Background: Various diagnostic tests across COVID-19 literatures were employed as surrogate markers in COVID-19, wherein interleukin-6 (IL-6) - gauge for cytokine storm or impending severity - is not readily available.
Objectives: This study determined the clinical value of inflammatory markers and hematologic indices as warning indicators in the prediction of severity of COVID-19 infection. Cut-off values were also determined.
Methods: Demographics, baseline inflammatory markers and hematologic indices were retrieved from the database covering April-December 2020 as a single-center retrospective cohort. Univariate, Multivariate, and Receiver Operator Characteristic analyses were done.
Results: There were 1,368 patients: 845 nonsevere cases (61.77%) and 523 severe cases (38.23%). Diabetes, hypertension, leukemia, cancer, cardiovascular disease, chronic lung disease, liver disease and chronic kidney disease are seen more in severe group. HIV did not establish significant difference between two groups. Markers C-reactive protein (CRP), lactate dehydrogenase (LDH), ferritin &procalcitonin; and indices neutrophil-to-lymphocyte ratio (NLR), fibrinogen, & D-dimer are significantly higher in severe group. Diabetes (OR 2.19, 95% CI 1.01-4.76 p < 0.05) and cancer (OR 4.58, 95% CI 1.24-4.76 p < 0.05) emerged as potent independent risk factors for COVID severity. CRP (OR 1.24, 95% CI 1.12-1.37 p < 0.05), LDH (OR 1.02, 95% CI 1.001-1.004 p < 0.05), and ferritin (OR 1.004, 0.998-1.009 p < 0.05) show the highest predictive value in developing severe COVID-19. Optimal cut-off values predictive of severity were determined more than 1.85 mg/dL for CRP (79% Sensitivity, 84% Specificity), more than 644.85 U/L for LDH (78.7% Sensitivity, 81.6% Specificity), and more than 621.4 ng/mL for ferritin (71.3% Sensitivity, 74.8% Specificity).
Conclusions: Nonsevere cases with diabetes, cancer, and high levels of CRP (> 1.85 mg/dL), LDH (> 644.85 U/L), and ferritin (> 621.4 ng/mL) have high predilection to become severe or O2-requiring in the course of infection. Utmost caution and monitoring at the onset are warranted.
Severe COVID-19, Inflammatory markers, Hematologic indices, CRP, LDH, Ferritin
COVID-19, caused by a novel single-stranded ribonucleic acid (RNA) beta-coronavirus, also known as SARS-CoV-2, is still a huge threat [1]. Predicting the severity is cumbersome due to the virus’ insidious characteristics. Cases have shown a wide array of presentation from asymptomatic to moderate presentation like pneumonia, and to critical events like thromboembolism, encephalopathy, cardiac manifestation, organ failure, acute respiratory distress syndrome (ARDS), and even death [2,3]. Burgeoning problems such as resource allocation and the gradual exhaustion of the health workforce become now more and more apparent. Thus, projecting the disease progression toward severe/critical is crucial for clinicians [4]. Presently, there is no current standard treatment of the disease. The management is mainly on the prevention of progression to severe/critical and its complications. The widely used gauge that is known to have the potential in predicting severity are laboratory markers. Levels of the serum markers have been employed - the inflammatory markers (serum C-reactive protein, ferritin, lactate dehydrogenase, and procalcitonin) together with the peripheral hematologic indices (leukocyte count, neutrophil-to-lymphocyte ratio, fibrinogen, and D-dimer) - in the projection of COVID severity [5-8].
The stratification of COVID-19 cases into severe (non-O2 requiring) and severe cases (O2 requiring) has been engaged by numerous studies in the association and determination of reliable laboratory markers in predicting severity. Several markers and hematological indices have been extensively studied [4,8-11].
Accumulating evidence suggests that inflammatory markers play a fundamental role in the severity and progression of the disease. However, the cut-off in predicting severity varies in different locales [12,13] and the overall inflammatory profile has not been established for COVID-confirmed patients, particularly in the Philippines.
The study employed a retrospective cohort from April 2020 to December 2020 with the databases: Southern Philippines Medical Center (SPMC) COVID-19 Severity Census, and SPMC Segworks Hospital Information System (SegHIS), accessible worldwide at https://his.spmcdvo.net/hisdmc/. Inclusion Criteria were adult patients (aged ≥ 19 years old) and are COVID-confirmed via Real-Time Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) of oropharyngeal and/oronasopharyngeal swab. A baseline workup was obtained, and nonsevere & severe status were determined at the onset of admission based on O2 necessity. The equipment was at par with International Standards: UniCelDxI 600 Access Immunoassay System (for CRP and LDH), UniCelDxC 800 Chemistry Analyzer (for procalcitonin and ferritin); and Hematologic indices: Stago STA Compact Max Coagulation Analyzer (for fibrinogen and d-dimer) & Sysmex XN-1000 Hematology Analyzer (for leukocyte, neutrophil, and lymphocytes). Biorad CFX 96 Real-Time RTPCR was used for COVID-19 detection.
Data were analyzed using SPSS version 26. Mann-Whitney U Test was used for gathered continuous data with non-normal distribution, and Pearson Chi-Square for the Categorical Data in determining the significant difference. Binary Logistic Regression Analyses were utilized to determine potential predictors for COVID-19 Severity. Receiver Operating Characteristics (ROC) was employed through Area-Under-ROC-Curve (AUROC) and Optimum Cut-off Value, to determine the predictive capability with sensitivity and specificity of the predictor(s).The higher the AUROC, the better the model in distinguishing patients as Nonsevere as truly Nonsevere (Non-O2-Requiring), and Severe group as truly Severe (O2-Requiring). Excellent Model has an AUROC of 0.8 and above by Hosmer-Lemeshow. Optimal cut-off values via Youden’s index for nonsevere were determined. Beyond that point, it carries the risk of severe.
Out of 1,368 cases, 845 (61.77%) were classified nonsevere while 523 (38.23%) for severe. Table 1 shows the demographic profile of the patients. Severe cases are significantly older as compared to nonsevere (median age of 40.29 versus 56.86, P < 0.01). There is significantly greater number of females (50.4% vs. 43.7%, P = 0.015) for nonsevere; and significantly more cases of males in severe group (56.59% vs. 49.5%, P = 0.018). Diabetes is relatively higher among severe 34.41% vs. 9.3% (P < 0.001). The same observations are seen with hypertension, cardiovascular disease, chronic lung disease, chronic kidney disease, liver disease, leukemia, and cancer. No statistical difference was seen for HIV cases (p = 0.439).Baseline inflammatory markers and hematologic indices between two groups with their corresponding significant differences are detailed in Table 2. All severe cases have significantly higher values in inflammatory markers and hematologic indices, except for leukocyte count.
Table 1: Demographic profile of patients with non-severe and severe COVID-19. View Table 1
Table 2: Baseline inflammatory markers and hematologic indices of patients with non-severe and severe COVID-19. View Table 2
Table 3 shows that all variables are found to be significant predictors of severity except for liver disease, HIV, and leukemia. In Multivariate analysis, as shown in Table 4, diabetes and cancer were demonstrated as strong independent risk factors for developing severe COVID with odds ratios of 2.19 [95% CI: 1.127-3.015 p < 0.05) and 4.58 [95% CI: 1.24-16.95 p < 0.05), respectively. High level of serum CRP, ferritin, LDH are independent risk factors for severe COVID-19 with odds ratios of 1.24 (95% CI: 1.12-1.37 p < 0.05), 1.02 (95% CI: 1.001-1.004 p < 0.05), and 1.004 (95% CI: 0998-1.009 p < 0.05), respectively. Procalcitonin did not establish risk (OR = 1) as compared with the aforementioned.
Table 3: Univariate Logistic Regression Analysis of variables. View Table 3
Table 4: Multivariate Logistic Regression Analysis of variables. View Table 4
ROC statistics shown in Figure 1 was run through diagnostics independently. The higher the AUROC, the better the diagnostic in distinguishing severe vs nonsevere. By standard, an excellent model has an AUROC of 0.8 and above. Among the potential predictors, only CRP, LDH, and Ferritin have excellent AUROC values with 0.855, 0.804, and 0.857 respectively as shown in Table 5. Optimal Cut-off for CRP levels for Nonsevere is 1.85 mg/dL as shown in Table 6; beyond that point is predictive for COVID Severity (CRP > 1.85 mg/dL) with 79% Sensitivity and 84% Specificity and 1.24x more likely to become severe (Multivariate OR 1.24; 95% CI 1.22-1.37 p < 0.05 - Table 4). A value greater than 644.85U/L for LDH is also a predictor of COVID severity with 78.7% Sensitivity and 81.60% Specificity and 1.004x more likely to become severe (OR 1.004; 95% CI 0.998-1.009 p < 0.05). For Ferritin, serum levels greater than 621.4 ng/mL are also predictive of severity with 71.3% Sensitivity and 74.8% Specificity, and 1.02x more likely to become severe as compared to the cut-off serum levels and below (OR 1.02; 95% CI 1.005-1.038 p < 0.05)
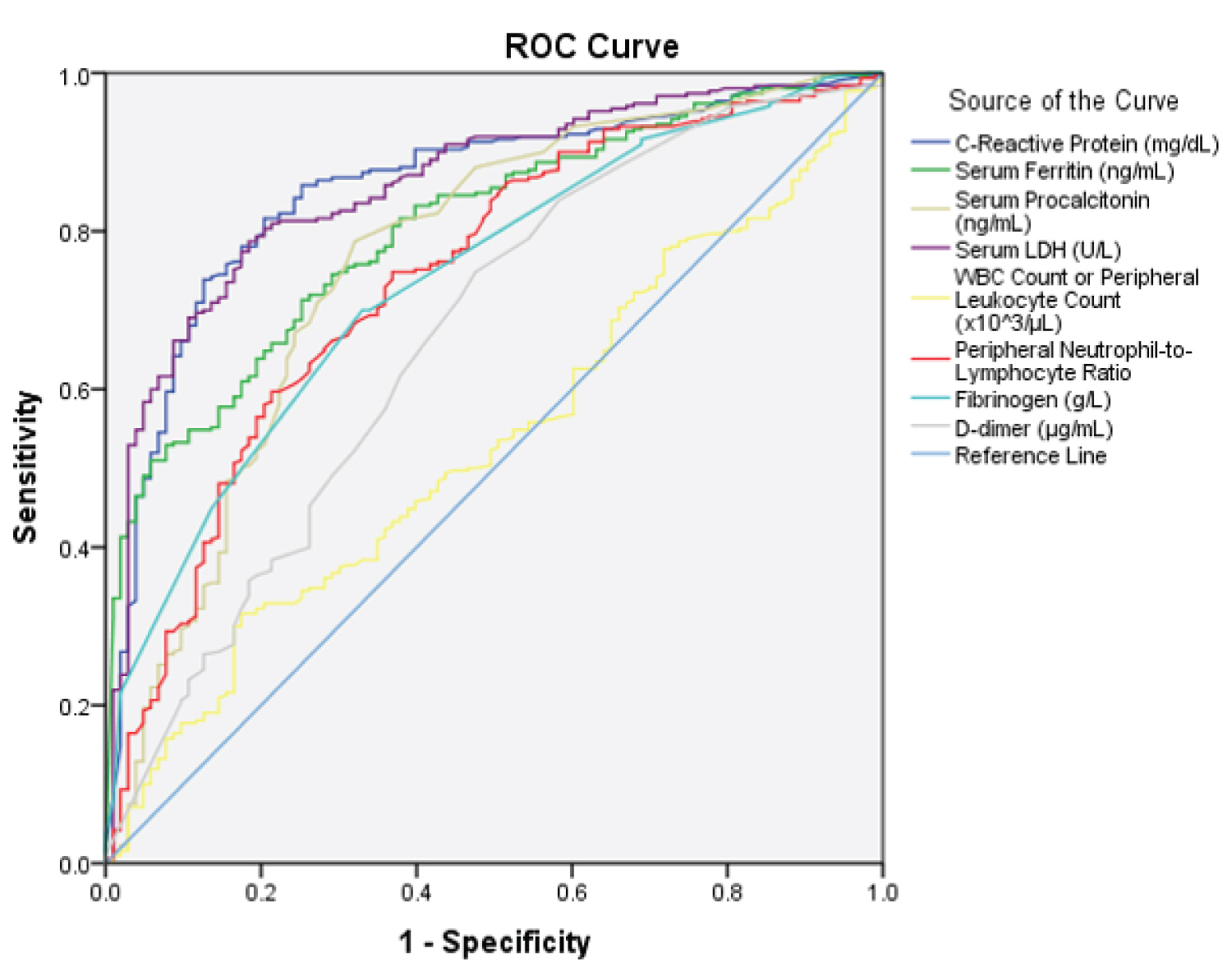 Figure 1: ROC Curve of Potential Predictors namely CRP, LDH, Ferritin, WBC Count or Leukocyte Count,
Peripheral Neutrophil-to-Lymphocyte Ratio, Fibrinogen, D-dimer.
Figure 1: ROC Curve of Potential Predictors namely CRP, LDH, Ferritin, WBC Count or Leukocyte Count,
Peripheral Neutrophil-to-Lymphocyte Ratio, Fibrinogen, D-dimer.
Abbreviation: ROC: Receiver Operating Characteristics; CRP: C-Reactive Protein; LDH: Lactate Dehydrogenase;
WBC: White Blood Cell;
View Figure 1
Table 5: Area under Curve (AUC) of the potential predictors. View Table 5
Table 6: Optimal Cut-Off Values of the Potential Predictors with Sensitivity and Specificity as a Stand-alone Diagnostic. View Table 6
Diabetes is a major risk factor for severity and mortality in COVID-19 like the previous coronavirus infections. Innate and humoral immunity are compromised during periods of hyperglycemic states. These impart the development of an exaggerated inflammatory response and therefore the manifestation of severity [14]. Mechanisms of exaggerated inflammation include increased glucose recognition and binding of C-type lectin receptors and possible changes in ACE2 and protein S glycosylation [15].
Those with cancer are more vulnerable than those with diabetes and much more than the general population. A Chinese nationwide analysis showed that cancer patients with COVID-19 had a higher risk of severe events including ICU admission, need for invasive ventilation, and death [16]. Severe events were more likely when there is an antitumor treatment within the last 14 days [1].
Our results are comparable with other studies which show more severe COVID-19 infection in patients with comorbidities, such as hypertension, cardiovascular disease, chronic lung disease, liver disease, and chronic kidney disease [17]. Although hypertension, cardiovascular disease, and chronic kidney disease are consistently listed in some studies to be risk factors for severity, these were not established in this study using multivariate analysis.
Higher levels of IL-6 as the basis for cytokine storm are not readily available in most institutions. Various surrogate markers came into play. Diagnostic tests that are significant independent predictors in this study are CRP, LDH, and ferritin - consistent with other published studies [4,6,7,18].
Cut-off levels have been reported but are not standardized and vary in different settings. CRP is a good marker for acute-phase inflammation and its production in the liver is induced by IL-6, thus considered as one of the best surrogates for IL-6 [7,19]. Our study shows that CRP > 1.85 mg/dL predicts severe COVID-19 infection with 79% sensitivity and 84% specificity - lower than other studies. Wang, et al. (n = 209) showed that CRP > 2.69 mg/dL is predictive of aggravation of nonsevere COVID-19 patients with 81.3% sensitivity and 79.3% specificity [20]. In the study of Liu, et al. (n = 140), the CRP optimal cut-off at 4.18 mg/dL is predictive of severity with 88.89% sensitivity and 72.73% specificity [21]. A similar study by Herold, et al. (n = 89) finds the optimal cut-off for CPR > 3.25 mg/dL at presentation but aimed to determine cut-off values predictive of the need for ICU admission and mechanical ventilation [19]. However, the population size has been one of the limitations of the above-mentioned studies. This study shows that a lower cut-off level for CRP is owed to the significantly higher number of patients included.
An LDH level > 644.85 U/L predicts COVID-19 severity in this study. Many studies did not include LDH in their investigations. But a meta-analysis showed that LDH is significantly higher in the severe group compared to the nonsevere group [4]. An early study used a lower cut-off value for LDH of 245 U/L comparing non-ICU and ICU patients. Their results showed no statistical difference. However, there were significantly more patients in the non-ICU group with LDH ≤ 245 U/L [22]. Elevated LDH (with cutoffs ranging from 240-253.2 U/L) showed 6.5-fold increased odds of developing severe COVID-19 infection and 16-fold increased odds of death in a pooled study [7]. LDH, an intracellular enzyme, catalyzes the interconversion of pyruvate and lactate and is found in almost all organ systems. It is a marker of hypoxia and organ damage. It is also elevated in cases of myocardial injury, renal failure, thrombotic microangiopathy, and other inflammatory states. Although this study reveals that LDH is a valuable tool for predicting severe COVID-19 infection, caution must be exercised in patients with CKD, as they represent 12.06% of the total population in this study.
A ferritin level > 621.4 ng/mL also predicts COVID-19 severity in this study but with relatively lower sensitivity and specificity compared with CRP and LDH. This could be attributed to the tendency of ferritin to increase during inflammation, as well as in liver disease and malignancy [18]. However, the result is consistent with the meta-analysis that shows ferritin as strong discriminator for severe disease [6,7]. Another meta-analysis reports that ferritin levels were consistently higher in the severe versus nonsevere group and have a potential role in monitoring disease progression [18].
NLR is an emerging hematologic marker for severity of COVID-19. It is readily available since a complete blood count is a routine workup for patients with suspected infection. An increase in NLR is thought to be caused mainly by increased neutrophil count and decreased lymphocyte count. A decrease in both CD4+ and CD8+ T lymphocytes is observed in severe cases. This points to a hyper inflammatory state combined with damage to lymphocytes essential for eliminating virus-infected cells [6,7,10]. This study supports the predictive value of NLR in severe COVID-19. However, NLR with a cut-off value of 4.32 does not show an excellent AUROC. It can give more information if utilized hand-in-hand with the other markers.
Procalcitonin, leukocyte count, NLR, fibrinogen, and d-dimer, did not establish strong predictive diagnostic value in this study. Although procalcitonin, NLR, and fibrinogen have acceptable AUROC values, their independent use in predicting should be at the discretion of the clinician. Respective cut-offs have been established in which the combination of these markers/indices might increase their diagnostic capability [5,8].
The large number of the population included in the analysis was the strength of this study. The study, however, has potential limitations.
The data gathered were solely taken from the database at a one-time period - during the onset of hospitalization. The outcomes after discharge were not followed through. The proponents recommend the inclusion of clinical outcomes in future studies.
This study shows that comorbidities, inflammatory markers, and hematologic indices are significantly higher in severe versus nonsevere COVID-19 disease. Utmost caution and further monitoring at the onset for nonsevere cases with diabetes, cancer, and high levels of CRP (> 1.85 mg/dL), LDH (> 644.85 U/L), and ferritin (> 621.4 ng/mL) are warranted. These cases have a high predilection to become severe or O2 requiring in the course of COVID-19 infection.
Personal information of the patients included in the study was withheld. The proponents did not contact the patients during the study. Upon approval from the Department of Health (DOH) Cluster Ethics Research Committee and the SPMC-Institutional Review Board (IRB), the data collected and analyzed are treated confidential and shall only be used for the sole purpose of the study.
All authors have no affiliation with a direct or indirect financial interest in the conduction of the study. No affiliations, organizations, or entities with financial interest (such as educational grants, honoraria, membership, employment, or consultancies) or non-financial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) are included in the entire provision in this manuscript.
All authors have participated in the design, analysis, and interpretation of the data, draft, and revision of the manuscript, and approval for submission to its final form.
All authors have participated in the design; analysis and interpretation of the data; draft and revision of the manuscript; and approval for submission to its final form.
This research is supported by the Department of Health Region XI of the Philippines in its international publication but has no contribution to the conduct of the study.