Introduction Tuberculosis is ranked the second cause of mortality in the world only behind the deadly COVID-19. The disease is very communicable especially in poorly ventilated environments and crowded places. High risk of transmission from patients to health workers and then to the general population has been a great worry for the tuberculosis control programme worldwide. While great efforts has been made to improve case detection and improve treatment outcomes using DOTS most districts in Africa still fall below the expected target. This study explored factors affecting TB case detection in Kwahu East District of the Eastern Region of Ghana.
Methodology:A cross-sectional study involving 138 tuberculosis patients on treatment was used. A non-probability sampling method (i.e., convenient sampling technique) was employed to study the TB patients due to the availability of the participants at the various treatment centres. A structured questionnaire was used to interview participants and the results analyzed using SPSS version 20.0. Data was presented in tables and figures in the form of descriptive statistics.
Results: The result revealed that100 were males (72.46%) and 38 (27.54%) were females. The level of knowledge was above average (52.9%) among the TB patients. Majority of the TB patients reported to have suffered one form of stigmatization (weighted stigma score is 3.0). While the health facility remained the most reliable place for TB care most, TB cases reported they rather sought treatment from Prayer Camp (44.2%) as the number one choice. Reasons for choice of treatment place were distance (41.3%), cost (33.3%), belief of effective treatment outcome (10.1%) and shortage of medications (28.3%).
Conclusion: In conclusion, the study revealed that knowledge about TB was above average. However, factors such as stigmatization, poor accessibility and shortage of medications affect TB case detection in the district. Conscious efforts should therefore be made to improve access, regular supply of medications and reduce stigmatization in the community and health facilities.
Tuberculosis, Health facility, Case detection, Access, Stigmatization, DOTS, Factors contributing, Ghana
DOTS: Directly Observed Treatment Short course; TB: Tuberculosis; UER: Upper East Region; WHO: World Health Organization; BCG: Bacillus Calmette Guerin; KEDHD: Kwahu East District Health Directorate; KEDHMT: Kwahu East District Health Management Team; CI: Confidence Interval; MTB/RIF: Multi-drug Tuberculosis; LMICs: Lower- and Middle-Income Countries; HIV: Human Immune-Deficiency Virus;
Tuberculosis is the second leading cause of mortality in the world only behind COVID-19. The disease was the number one killer infectious disease before the insurgence of the COVID-19 pandemic [1]. Tuberculosis was responsible for over 1.5 million deaths globally in 2019 alone and new infections accounted for over 10 million worldwide [2]. The burden of tuberculosis has worsened due to disruption of TB activities during the insurgence of the COVID-19 pandemic [3]. Case detection has slowed down causing a major setback in the global effort to reducing TB incidence by 80% and mortality by 90% [1]. Tuberculosis (TB), which is caused by Mycobacterium tuberculosis complexes is a bacterial disease that mostly affects the lungs but can also affect other parts of the body [1]. Tuberculosis that affects the lungs is the most common form of tuberculosis and usually referred to as pulmonary tuberculosis. Tuberculosis affecting other parts of the body apart from the lungs is referred to as extra-pulmonary tuberculosis [2]. The main mode of transmission is usually from person-to-person through infectious aerosolized droplet nuclei generated by active coughing, sneezing, or spitting indiscriminately [3]. Globally, tuberculosis has been ranked alongside Human Immunodeficiency Virus (HIV) infection as responsible for high morbidity and mortality, with an estimated 9.6 million incidence cases and 1.5 million mortalities in 2014 [4]. Infectious diseases of such nature put excessive burden on health systems and fragile economies of both low and middle-income countries [5] of which Ghana is no exception.
Since the 1940s, effective treatment exist for the management of positive TB cases in addition to global transformation in social and economic development, but TB continues to be a devastating disease that affects the lives of millions of people especially in the African Sub-region [6]. The burden of tuberculosis is highest in Asia and Africa with about 25% of the global incidence reported in Africa alone. Evidence shows that while an estimated 10 million people were reported to have been infected with TB disease globally in the year 2019, just above average (71%) got reported to the health authorities. The remaining 29% missing cases were persons who were diagnosed with TB, yet could not be reported through the health system, private sector and undiagnosed cases [7].
It is estimated that about one-third of the human race are carriers of the tuberculosis bacilli but only few progresses to the disease stage due to precipitating host defence factors. An estimated three million cases of tuberculosis remained undiagnosed and have therefore not been treated in the African Sub-region [8]. A national survey conducted in Ghana in 2019 estimated the national prevalence of tuberculosis to be 290 per every 100,000 population which is over three-times the acceptable prevalence of 92 per 100,000 by the WHO [8]. Available data estimated the national prevalence of tuberculosis in the year 2020 through microscopy as 111 per 100,000 population and bacteriologically confirmed TB was 356 per 100,000 population [9].
Despite conscious efforts in Ghana and the enviable progress made in interrupting TB infection in Ghana, the disease remains a major public health challenge with over 46,000 incidence cases of active TB infection estimated to occur annually and killing about 7.5 per 1,000 infected individuals [10].
Even though Ghana has achieved above the global TB treatment success rate at 85%, case detection rate still remained low and shortfall of the internationally acceptable target for so many decades [11]. One might presume that low case detection translates to low prevalence of the disease, or a weakness of the surveillance system structures to detect and report cases. Epidemiological evidence available however, points to the fact that passive TB case finding remains inadequate to initiate early diagnosis especially in rural populations where the highest burden of TB outbreak could be detected [11].
While the national TB programme in Ghana remains very resilient in improving case detection and treatment outcomes huge disparities still exist in the programme. An estimated 3.7 million TB cases with about 1.6 million positive smear sputum positive TB are said not to be reported through the Direct Observed Treatment Strategy (DOTS) programmes [12].
While the focus for case detection in low- and middle-income countries (LMICs) has been through passive surveillance, a combined strategy of both passive and active case finding could improve case detection, especially in high-burden settings [13].
Anecdotal evidence suggests many people do not self-report to healthcare facilities because of fear of being stigmatised. Stigmatization against persons with tuberculosis and associated social discrimination does not compel people to volunteer and report to the health facility for diagnosis and treatment. Even among those diagnosed, adherence to treatment becomes difficult and many people end up defaulting. Poor adherence to treatment and defaulters consequently results in drug resistance and complicates the treatment choices available.
Until recently when Expert MTB/RIF was introduced with 105 GeneXpert machines installed across the country in Ghana, the mode of diagnosis of TB was through sputum smear microscopy and mostly done only by the government health facilities [14]. While this is an improvement, majority of the laboratories designated for TB diagnosis are secondary and tertiary level facilities with poor or no access to the rural communities where most cases reside. This implies that when a case is identified at a rural health centre the case would have to be referred to the nearest secondary or tertiary health facility for confirmation and initiation of treatment. In most cases the individuals fail to report for confirmation and find themselves back in the community interacting and transmitting the infection. This gap creates a major barrier for TB case detection, improved diagnosis and treatment of cases [14]. An estimated 3.7 million TB cases with 1.6 million with sputum smear positive were identified not to have been reported through the Direct Observed Treatment Strategy (DOTS) programmes in Ghana [15].
While many efforts have been made globally and in Ghana to increase TB case detection through improved diagnosis, expansion of diagnostic and treatment centres to improve access, provision of enablers packages to support feeding and transportation of TB patients coupled with the introduction of community DOT programme, TB case detection remain low in most districts in Ghana including the Kwahu East District of the Eastern Region. Current studies with evidence-based data on the causes of low TB case detection in the Kwahu East District to inform management of the health system to take concrete decisions to improve case detection are practically unavailable. With the current COVID-19 pandemic that further disrupted the health system and mimicking TB, people are afraid to report to the health facilities with cough for possible diagnosis of TB with the fear they may be diagnosed with COVID-19 and suffer the associated stigma. Consequently, cases of tuberculosis are increasingly undetected posing further risk to the population. This study could not have been conducted at any other time than now to provide evidence-based information on the causes of low TB case detection in the district.
In their article on "the stigma complex" Pescosolido and Martins eluded that contemporary research have identified common dimensions of public stigma even though studies most often do not employ extensively these dimensions. They further explained that not a single dimension of public stigma can be universally regarded as the most acceptable construct yet studies relies on one or two dimensions largely due to constraints on resources, time and burden on respondents [16]. The interplay of these dimensions outlined in Pescosolido, and Martins study are significant determinants of TB case detection and of great relevance in this current study. The conceptual framework in Figure 1 shows the influence of public stigma on TB case detection.
 Figure 1: Common dimensions of public stigma.
Figure 1: Common dimensions of public stigma.
Source: Pescosolido and Martin [16].
View Figure 1
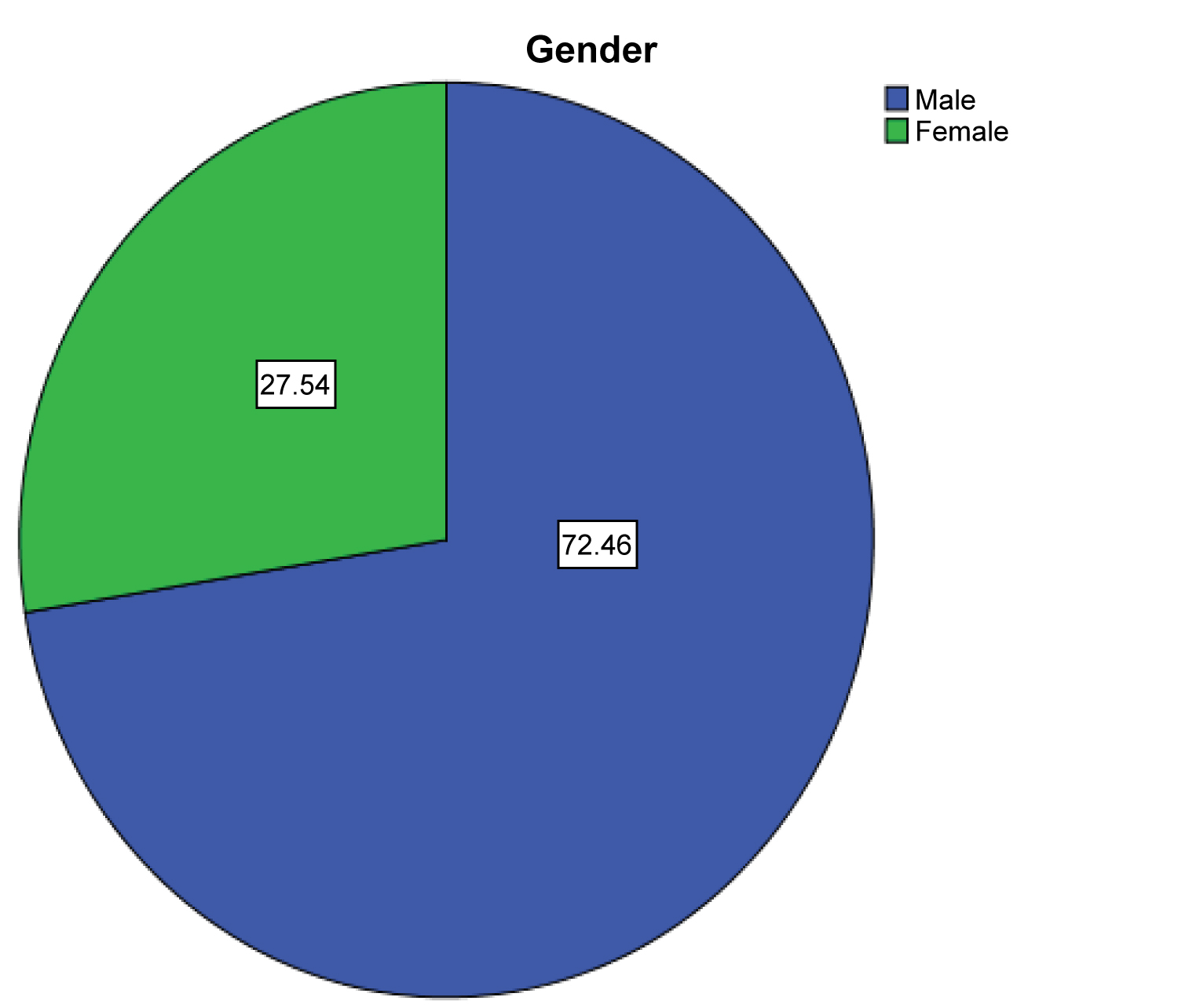 Figure 2: Gender of participants.
View Figure 2
Figure 2: Gender of participants.
View Figure 2
This was a descriptive cross-sectional study conducted among TB patients in the Kwahu Municipality of the Eastern Region of Ghana. A Non-interventional sampling technique was adapted due to the study targeting only TB cases on treatment in the area. The study made use of careful measurement of patterns of tuberculosis service usage and its outcome to draw inferences about factors affecting tuberculosis case detection.
The study was conducted in the Kwahu East District which was originally part of the Kwahu South District. Through a Legislative Instrument (L.I) 1839 the district was established and inaugurated on 29th February 2008 with Abetifi as the District capital. The district is situated on the northern part of the Eastern Region and shares boundaries with the Kwahu North to the east, Kwahu South to the south, Fanteakwa District to the southeast and Asante-Akim North of the Ashanti Region to the north. The district lies within three physiographic regions namely the Southern Voltarian Plateau, the Forest Dissected Plateau and the Savannah Plains consisting of a series of escarpments, notable among which is the Kwahu scarp rising from 220m to 640m above sea level [17].
The population of the district is heterogeneous with the predominant ethnic group as Akans (70.4%) of the total population. The other significant tribes include Ewes (17.7%) and Ga-Adangbe (5.0%). There are other minor ethnic groups with Northern origin alongside a number of Nomadic Fulani Herdsmen mostly from Mali and Niger [17].
Over 90% of the inhabitants are Christians of different denominations while the rest represent Islamic and traditional religions. Over 60% of the populations are literates and could read and understand information about TB.
The district currently is without a single hospital hence the habitants relies on 4 health centres, 2 clinics and 30 CHPS compounds for health services. All these health facilities can only provide basic primary health care services which warrant major cases to be referred to other districts with hospital facilities. In essence, access to TB diagnosis is limited in the district since only 5 facilities are currently designated for TB diagnosis. Even these designated health facilities can only conduct microscopy with limited personnel and other resources. In the nutshell, majority of the suspected cases might have to travel additional distances to access TB diagnosis. In most instances the suspects do not adhere to the referrals given to them and end up back into the community and eventually continue to spread TB among their families and peers. The poor access to diagnostic centres could translate to poor case detection and continuous spread of tuberculosis. This study was therefore relevant to provide evidence-based information on the factors that contributes to low TB case detection in the district and to provide basis for implementation of strategies to improve early case detection, early treatment and improve outcomes.
The study was carried out among adults who are currently on TB treatment during the years 2020 and 2021. Frontline health workers who are directly involved in the tuberculosis programme were also interviewed to establish administrative challenges that contribute to TB case detection. The study focused on Tuberculosis positive patients primarily because they are directly affected and health workers due to the indirect factors that affect case detection.
To determine the sample size for this study, the Cochran's formula for sample size determination was adapted.
Where Z = is the standard normal variant at 95% C.I. (1.96)
p = Expected proportion in population based on the prevalence of TB in the district (10%)
d = Absolute error or precision (5%).
Therefore, with z = 1.96 using confidence level of 95 %,), p = 0.9 (i.e. 90%) and d = 0.05 (i.e. 5%)
However, the study received 138 completed questionnaires representing a response rate of 92%
A non-probability sampling technique specifically convenient sampling technique was adopted in this study to select the participants for the study. Purposive sampling was employed to select the health facilities. This was due to the fact that TB diagnosis and treatment are done only in five of the 36 health facilities. Participants who visit the TB unit on daily basis for their review and treatment were conveniently enrolled after consent was sought. These techniques were relevant for this study due to the covet nature of the target population. Due to stigmatization and other social determinants associated with TB makes it difficult for TB patients to accept to be included in such studies. Convenient sampling ensures that any case of TB who was available and willing to participate in the study during the period of the study was included. As cases report for treatment and other related services they were first screened to ensure that they are registered by cross-checking the register before they were recruited into the study. New cases of TB who visited the treatment unit were also not recruited into the study. The study, however, did not include TB patients below age 18 years to avoid ethical violations.
A semi-structured questionnaire was used for data collection. The questionnaire was piloted to increase its reliability and validity by pretesting in a similar population in a different district among a sample of 10 patients. This ensured that all questions with ambiguities and other unpleasant responses were well constructed before the final study. Also, questions that did not provide objectivity in measuring the main research question were deleted. The data collection tool addressed variables on the demographic characteristics of the participants, knowledge, accessibility and stigmatization factors that affect TB case detection.
A semi-structured questionnaire was used for data collection. The questionnaire was piloted to increase its reliability and validity by pretesting in a similar population in a different district among a sample of 10 patients. This ensured that all questions with ambiguities and other unpleasant responses were well constructed before the final study. Also, questions that did not provide objectivity in measuring the main research question were deleted. The data collection tool addressed variables on the demographic characteristics of the participants, knowledge, accessibility and stigmatization factors that affect TB case detection.
The non-probability sampling technique of convenient sampling is the main limitation of the study. Convenient sampling weakness of not allowing equal opportunities for inclusion in a study creates a form of selection and interviewer biases. The fact that this study purposively studied TB patients and frontline health workers might have also introduced a selection bias.
The study anticipated total participants of 150. However, 138 participants responded to the questionnaire representing a response rate of 98.6%. Most of the cases were males, 100 (72.46%) and the rest 38 (27.54%) were females in the study (Figure 2). Majority of the participants were in the youthful age. About 26.8% were in the age category of 38-47 years, 21.0% 18-27 years while 3.6% were 28-37 years old. About 20.3% were above age 50 years (Table 1). Only 10% of the cases were less than 18 years. This implies that cases of TB were more prevalent among adults compared to children. This partly might be associated with BCG vaccination and the fact that adults seems to engage in more outdoor activities, involve in risk behaviours such as alcoholism and poor diet intake which predisposes them to development of active TB. While 73.2% of the TB cases had formal education, 26.8% had no formal education (Figure 3).
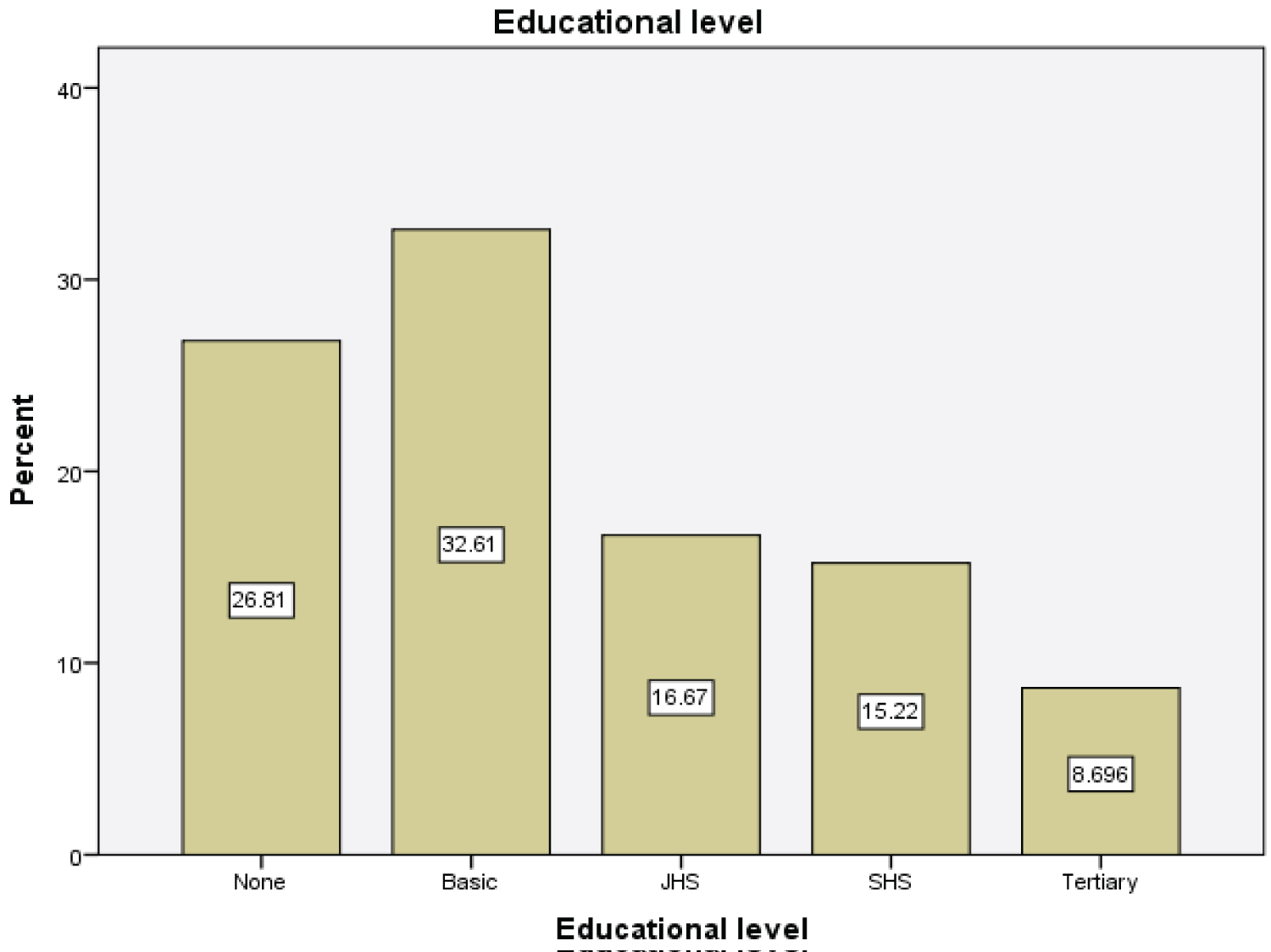 Figure 3: Participants educational status.
View Figure 3
Figure 3: Participants educational status.
View Figure 3
Table 1: Age distribution of respondents. (Source: Researcher's fieldwork, 2021). View Table 1
The study assessed the level of knowledge of participants on the following indicators; (1) what is TB? (2) Causes of TB (3) mode of transmission of TB and (4) symptoms associated with TB.
Knowledge regarding TB was found to be averagely good among the participants. A little above average (52.9%) knew TB was a disease (Table 2). Meanwhile, a good proportion (29.0%) did not have knowledge about tuberculosis. About 18.1% of the TB cases still belief that the disease is an ancestral curse. More than half of the participants were able to respond that TB was caused by a bacteria (n = 83, 60.1%). However, others mentioned ‘Curses' (n = 22, 15.95%), ‘Witchcraft' (n = 22, 15.9%) and ‘bad odour' (n = 7, 5.1%) as the main causes of TB infection (Table 2).
Table 2: Respondent's knowledge of tuberculosis. (Source: Researcher's fieldwork, 2021). View Table 2
While over 50% of the participants could correctly say TB infection is acquired through inhaling someone's cough and sneeze' contaminated with the TB bacteria (n = 74, 53.6%), other participants mentioned ‘sexual intercourse' (n = 37, 26.8%) and ‘sharing of sharp objects' (n = 27, 19.6%) as the main modes of TB transmission (Table 2). Even though participants could mention some of the signs and symptoms of TB, it was clear that they could mention not more than three signs or symptoms. Prominent among the signs and symptoms participants could recognize were ‘Weight loss' (n = 48, 34.8%), ‘Cough' (n = 47, 34.1%), ‘Night Sweat' (n = 17, 12.3%), and ‘Fever' (n = 14, 10.1%) (Table 2).
The study identified stigmatization as a major determinant of TB case detection. The result reveals that all participants suffer one or more forms of stigmatization in their daily lives as TB patients. The weighted stigma score measured in this study was 3.0 (Table 3). This is quite high and suggests the patients' agreement to being stigmatized in one or more forms. Meanwhile, participants do not feel being looked down upon by their family members who gave a weighted mean score of 2.4 (Table 3).
Table 3: Analysis of constructs of stigmatization among TB patients. View Table 3
Access to TB diagnostic centres is a very key indicator for early diagnosis and prompt treatment. The study explored the available facilities for TB diagnosis and treatment among the participants. While the District has 5 designated diagnostic and treatment centres, majority (44.2%) of the participants prefers to visit the prayer camps for their healing when they are diagnosed with TB (Figure 4). Other preferred treatment choices mentioned were traditional healers (23.9%) and licenced chemical stores (13.0%). Only 18.8% of the participants indicated their readiness to visit the health facility for treatment when they test positive (Figure 4). Various reasons were cited for the choice of treatment centres. Participants choice of treatment as established in the study were; easily accessible (n = 57, 41.3%), less costly (n = 46, 33.3%), healing is fast (n = 21, 15.2%) and Effective treatment (n = 14, 10.1%) (Table 4). This suggests that the available health facilities designated for TB diagnosis and treatment are not accessible to the population and hence they found alternatives for treatment. This could result in missed cases, treatment failure, drug resistant and other associated complications.
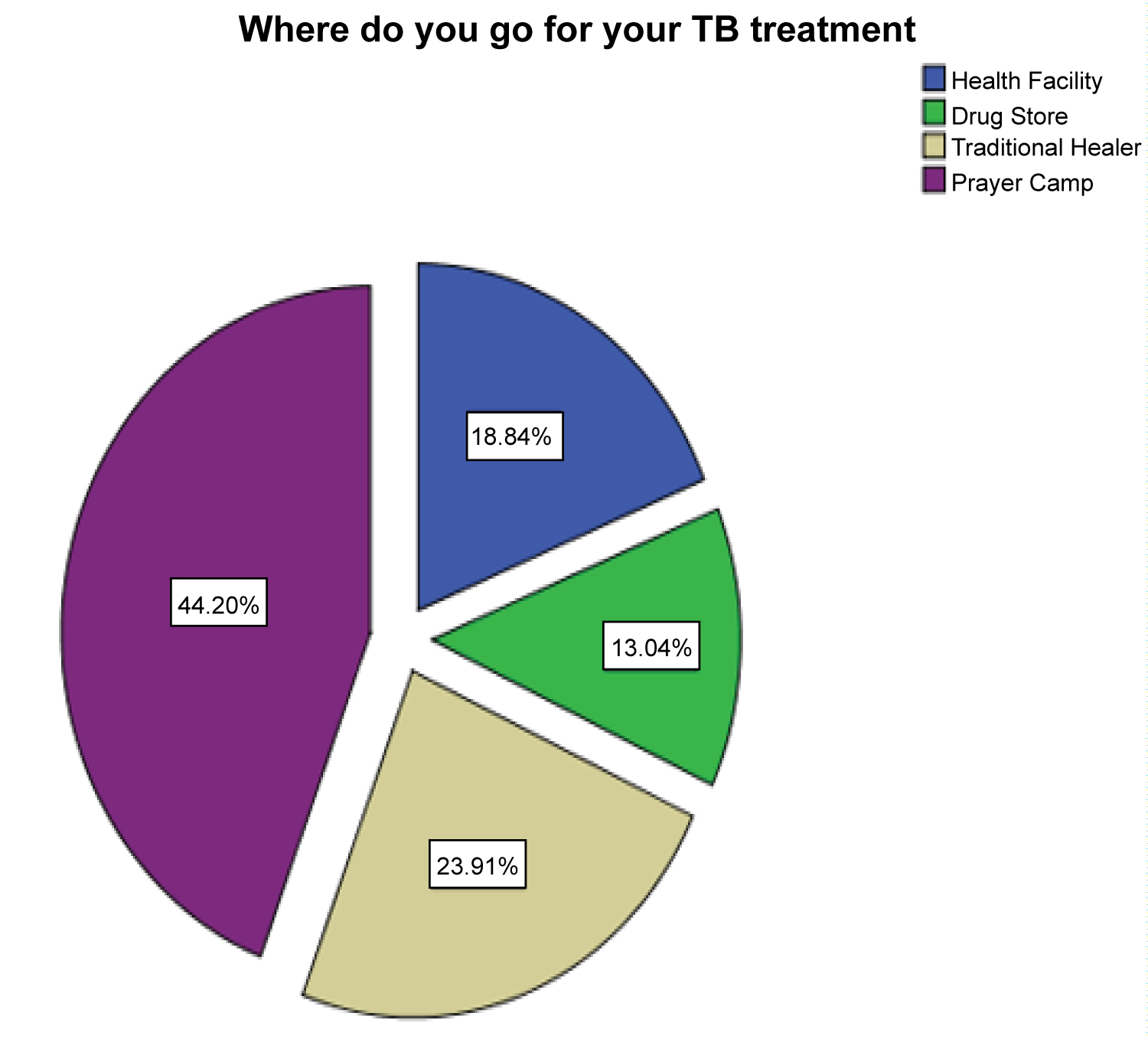 Figure 4: Respondents choice of treatment place.
Figure 4: Respondents choice of treatment place.
(Source: Researcher's fieldwork, 2021)
View Figure 4
Table 4: Factors affecting accessibility of tuberculosis services/facilities. (Source: Researcher's fieldwork, 2021). View Table 4
The nearest treatment centre according to the study was 1 km (n = 41, 29.7%). Other participants indicated that they travel more than 2 km (n = 55, 39.9%) while some travel about 2 km (n = 42, 30.4%). Distance has been cited in many studies as a major barrier for TB case detection and treatment (Table 4).
The study also revealed that access to medication at the designated treatment centres is a major challenge. More than half of the respondents agreed and strongly agreed to the statement ‘lack of medication during TB treatment'. As presented in (Table 4) about 39 (28.3%) each agreed and strongly agreed to the fact that they do not get the required medication during their visit. Again, fifty percent of participants cited long waiting time for more than 1 hour as a barrier for TB treatment. The amount of time spent during medical consultation is a very important factor in either motivating or demotivating a sick person for seeking appropriate medical care. However, another 50% cited that the time spent during consultation and treatment was less than 1 hour. The result in Table 4 further revealed that about 59 (42.8%) and 44 (31.9%) ‘strongly disagreed' and ‘disagreed' respectively that they were visited at home during their sickness. High cost of transportation and poor access to health facilities were other factors cited that affects TB case detection.
Failure of the health system and other community structures to detect cases of tuberculosis remained a fundamental challenge in interrupting community transmission, ensuring early treatment and improving outcome of tuberculosis disease. The target to ensure communities are free of tuberculosis is highly dependent on the ability of the health system to detect and report cases early for diagnosis and early treatment. Low tuberculosis case detection is a major consequence that the health system and other stakeholders must address to achieve the goals of the global tuberculosis control programme. Low case detection has been consistently observed in the Kwahu East District for the last three years. The District recorded 13.8, 10.4 and 18.4 per 100,000 population for the years 2019, 2020 and 2021 compared to an estimated 282/100,000 target by the WHO per district. Appropriate screening mechanism is required to improve case detection and interrupt community transmission. This health facility-based study was thus conducted to determine factors accounting for the consistently low TB case detection rate in the district by providing evidence-based data for decision making to improve the case detection rate.
Majority of the study participants were adults ranging between 38-47 years. The average age of the participants was about 40years. Only few of the cases studied were less than 18 years. Similar findings were reported in a community based study conducted in the Volta Region of Ghana where most of the TB cases were found among persons over 30 years with an average age of 43 years [18,19]. This finding could suggest the high risk population for tuberculosis in the district and appropriate group for targeted screening for presumptive cases. Men were found to be more affected than women. This finding conforms to findings a cross-sectional study in the Gambia on delays in TB diagnosis were they reported over 70% of the cases to be men [13]. Other studies conducted in Africa [16,17,19] also identified men as a high risk group for TB infection than women. Men are found to be mostly involved in outdoor activities compared to women and might account for what was observed in this study. Women usually are confined to their homes taking care of household chores and children thereby reducing their risks of exposure to the causative organism Mycobacterium tuberculosis which is known to be transmitted through the air. While education plays a major role in disease prevention this study found over a quarter of the cases not to have had formal education. Only few cases were recorded among persons who had formal education. This suggest that education is a positive determinant of TB infection since educated people have access to information regarding TB through various media compared to the uneducated.
Knowledge about tuberculosis empowers people to take steps to prevent infection and appropriately access diagnosis and treatment early to prevent complications and transmission to others. High knowledge about tuberculosis should under normal circumstances translate into early reporting, diagnosis and treatment. The study found knowledge about tuberculosis to be above average. Similar studies [20,21] also reported high knowledge of tuberculosis among the study participants. Over fifty percent of the participants could accurately identify TB infection as a disease caused by a bacterium. It was further established that most of those who had knowledge about tuberculosis only had knowledge after they had the infection. This means that prior knowledge of tuberculosis before infection could be low on the sampled community. The main source of knowledge was from health workers. Most participants had accurate information about TB from the health facilities when they either go for screening, diagnosis or started the treatment. Other sources according to the study were media and friends.
While more than half of the participants understood the cause of tuberculosis, more than a quarter of the participants had poor knowledge. Some participants associated TB infection to ancestral curses, witchcraft and bad odour [20]. The poor knowledge as established is a major challenge that health professionals must take immediate steps to address. Poor knowledge implies that community transmission might be difficult to interrupt and suggest that many people are infected but have not reported for screening and possible treatment when positive.
While majority of the participants were aware of the mode of transmission of the TB bacilli few other still belief that TB could be transmitted through sex and sharing of sharp objects. While this findings agrees with the finding of [22,23] it also disagrees with the outcome of what [24] found out in a study that showed that respondents have poor knowledge regarding tuberculosis infection.
Stigmatization of any form is a major barrier that affects people from volunteering to have a TB test or diagnosis. According to Mitchell et al., people may stigmatize against people with TB due to its relative deviance from that which is acceptable to be normal. The norms governing what is considered acceptable or unacceptable are socially constructed and expressed not only by individuals and thus TB stigma may be experienced in multiple ways both at the individual and community level [25]. The consequences of stigmatization affect early detection, early diagnosis and treatment adherence. Most TB patients default because of fear of stigmatization from the community, health authority and peers. This study found similar outcome as majority with weighted stigma score of 3.0 (range 0-4) of the participants reported to have witnessed one form of stigmatization during the period they were diagnosed. Similarly, other studies in Africa [23,26], found that TB patients are stigmatized against in their community and peers. Reported forms of stigmatization includes friends and neighbours looking down upon TB patients; friends or neighbours looking down on TB patients' family; and friends or neighbours avoiding TB patients on purpose [26-28]. The high level of stigmatization in the community could affect case detection as people would not report for testing or default treatment. When people don't come for diagnosis even when they have signs/symptoms or default in treatment transmission would continue in the community. But the health system is unable to detect these cases because of poor access to diagnostic centres, poor availability of logistics and sometimes shortage of medications.
The study however found that stigmatization within the families of TB cases was not happening. This finding is contrary to what was found in the study by [26]. Social support from the immediate family was good and a source of motivation for cases to continue treatment. Family is an important social system that offers various forms of support to its members especially in African societies. To ignore and abandon a member of a family because of illness is highly frowned upon.
Access to appropriate facility for TB diagnosis, treatment and care is an important factor that ensures the right diagnosis and treatment for tuberculosis patients. Many people seem to explore various sources for TB treatment when they are sick due to poor access to a health facility. Most of the participants in this study indicated their most preferred place for treatment was a Prayer Camp. Only a few indicated their choice of place for treatment to be a health facility. Reasons cited in this study for the choice of treatment place were poor access to health facilities, cost of traveling to health facility [29,30] and the belief that healing is faster and effective when they visit a prayer camp, traditional healer or spiritualist. This is an indication of missed cases through these other sources than the health facilities. While health facilities remained the best and reliable places for treatment of TB, most of the respondents prefer other options to have treatment for TB largely due to poor access. Distance was found to account for participants' inability to visit health facilities for treatment and therefor resorting to prayer camps and others [25,31]. While few participants indicated they travelled less than 2 km to the nearest health facility, majority of the participants travelled over 3km to access health care including tuberculosis care. These findings are supported by the results obtained from another research conducted in Upper East Region (UER) of Ghana which indicated that majority (62%) of the population resident in the UER were located more than 10 km away from a health facility providing TB testing services [32,33]. The mean distance ± standard deviation to the nearest public health facility providing TB testing services in UER was 33.2 km ± 13.5 [32].
The study also revealed poor access to medications as a major barrier affecting case detection. A good proportion of cases reported that they could not get all the medications required when they visited the health facility for treatment. The shortage of medication affected subsequent visits and the decision to resort to other options to have treatment. This finding was also reported in a study by [25] where patients were cited to express their disappointment for lack of medication during visit to the treatment centre. One of the pillars of the DOTS strategy emphasized the need for adequate supply of quality medications to prevent interruption of treatment. The lack of medication reported in this study therefore violates that component of the strategy and all efforts must be made to ensure sustainable supply of medication to avoid interruption of treatment which could result in relapse of cases and subsequent development of drug resistant TB. The DOTS strategy also emphasized quality diagnostic equipment by microscopy and new methods that would identify over time to avoid false negative diagnosis. However, out of the 40 health facilities in the district, only 5 of them are diagnostic centres. The limited diagnostic centres and pressure on the few health personnel, equipment and logistics could affect the quality of diagnosis leading to missed cases. Due to the cost of traveling to receive treatment, shortage of medications would mean some patients would not return in subsequent visit. This study sustained the results established by [34] which identified that all components that go into management of TB including quality smear microscopy and adequate supply of medication should be enforced at all times. The lack of any of the components of the DOTS strategy could leads to poor case detection and high attrition rate.
Other barriers identified by this study were long waiting time and lack of home visit to follow up on TB cases. The average time spent was about 1 hour at the health facility. Some reported to have spent longer than an hour to see the doctor and that discouraged them from visiting the health facility. In the study it was seen that respondents who lost time in repeat visits to health providers also lost cost in various ways, such as through opportunity costs including lost earnings, neglected household responsibilities and lost productivity [35]. In the likert questionnaire about half of the respondents strongly agreed and agreed to have spent more than sixty minutes. Similar findings were identified in another study [36].
The level of knowledge of TB patients was above average. Factors affecting case detection identified in this study were high level of stigmatization, poor access to TB diagnostic centres, high cost of transportation, periodic shortage of medications and long waiting time for consultation, diagnosis and treatment. A good proportion of TB cases seem to be missed through prayer camps and traditional healers due to these challenges enumerated in the findings. A collaborative effort between the various stakeholders including traditional healers, spiritual healers, chemical sellers and the Ghana Health Service would be important in ensuring effective referrals for effective diagnosis and treatment of TB cases. This would ensure cases that might visit either of these places than the health facilities are linked to the health facilities for appropriate diagnosis and treatment. Case detection can then be more enhanced to avoid missed cases and improve notification and detection.
The study received approval from the Kwahu East Municipal Health Directorate for access and use of information from their TB records for the study. All participants were informed about the benefits and risk associated with the study. Subsequently, participants were informed about the fact that participation is voluntary and participants deserve the right to pull out of study at any point without any penalty. To ensure anonymity of participants, identification numbers were used instead of names. This method of anonymity ensures that participants are not identified through their responses to the questionnaire or otherwise. The study did not involve collecting medical information of the respondents and concentrated on only TB and thus any other medical condition of the patients while on treatment was not considered.
The authors have no conflict of interest regarding any aspect of the study.
No funding received from any source apart from the researchers' personal contributions.
We are grateful to the study participants who volunteered to participate in the study. We are also grateful to the Kwahu East District Health Management Team for their support, cooperation and approval of this study by providing relevant information throughout the study period.
The contributions of the authors are as follows: conceptualization, MK, HSD, KL, KOF and AM.; methodology, MK, HSD, KL, KOF and AM; formal analysis, MK, HSD, KL, KOF and AM; writing-original draft preparation, MK, AA and PKA; writing-review and editing, MK, AA and PKA; supervision of study, MK. All authors have read and approved the manuscript.