Background: Toxoplasmosis is a parasitic infection with public health importance. The aim of this study was to determine the seroprevalence of toxoplasmosis and its risk factors among pregnant women consulted at the Bamenda Regional Hospital.
Methods: This study was a hospital-based cross-sectional study carried out on pregnant women who attended the antenatal clinic at the Bamenda Regional Hospital. Venous blood was collected in dry tubes and analyzed for the presence of Toxoplasma gondii antibodies. A rapid diagnostic test was done with a cassette to detect IgG and IgM antibodies in the serum. The cassette was labeled with the patient's identification number and placed on a flat surface.
The potential risk factors were evaluated with the administration questionnaire using a binary logistic regression model. Statistical significance was measured at P < 0.05.
Results: The overall seroprevalence of toxoplasmosis was 23.9% with 0.85% for IgM and 23.08% for IgG. Women in the second trimester (26.66% for IgG and 3.33% Ig M) of gestation were highly infected than those in the first trimester (20% for IgG and 0% Ig M) but no significant association was reported between the age of pregnancy and toxoplasmosis seroprevalence. High seropositivity (33.33% for IgG and 0% Ig M) was observed in women of age group 23-31, it was not found to be a risk factor for toxoplasmosis, as age was not statistically significant in this study. A statistical significant higher prevalence (20%) was seen in women who had no knowledge on Toxoplasmosis and in single women with seroprevalence (28.13% IgG and 3.13% IgM).
Conclusion: Screening for toxoplasmosis should be done routinely during antenatal care to reduce the risk of transmission from the mother to fetus.
Pregnancy, Toxoplasmosis, Seroprevalence, Risk factors, Bamenda
Toxoplasmosis is one of the most common worldwide parasitic zoonosis caused by the Apicomplexa protozoa Toxoplasma gondii [1]. This parasitic protozoan disease is one of the leading causes of spontaneous abortion or fetal abnormalities [2]. High prevalence of infection has been reported among pregnant women and women of childbearing age from different parts of the world [3]. Toxoplasma gondii is transmitted to humans through ingestion of oocysts in water, food, or soil contaminated with cat's faeces or by eating raw or undercooked meat containing cysts [4] and women can transmit the infection through the placenta to their unborn foetus. Other infectious pathways are blood transfusion and organ transplantation [5]. Pregnant women who are not immunized (negative serology to IgG and Ig M anti-toxoplasmic antibodies) constitute an important risk group. In Cameroon, recent studies have reported seroprevalences of 45.5% in Mbou'o-Bandjoun [6], 71.8% in Limbe [7], 78.6% in the city of Douala [8] and 80% in the city of Yaounde [9]. Although toxoplasmosis serology is among the examinations for the first prenatal consultation, pregnant women at the Bamenda regional hospital neglect this examination because of the lack of knowledge about toxoplasmosis and the high cost of this examination. All these parameters emphasize the need to sensitize pregnant women to the disease. The aim of this study was to determine the seroprevalence of toxoplasmosis and the associated risk factors in the transmission of Toxoplasma gondii at the Bamenda Regional Hospital to develop control strategies for this disease.
This study was carried out at the Bamenda Regional Hospital located in the Bamenda II sub division.
Our study population were pregnant women attending antenatal consultations at the Bamenda Regional Hospital. The sample size was calculated using Lorenz's formula (StatCalc of EPI Info software). Using the prevalence of 34%, with an 80% power to detect significant associations or differences and a 5% accepted margin of error, the minimal sample size estimate was 345 participants.
All pregnant women, attending an antenatal consultation at the Bamenda Regional Hospital and who signed the informed consent form were included. Were excluded all pregnant women with hemophilia and any pregnant women not residing in Bamenda.
A blood collection tube was labelled with the subject's code, sex, and date of sample collection. After choosing a suitable vein on either arm of the participant, a tourniquet was tied on the upper arm to provide pressure for adequate blood flow. Using a syringe, about 4 ml of blood was drawn into a dry tube for analysis.
After collection, the sample was centrifuged at 3000 rpm for 3 minutes to get serum which was used for the analysis. A rapid diagnostic test was done with a Rapid Immunochromatographic test (cassette and Buffer) to detect IgG and IgM antibodies in the serum. The cassette was labeled with the patient's identification number and placed on a flat surface. Briefly, fifty (50) μl of the serum was pipetted into the sample port of the cassette and the results were read after 15 minutes. The appearance of two red/pink lines, one at the test zone and another at the control zone, was indicative of a positive test. While the appearance of a single line at the control zone only this was indicative of a negative test. The absence of the control line was indicative of an invalid test, and the test was repeated.
The ethical clearance to carry out this study was obtained from the Ethical Review Committee/Institutional Review Board of The University of Bamenda, an administrative authorization for research was also obtained from the General Supervisor of the Regional Hospital Bamenda.
The data collected was first recorded in the laboratory notebook and then entered into Microsoft Office Excel 2010. They were then transferred to SPSS version 26.0 (Statistical Package for Social Sciences) for statistical testing. The Chi-square test (x2) allowed us to compare prevalences according to sex, age, neighborhood, level of education, and knowledge of the disease. The Risk Test allowed us to calculate the Odds Ratio in order to determine the risk factors. At p 0.05, the tests were statistically significant. For a variable to be defined as a risk factor its Odds ration must be greater than or equal to 1 and must be within the 95% confidence interval. The p-value shows the strength of the association.
Table 1 presents the socio-demographic profile of the population. It can be seen from this table that the majority of the population was in the age group 23-31 (46.15%), with the highest levels of education being secondary school (33.33%) and university (56.42%). More than half of the populations were married (82.05%) and 82.05% said they did not know about the disease. Based on their occupation, the highest represented were students and others with a total of 33(28.2), each, civil servants 27(23.1), business 18(15.4), and the least represented were farmers with a total of 6(5.1). A total of 15 (12.8) of the participants in this study were in the first trimester, 90(76.9) in the second trimester, and 12(10.3) in the third trimester.
Table 1: Demographic Distribution of the Study Population. View Table 1
Figure 1 shows the overall seroprevalence of IgG and IgM toxoplasmosis. It follows from the analysis of this figure that 23.9% of pregnant women were positive for toxoplasmosis with 1 (0.85%) positive for IgM, 27 (23.08%) positive for IgG.
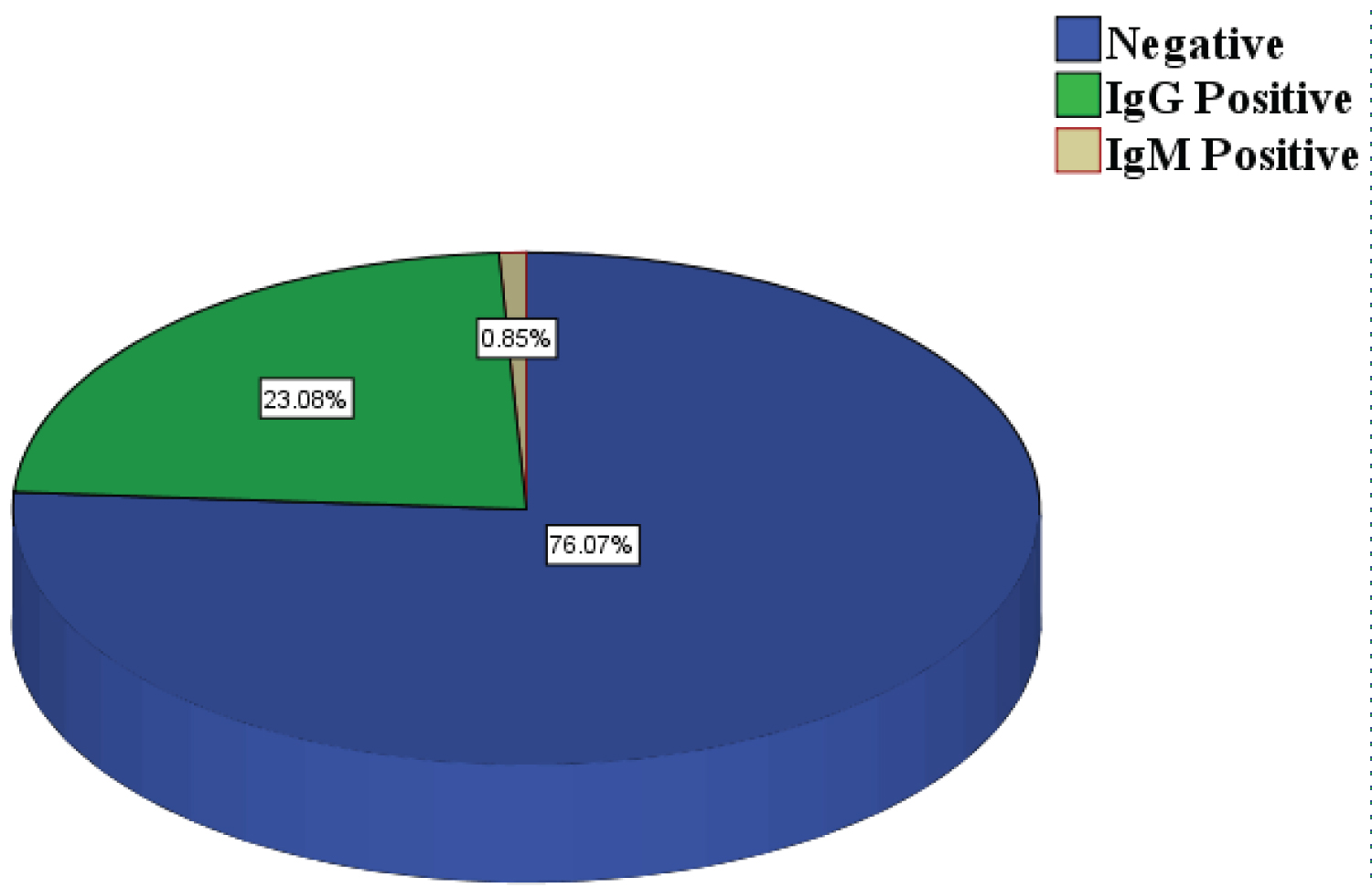 Figure 1: Seroprevalence of IgG and IgM toxoplasmosis.
View Figure 1
Figure 1: Seroprevalence of IgG and IgM toxoplasmosis.
View Figure 1
Table 2 presents the prevalence of toxoplasmosis according to socio-demographic factors. This table shows that there is a statistically significant difference between the levels of education, job occupation, and marital status for toxoplasmosis infection (p < 0.05).
Table 2: Prevalence of Toxoplasmosis According to Socio-demographic Factors. View Table 2
Table 3 presents the risks associated with toxoplasmosis. With regard to level of education, it appears that secondary school subjects are likely to be infested: OR: 4.714; CI: 1.955-11.367; P = 0.002. On the other hand, the risks of infestation with regard to age are relatively equal.
Table 3: Risk factors Associated with Toxoplasmosis. View Table 3
Speaking of occupation and knowledge of the disease, farmers and those who declared "no," not knowing, were at risk of infection, respectively, with OR: 1.111; CI: 0.986-1.252; P = 0.003; and OR: 3.2; CI:1.278-8.015; P = 0.01. Similarly, pregnant women, especially those in the second trimester, and consumers of uncooked meat were also at risk.
This study aimed to establish the seroprevalence of toxoplasmosis and its risk factors among pregnant women followed at the Bamenda regional hospital. The overall prevalence reported in this study was 24.0% (23.1% positive for IgG and 0.9% for IgM). This prevalence is similar to that obtained by Nissapatorn, et al. [10] in Thailand (23.1%). The seroprevalence obtained in this study is lower than in most studies conducted in Cameroon: 34.5% in the Bamenda Regional Hospital [11], 32.5% in Buea [12], and 45.5% in Mbouo-Bandjoun, Western Region of Cameroon [6]. Such variations in toxoplasmosis seroprevalence may be due to differences in geographical location, characteristics of pregnant women such as age, educational level, cat handling, hygienic and feeding habits. Furthermore, the technique used to diagnose the disease may equally explain the differences in prevalence.
The results of the present study reported a significantly associated seroprevalence among pregnant women with a secondary level of education (12.82% IgG and 7.69% IgM). This result contradicts that of Mariam [13] in Morocco, where the level of education does not affect the immune status of pregnant women but are similar to those of Nkain, et al. [9] who reported that pregnant women with primary education were 3.9 times more likely to be infected with T. gondii than those with secondary education.
Our findings showed that women in the second trimester (26.66% for IgG and 3.33% Ig M) of gestation were highly infected than those in the first trimester (20% for IgG and 0% Ig M) but no significant association was reported between the age of pregnancy and toxoplasmosis seroprevalence, which is in agreement with the results reported by Nkain, et al. [9].
High seropositivity (33.33% for IgG and 0% Ig M) was observed in women of age group 23-31, it was not found to be a risk factor for toxoplasmosis seropositivity, as age was not statistically significant in this study. This result is in agreement with that reported by Nguemaim, et al. [11]. This could be justified by the fact that it is during this part of life that women are sexually active and therefore pregnant. On the other hand, age was a statistically significant risk factor associated with IgG toxoplasmosis positivity in a study conducted by Nkain, et al. [9] on the Seroprevalence of Gestational and Neonatal Toxoplasmosis as well as Risk Factors in Yaounde, Cameroon. This highlights the importance of educating young women of childbearing age about the risk factors for Toxoplasma infection.
In this present study, a statistical significant higher prevalence (20%) was seen in women who had no knowledge on toxoplasmosis. This observation clearly shows that seroprevalence is higher when pregnant women do not know about the disease. These results are consistent with those obtained by Kacimi and Ammam [14]. This could be due to the lack of information characterized by the absence of awareness on the part of the health authorities.
Toxoplasma gondii seropositivity was high among participants using tap water. These results are in line with those of Nissapatorn, et al. [10] where 27.01% seropositivity were women who used tap or pipe water.
The job occupation of pregnant women (100% IgG for farmers) was found to be a statistically significant toxoplasmic risk factor. This could be explained by the fact that farmers are always in contact with contaminated soil, which facilitates the exchange and dissemination of parasites. This result contrasts with that obtained by Kouitcheu, et al. [15] in Penka-Michel, who reported a statistically significant association between pregnant housewives and the seroprevalence (47.4%) of toxoplasmosis.
Regarding marital status, a statistically significant association was observed in single women with seroprevalence (28.13% IgG and 3.13% IgM) of toxoplasmosis. In contrast, Nkain, et al. found no significant association between marital status and toxoplasmosis seroprevalence. This discrepancy could be explained by the difference in sensitivity and specificity of the analytical methods [9].
Observations from this study showed that rarely and often consumption of undercooked meat are statistically significant risk factors associated with the seropositivity of toxoplasmosis. This result corroborates that reported by Hamaichat in Morocco [13], who found a positive correlation between the consumption of undercooked or uncooked meat and the seroprevalence of toxoplasmosis. This is probably due to the fact that undercooked or uncooked meat contains tissue cysts of the T. gondii parasite. Contrary to our results, Nguefack, et al. [8] did not find a significant correlation between the consumption of undercooked or uncooked meat and the potential risk of acquiring toxoplasmic antibodies. This difference could be explained by the different dietary habits of the participants in each study. It could also be explained by the analytical methods used in these studies.
The current study reveals the prevalence of toxoplasmosis to be 24.0% among pregnant women who were attending antenatal care at RHB that could justify the importance of having routinely antenatal screening for T. gondii infection.
All data generated and analysed are included in this research article.
The authors declare that no conflicts of interest exist.
The study received no funding from any source or organisation.
YC, NACN, and VKP conceived the idea and designed the study. NFA and GNGA performed the experiments. NFA and GNGA analyzed and interpreted the data. YC, NACN, and VKP drafted the manuscript. All authors read and approved the final manuscript.