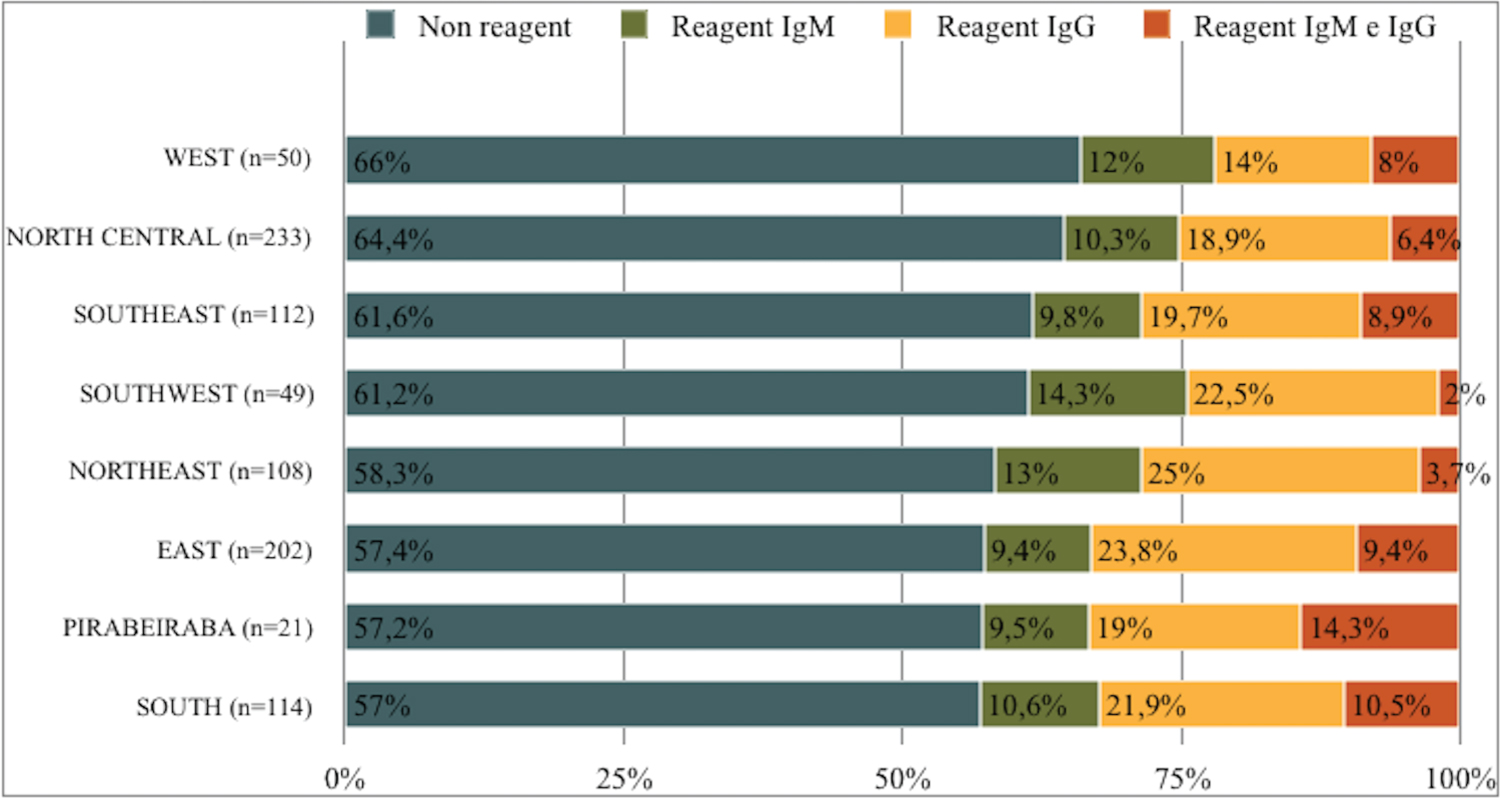 Figure 1: Analysis of seroprevalence by region of the municipality of Joinville.
View Figure 1
Figure 1: Analysis of seroprevalence by region of the municipality of Joinville.
View Figure 1
When analyzing the prevalence of antibodies among the residents of Joinville according to the months of collection, it is possible to observe, as shown in Figure 2, that November 2020 was the month with the highest number of reactive results (42.5%). On the other hand, January had the lowest prevalence (37%). Investigating by immunoglobulin, a peak of reactive IgM was found in November, constituting 12.8% of the samples. The IgG peak occurred in February (22.7%) and in December there was a peak of concomitant IgG and IgM immunoglobulins, representing a total of 18.2% of the individuals. The tests were performed until the 4th of March 2021. Therefore, the data collected in March was not included in the analyzes.
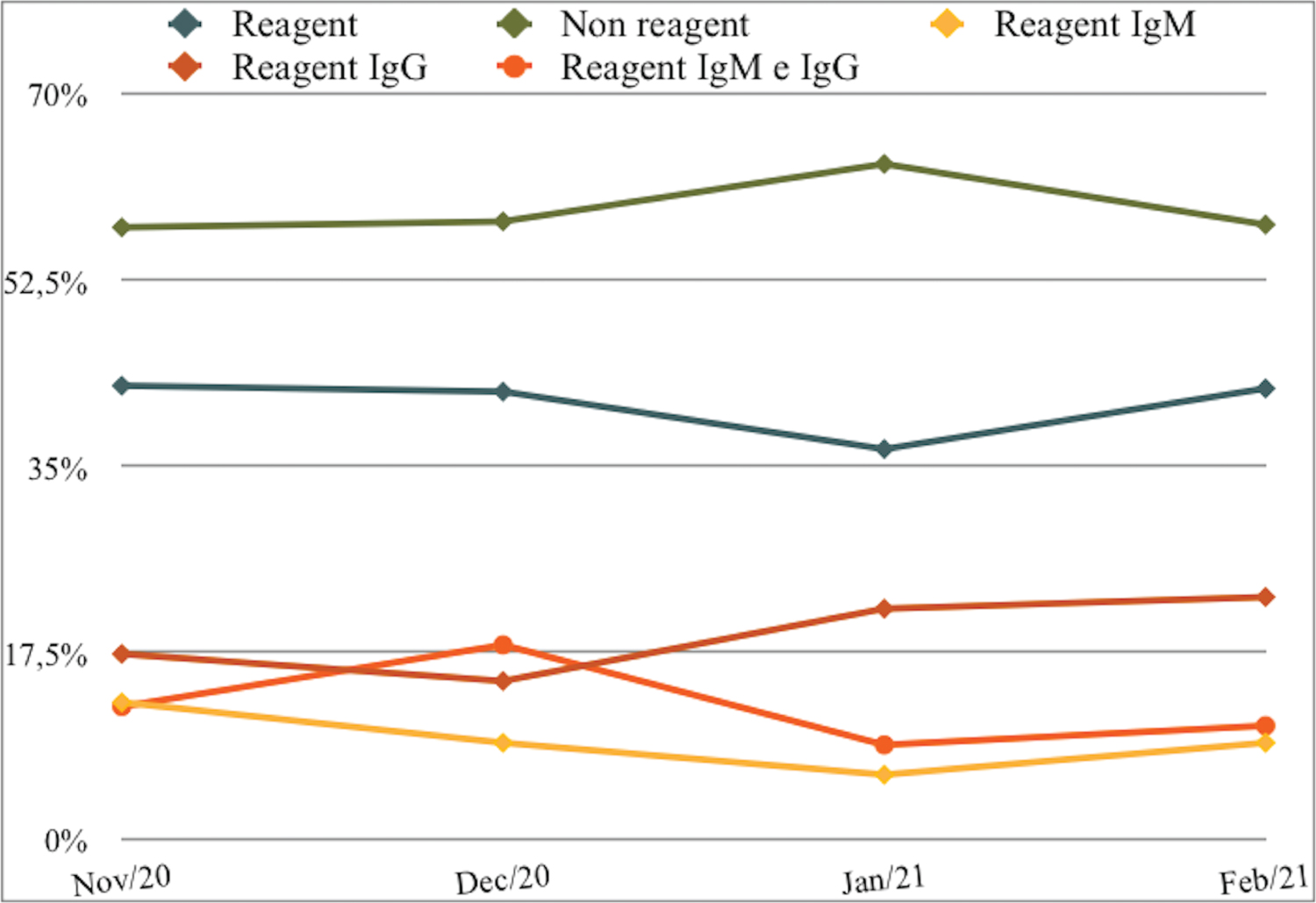 Figure 2: Monthly analysis of seroprevalence.
View Figure 2
Figure 2: Monthly analysis of seroprevalence.
View Figure 2
Regarding the test results according to age group, there was a decrease in the prevalence of antibodies with increasing age. The age range that showed a predominance of positive antibodies corresponded to individuals between 18 and 29 years (43.9%), followed by those between 30 and 49 years (39.2%) and, finally, a lower prevalence (34.2%) in donors between 50 and 69 years. However, when analyzing via binary logistic regression, it is possible to see that age did not represent a statistically relevant factor for the presence of antibodies. In the analysis for individuals aged 18 to 29 years, an OR = 0.992 (95%CI 0.93-1.05; p = 0.8) was seen; while for 30 to 49 years of OR = 0.978 (95%CI 0.94-1.009; p = 0.16) and OR = 0.941 (95%CI: 0.85-1.04; p = 0.23) for 50 to 69-years-old.
The presence of anti-SARS-CoV-2 antibodies was higher, but without statistical significance, in males, corresponding to 40.9% of the reagent samples, against 39.7% in females. Regarding the isolated positive results for immunoglobulin, men also had a higher prevalence of IgM (9.4% vs. 9.3%) and of IgM and IgG combined (3.6% vs. 11%). Regarding the isolated presence of reactive IgG, women had a greater number of positive samples (9.4% vs. 17.9%). When performing the binary logistic regression analysis regarding the gender of the participants and the presence of antibodies in the samples, it was noticed that the gender variable did not present a statistically relevant interference with the result, represented by an OR = 1.04 (95%CI 0 .81-1.35; p = 0.71).
The COVID-19 pandemic had great worldwide repercussions, which fostered the urgent need for further research on its transmissibility and infectivity. In this study, the seroprevalence of SARS-CoV-2 in asymptomatic individuals was identified in 40.4% of the tested individuals (95%CI 34.22%-48.43%), showing a high prevalence of infected individuals compared to other studies in different scenarios.
One of the pioneering studies looked at the prevalence of SARS-CoV-2 aboard the Diamond Princess cruise ship in Japan in March 2020 and found a proportion of 17.9% (95%CI 15.5-20.2%, n = 634) of asymptomatic cases tested using the qPCR method. However, due to the limitations of the study and the majority of passengers being 60 or more years-old, the data tend to be underestimated, not being used as a comparison parameter for population studies [12].
When comparing our prevalence results with other studies carried out in healthy blood donors, was found differences compared to data found in the literature. A study carried out in Milan between February and April 2020 (n = 789) found an increase from 2.7% to 5.2% at the expense of an increase in immunoglobulin IgG of 5% over the months of collection, derived from lateral flow immunoassay results. At the end of the research done in Milan, it was observed, that 2.4-9% of healthy adults had seroconversion (IgG + IgM) [11].
Another study carried out in Kenya in January 2021 with blood donors showed a total adjusted prevalence of 4.3% (95%CI 2.9-5.8%) using the ELISA method for SARS-CoV-2 IgG, with higher percentages in urban regions of the country [13]. Denmark had a study carried out with 9496 blood donors in April 2020 with a seroprevalence of 1.7% (95%CI 0.9-2.3) using the lateral flow test to identify immunoglobulins IgM and IgG [14]. The Netherlands, on the other hand, presented a seroprevalence of 2.7% according to the total antibody ELISA results for SARS-CoV-2 in a study carried out in April 2020, with significant regional variation, reaching up to 9.5% of immunoconversion [15].
In a cross-sectional Brazilian study carried out at the Blood Bank located in Rio de Janeiro, different results were obtained via rapid tests, compared to ours. The Hemorio study was carried out from April 14 to 27, 2020, with a population of 2857 blood donors, and presented a seroprevalence of 3.3% (95%CI 2.6-4.1). Furthermore, the respective individual seroprevalences were in disagreement with those identified in our study, with a predominance of isolated IgG, followed by both (IgM and IgG) and finally isolated IgM. In Hemorio there was a seroprevalence of isolated IgM of 23.7%, isolated IgG of 11.4% and both of 64.9%. Finally, contrary to our results, the study from Rio de Janeiro obtained statistical significance in individuals aged 18 to 29 years (OR = 1.86; 95%CI 1.12-3.08%) [16].
On the other hand, more recent studies have shown prevalence results that are congruent with our data. A Pakistani study carried out in December 2020 had a total of 380 healthy male blood donors who were tested by electrochemiluminescence immunoassay (ECLIA) for IgA, IgM and IgG antibodies, obtaining a final seroconversion of 37.7%, being 81% of the IgG type confirmed by the ELISA method [17]. In Jordan, 1374 blood donors were tested for total antibodies (IgA, IgM and IgG) by ECLIA against SARS-CoV-2, with a seroprevalence of 27.4% in February 2021 [8].
Regarding age groups and gender, our study is in agreement with the world literature, with no statistically relevant correlation with these variables. As observed in the study carried out in Jordan, blood donors did not present a statistically significant difference when analyzing the parameters of sex, age, residence and blood group. Men and women were equally affected (27.6% vs. 26.3%) [8]. Also in this context, the Dutch study showed a gender-independent seroprevalence in all age groups. Furthermore, congruent with our study, it was observed that antibodies were more prevalent in the population of young people between 18 and 30-years-old [15].
The Kenya study, in turn, analyzed a total of 3174 blood donors aged between 15 and 66 years, with a predominantly male population (82%). In this research, the gross seroprevalence did not vary by sex (P = 0.50), being higher in the younger age groups (15 to 44-years-old) and decreasing with age (45 to 64-years-old) [13]. Furthermore, it was also found in the Italian study that the most recent infections, positive for IgM, were more prevalent in the older population, while young people had higher seroconversion to IgG [11].
After comparing the prevalence of SARS-CoV-2 in asymptomatic people with what is reported in the literature, we emphasize that the epidemiological moment in which each study was carried out is a relevant variable. While studies carried out at the beginning of the pandemic have shown lower prevalence, other more recent ones have found higher prevalence due to the prolonged time of exposure to the virus. Furthermore, prevention and control measures were different in each country, which probably led to divergences in the viral prevalence in each region. Within the context of the period between the third quarter of 2020 and the first quarter of 2021, our study found itself, in a peak of increase in notified and confirmed cases of the disease in the city of Joinville, proportionally increasing the total number of positive tests.
Comparing our results with the proven cases of COVID-19, there is no agreement with the peaks of incidence according to the months. According to the notifications of individuals confirmed by the infection through the qPCR exam by the eSUS system, the maximum peak occurred in the month of December (2020) with a total of 11,478 individuals (31.11%) [4]. On the other hand, our study showed a peak in November (2020) that represented 42.5% of reagents, while eSUS showed 22.7% [4].
Our study has as its strength the analysis of 1015 individuals from the metropolitan regions and municipalities of Joinville that were randomly chosen to participate, culminating in seroprevalence data from blood donors in the region. In addition, we determined the prevalence of antibodies in asymptomatic individuals to assess the epidemiological profile of this population, a fact that contributes to the formation of preventive measures to control the pandemic.
To ensure safety in carrying out this study, the recommendations for implementing measures to avoid false positive and negative test results were followed. According to the manufacturer's instructions, the correct storage of blood samples and the contents of the analytical kit and its devices was carried out, in addition to proper handling of the material so that there was no cross contamination; non-reuse of materials used for testing; labeled the samples with the correct information and confirmed compatibility with the individual result and correct disposal of biological waste [18].
However, our study has some limitations. First, the representativeness obstacle, as blood donors differ from the general population in terms of viral exposure and the prerequisites of the blood donation ITSELF. In addition, many infected individuals are not included in our study as they were not part of the age group in focus (> 18 years to < 69 years), making it difficult to extrapolate according to age. Although socially heterogeneous, the population represents a preliminary view of asymptomatic individuals with antibodies to SARS-CoV-2.
Second, the interpretation of results is operator dependent and there was no confirmation through the qPCR method, which is considered the "gold standard". Additionally, the quick test performance may have been below that described by the manufacturer. According to a document published by the National Ministry of Health in 2020, no published studies were found that evaluated the tests in practice despite the tests having been approved by Anvisa, thus evidencing the possibility of a difference in performance to that described by the manufacturers [19]. In order to reduce bias, all sample results were individually interpreted and reviewed by three analyzers to ensure greater reliability in the acquired results.
Third, we did not obtain additional data from study participants, such as comorbidities, blood type, and viral exposure history. It is believed that these factors may partially explain the divergences in prevalence results as well as the distribution of cases according to months.
As a last limitation of the study, it is noteworthy that the start of vaccination in the city of Joinville occurred from January 19, 2021, onwards, that is, during the period of data collection for this research. In the first phase, vaccination took place in health professionals and individuals assisted by Long-Term Institutions for the Elderly (LTCIs). In a second moment, vaccination was started for individuals over 90 years of age and then progressing to those aged 85 years. These periods coincide with the research, however, due to the fact that our population is between 18-67 years-old, it will have had little impact on the data analysis.
Nevertheless, controlling the spread of the virus remains a challenge when considering the number of asymptomatic carriers. An American study looked at the spread of the SARS-CoV-2 virus in the first 6 months of the pandemic and found that there are almost 5 individuals with asymptomatic infection for every diagnosed case of COVID-19 [20]. In this context, the analysis of the number of asymptomatic and subclinical infections is favorable in obtaining information that delimit the significance of the prevalence of SARS-CoV-2 in the healthy population [21]. The viral load of symptomatic and asymptomatic patients is similar, a fact that suggests potential transmission from individuals who do not present symptoms of the disease, which corroborates the importance of social distance and correct use of masks [22].
Finally, our data suggests a high seroprevalence for SARS-CoV-2 in asymptomatic individuals, making them a potential source of risk for viral transmission. Hence, we see the need to understand the vulnerability of the local population to infection and implement specific strategies to fight the pandemic [16]. In conclusion, the main strategies for pandemic control must include the isolation of active cases, contact tracking and social distancing [10].
The Authors declare that there is no conflict of interest.
Research funded by the Municipal Health Department of Joinville.
All authors have seen and approved the content of the manuscript and have contributed significantly to the work.