Background: The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) Omicron variant was responsible of an increase of the COVID-19 incidence worldwide. This study aimed to investigate the circulation of SARS-CoV-2 Omicron variant (B1.1.529) in the general population in Burkina Faso and provide better preventive strategies.
Methods: This was a descriptive cross-sectional study conducted from November 2021 to November 2022. All individuals with PCR-positive results were tested with the DI SARS-CoV-2 MOC/I Multiplex kit for detection of variants. Innovative Diagnostics DISoft™ analysis software was used to interpret the results. All participants with SARS-CoV-2 positive samples categorized as SARS-CoV-2 Omicron variant (B.1.1.529) with the DI SARS-CoV-2 MOC/I Multiplex kit were included in the study population.
Results: Two hundred and twenty-five SARS-CoV-2 positive samples were analyzed for variant detection. First reported in December 2021 in Burkina Faso, the SARS-CoV-2 Omicron variant was found in 207 samples (83.94%) defining a study population of 207 participants. Out of these 207 participants, 98.55% (204/207) were from the town of Bobo Dioulasso. One hundred and six (51.21%) were males. Their age ranged from 2 Months to 83 years with a median age of 46.38 ± 17.72 years-old. The most represented age group was 40-64 years-old corresponding to 56.52%. Out of 207 patients, 57.97% (120/207) were non-suspected COVID-19 cases. The highest number of SARS-CoV-2 Omicron variant cases was observed in January 2022 representing 42.03% of total cases found between November 2021 and November 2022.
Conclusion: Our study revealed that the SARS-CoV-2 Omicron variant can spread in different age groups, sexes, and in asymptomatic patients. In addition, the SARS-CoV-2 variant would circulate throughout the year but would take advantage of favourable periods to cause new waves. These results provide information on the transmission dynamics of the SARS-CoV-2 variants and should be used for the optimization of future public health measures targeting COVID-19 in Burkina Faso.
Omicron, SARS-CoV-2, Circulation, Bobo-Dioulasso, Burkina Faso
COVID-19: Corona Virus Disease of 2019; SARS-CoV-2: Severe Acute Respiratory Syndrome Coronavirus 2; SSUHC: Sourô Sanou University Hospital Center; MC: Muraz Center, CT: Cycle Threshold
The current coronavirus disease 2019 (COVID-19) pandemic is a global human health crisis caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [1].
Since its outbreak in the late of December 2019, SARS-CoV-2 is rapidly evolving and mutating continuously, leading to the genesis of various variants with variable degrees of infectivity and lethality [2-4]. SARS-CoV-2 variants included Alpha (B.1.1.7), Beta (501.V2 or B.1.351), Gamma (P.1), Delta (B.1.617.2) and Omicron (B.1.1.529) among others [5]. The SARS-CoV-2 Omicron variant is driving the current surge of COVID-19 cases in most countries and is likely to replace 'delta' worldwide [5]. SARS-CoV-2 Variant, B.1.1.529 was first reported on November 24, 2021, in South Africa [6]. On November 26, 2021, the World Health Organization (WHO) named B.1.1.529 as Omicron, a SARS-CoV-2 Variant of Concern [7]. Omicron belongs to Pango lineage B.1.1.529, Nextstrain clade 21K, and is characterised by 30 amino acid changes, three small deletions and one small insertion in the spike protein compared to the original virus. This variant was noticed to have a higher number of mutations than any other previous variants of the virus. Omicron belongs to Pango lineage B.1.1.529, Nextstrain clade 21K, and is characterised by 30 amino acid changes, three small deletions and one small insertion in the spike protein compared to the original virus [8]. A striking feature of SARS-CoV-2 Omicron variant is that it comprises three distinct sub-lineages (BA.1, BA.2, and BA.3) that were discovered near simultaneously, despite each sub-lineage being as different from one another as Alpha, Beta, Gamma and Delta are from one another [9,10]. Subsequently, two other broad sublineages have been defined, BA.4, BA.5, as well as many sublineages within BA.1 and BA.2 [11].
The SARS-CoV-2 Omicron variant has not altered the social demographics of the infected individuals compared to the other SARS-CoV-2 variants. However, it has a significant growth advantage over the Delta variant, resulting in its rapid spread within the community and a higher incidence than previously observed during this pandemic. Although this variant is associated with a lower risk of severe illness and death than the Delta variant, the very high rates of transmission have nonetheless resulted in a significant increase in hospitalization rates, continuing to place massive demands on the health care systems of most countries, and can result in significant morbidity and mortality, particularly in vulnerable populations [12].
The first case of the SARS-CoV-2 Omicron variant in Burkina Faso was reported on December 17th 2021 by the Ministry of Health and Public Hygiene as part of the routine surveillance for SARS-CoV-2 variants [13].
In the last three months before the detection of the SARS-CoV-2 Omicron variant recorded 772, 315 and 993 new cases respectively, for a total of 2080. In the three months following the detection of the SARS-CoV-2 Omicron variant, the country recorded 4.700, 3.147 and 849 new cases respectively, for a total of 8.696. In just three months, the number of new SARS-CoV-2 infections recorded in Burkina Faso has increased by 4 times [14].
However, there is, as of today, no published data on the circulation of SARS-CoV-2 Omicron variant in the general population of the country. This study aimed to investigate the circulation of the SARS-CoV-2 Omicron Variant of Concern in the general population of Burkina Faso.
The Sourô Sanou University Hospital Center (SSUHC) and Muraz Center (MC) are located in the city of Bobo Dioulasso, capital of the Hauts-Bassins region and the economic capital of Burkina Faso. The health coverage regions of the SSUHC, which includes the Haut-Bassins, the Cascades, Boucle of Mouhoun and South-West regions, with a total population estimated at 6,555,016 inhabitants in 2022. This center, with a capacity of 656 beds, has six departments, namely medicine, pediatrics, surgery, obstetrics and reproductive medicine, pharmacy and laboratory. In the context of the coronavirus pandemic, the virology unit of the SSUHC, in addition to being the reference laboratory for the diagnosis of suspected COVID-19 cases, is a surveillance center for SARS-CoV-2 variants. The Muraz Center, founded in 1939, is one of the research organs of the National Institute of Public Health (NIPH) of Burkina Faso. Its mission is to contribute to the prevention, diagnosis and control of diseases through the promotion and implementation of health research. In the context of the Coronavirus pandemic, the MC, in addition to being the reference laboratory for traveller diagnosis, is a surveillance center for SARS-CoV-2 variants. The study was carried out in the section of the virology of the laboratory department at the SSUHC and MC for screening of SARS-CoV-2 Variant of Concern from November 2021 to November 2022.
This was a descriptive cross-sectional study. All persons (asymptomatic: travellers and contact cases and symptomatic: Suspected COVID-19 cases) with a PCR diagnosis during the study period were included in this study. However, only participants with a positive PCR test for COVID-19 followed by detection of the SARS-CoV-2 Omicron variant were included. An exhaustive sampling technique was used in this study.
This study was carried out by collecting data from patient charts as part of the COVID-19 diagnosis. The anonymity of the patients involved in the study was maintained. The results were shared with the Ministry of Health and Public Hygiene as part of the routine surveillance of SARS-CoV-2 variants. Only the laboratory number was mentioned to ensure confidentiality.
Socio-demographic and biological data of the patients were collected using the case report forms [15]. The sociodemographic data included the age, gender, place of residence, status (suspect case and non-suspect case according to the WHO) definition) [16], nature of sample and sampling collection period. Nasopharyngeal, oropharyngeal or naso-oropharyngeal samples were collected for routine diagnosis of COVID-19 using PCR. The biological data was the results of screening for SARS-CoV-2 variants.
The SARS-CoV-2 MOC/I Multiplex DI kit (Innovative Diagnostic, Grabels, France) was used to confirm the detection of SARS-CoV-2 and to screen for its variants according to the manufacturer's instructions. The reactions were run on a CFX96 Touch Real-Time PCR detection System (Bio-Rad) for amplification and mutation detection. The PCR results were analyzed and for further interpreted using the Innovative Diagnostics DISoft™ analysis software [17].
A cycle threshold (Ct) value greater than or equal to 33 cycles for the SARS-CoV-2 CFR610 target corresponded to a sample that was below detection limit for mutations and was not considered for mutation analysis (Figure 1). A cross-over of the mutation profiles of different SARS-CoV-2 variants is used to derive SARS-CoV-2 variants (Table S1) as instructed by the manufacturer.
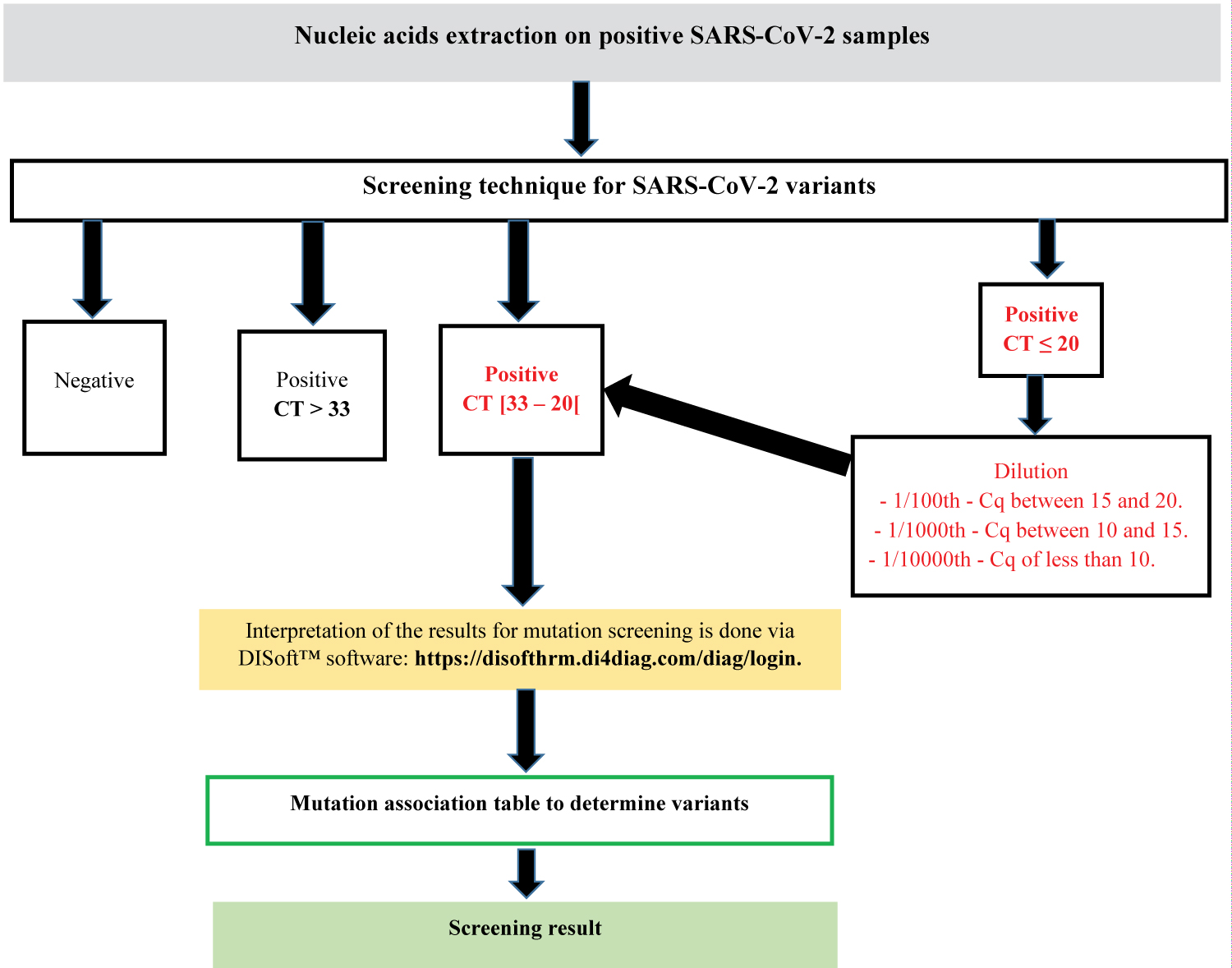 Figure 1: SARS-CoV-2 Screening protocol at Sourô Sanou University Hospital center:
Figure 1: SARS-CoV-2 Screening protocol at Sourô Sanou University Hospital center:
Samples that are positive during routine PCR diagnosis are subjected to the screening test. Positive samples with a Ct of 33 or less will be subjected to interpretation of the results. Interpretation of results for mutation screening is done via DISoft™ software, available at: https://disofthrm.di4diag.com/diag/login.
View Figure 1
Microsoft Excel 2013 and SPSS software (IBM SPSS Statistics 21, Armonk, NY) were used to analyse the data. Quantitative data was described as the mean and standard deviation while qualitative data as the numbers and proportions. Student's t-test for age and Fisher's exact test for gender were used to analyse the results.
During our study PCR diagnosis of COVID-19 was performed on 9237 persons of which 497 were positive (5.38%). Out of the 497 samples, 464 (93.36%) were screened with the DI SARS-CoV-2 MOC/I Multiplex kit. From these 464 samples, 225 (48.49%) were categorized as SARS-CoV-2 variants. Among these, we detected 209 (92.90%) SARS-CoV-2 Omicron variant (Figure 2). The latter was detected for the first time in December 2021. We also detected during this study SARS-CoV-2 non-Omicron variant: Delta, Lambda and Gamma. The SARS-CoV-2 Delta variant ((B.1.617.2), which appeared in Bobo in September 2021, represented a minority in our study population (4.44%). We also observed 2.22% of the SARS-CoV-2 Lambda variant of and 0.44% of the Gamma variant of SARS-CoV-2 (Figure 2). The SARS-CoV-2 Lambda (C.37) and Gamma (P.1) variants were respectively first detected in February 2022 and December 2021 in Bobo Dioulasso.
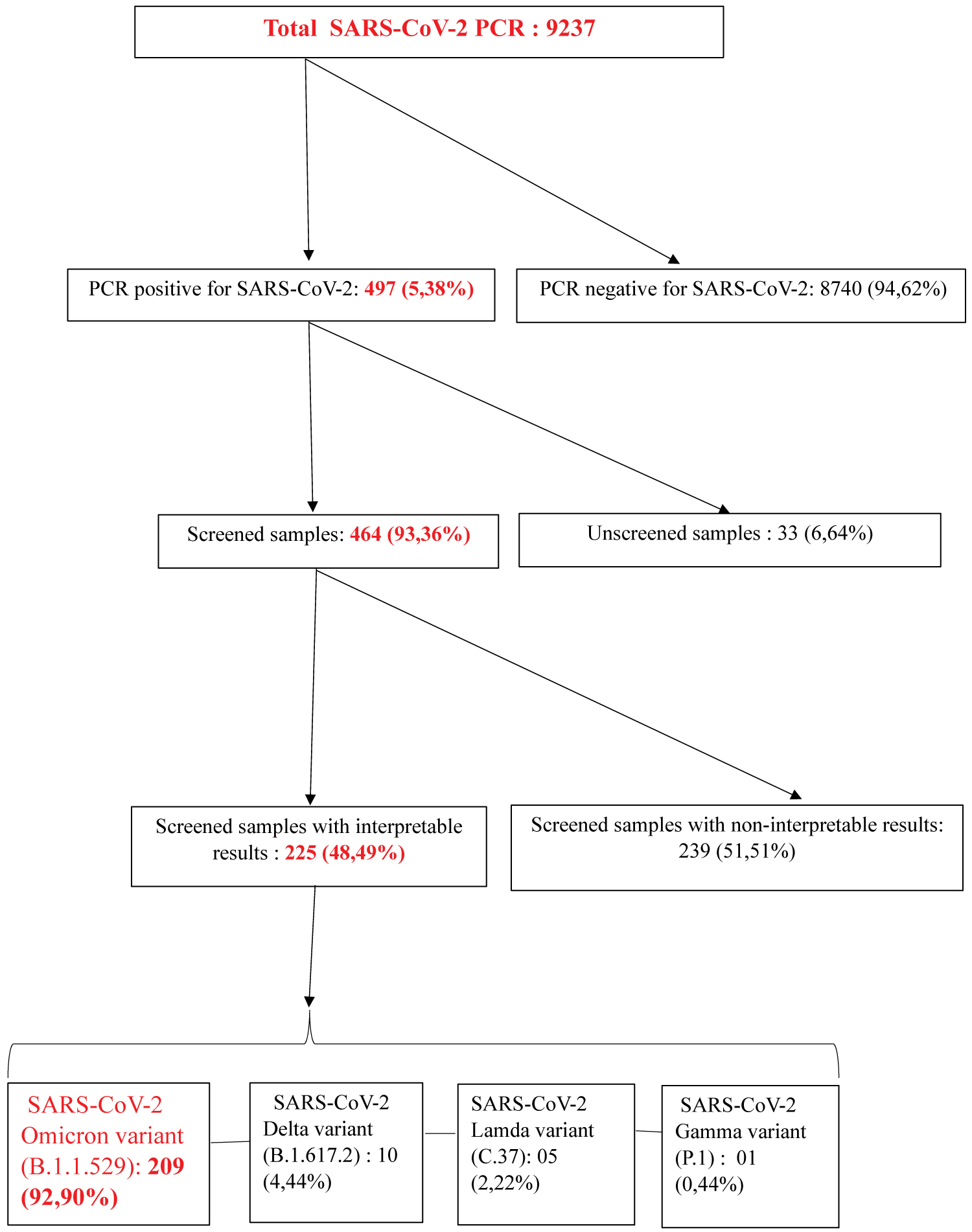 Figure 2: Review of the COVID-19 PCR diagnostic and screening results:
Figure 2: Review of the COVID-19 PCR diagnostic and screening results:
In our study 93.66% of the PCR positive samples were screened and 83.94% of the screened samples were SARS-CoV-2 Omicron variants.
View Figure 2
Out of the 209 SARS-CoV-2 Omicron variants, 2 are without socio-demographic characteristics which justify the use of 207 SARS-CoV-2 Omicron variants for further analysis.
Out of the 207 participants included in this study, 106 (51.21%) were males. Among the participants infected with SARS-CoV-2 non-Omicron variant, 60% were male. The difference was not statistically significant (p = 0.510) (Table 1). The age of the participants ranged from 2 month to 83 years with a median age of 46.38 years +/- 17.72 years-old. We also found a mean age of 44 ± 15.2 years for SARS-CoV-2 non-Omicron variant patients. The difference was not statistically significant (p = 0.613) (Table 1). The most represented age group was 40-64 years representing 61.39% (97 ÷ 158) participants (Figure 3).
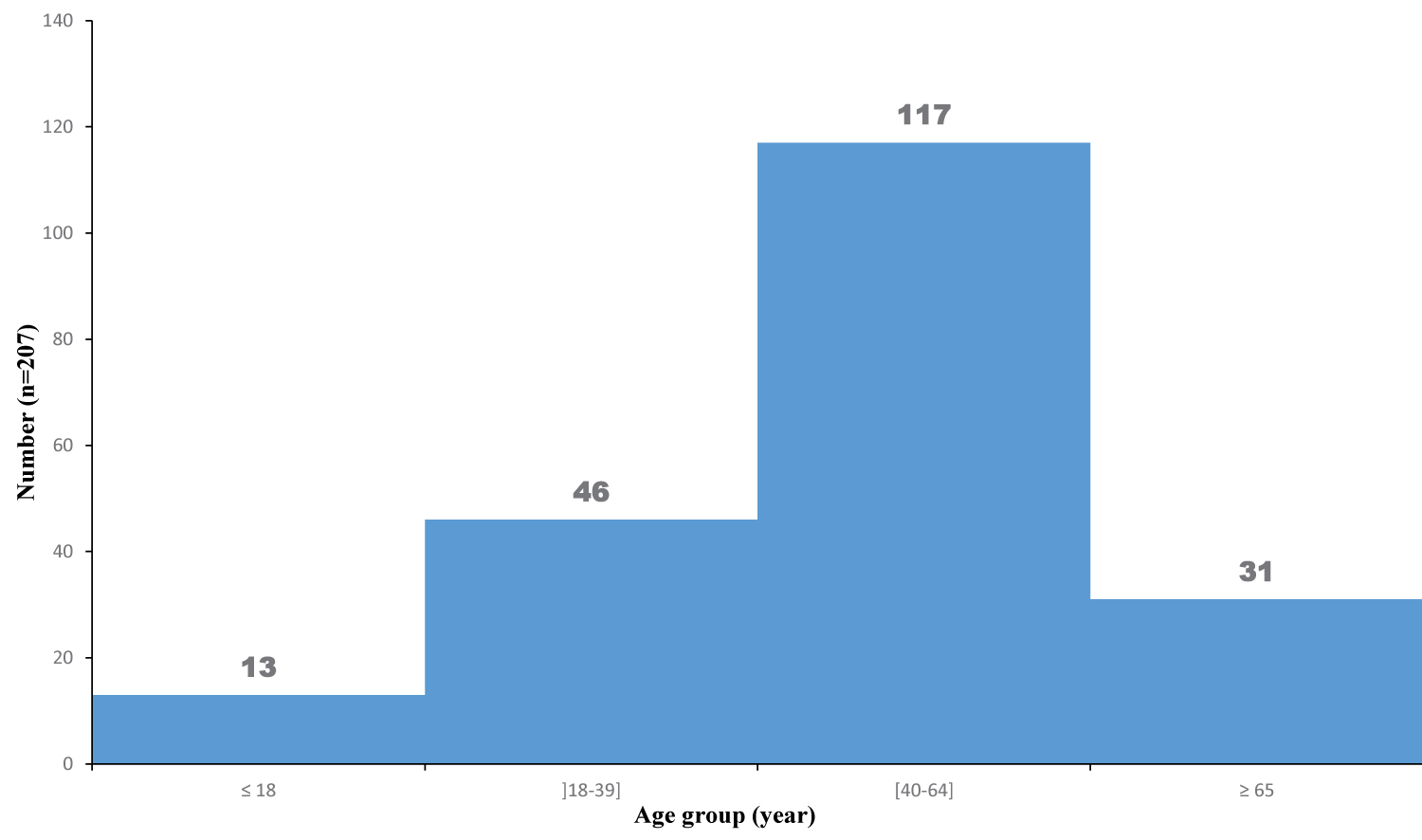 Figure 3: Distribution of patients infected with Omicron by age group:
Figure 3: Distribution of patients infected with Omicron by age group:
The figure showed the age group of 40-64 years-old was most infected with SARS-CoV-2 Omicron variant.
View Figure 3
Table 1: Association of age and gender with SARS-COV-2 Omicron infection:
No statistically significant difference was observed between infection with the SARS-CoV-2 Omicron variant and social demographic characteristics such as age and sex (p = 0.613/0.510).
View Table 1
The majority of the study population consisted of people residing in the city of Bobo Dioulasso (98.56%) (Table 2). Half of the patients were suspected of COVID-19 cases representing 57.97% of the study population.
Table 2: Some socio-demographic characteristics of persons infected with the SARS-COV-2 Omicron variant:
Almost all of the study population (98.56%) is from Bobo Dioulasso with a majority of men (51.21%). There was no difference between suspected and non-suspected cases. Although SARS-CoV-2 Omicron variants of were isolated from all types of specimens, oropharyngeal specimens dominated (56.04%).
View Table 2
Oropharyngeal sample was the most frequent sampling technique 56.04% (Table 2).
In our study, Omicron was not detected in November 2021. Its first detection was in December 2021. The highest number of Omicron was observed in January 2022 corresponding to 42.03% (87/207) of the total cases. From March until May no SARS-CoV-2 variant was detected. We observed cases in June but it was in August that the second wave really took off with a rate of 26.009% (54/207). This study revealed two waves of the SARS-CoV-2 Omicron variant in January and August 2022 after its introduction in Burkina Faso (Figure 4).
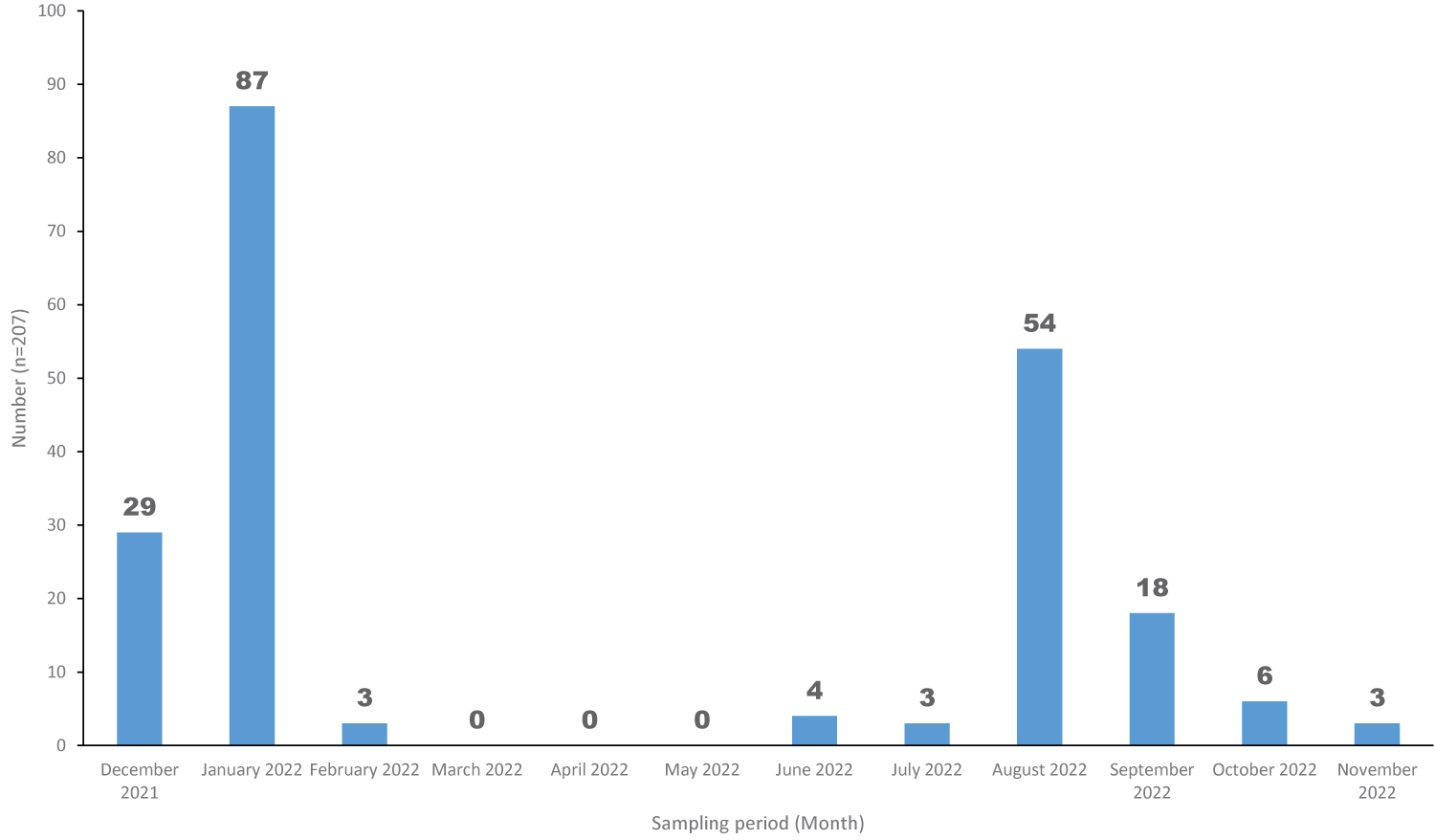 Figure 4: Frequency of SARS-COV-2 Omicron variants according to sampling period:
Figure 4: Frequency of SARS-COV-2 Omicron variants according to sampling period:
We observe two waves with peaks in January (42.03%) and August (26.09%) 2022.
View Figure 4
The purpose of this study was to investigate the circulation of SARS-CoV-2 Variant of Concern in the general population of western Burkina Faso. Although the Delta (B.1.617.2), and Gamma (P.1) variant of SARS-CoV-2 were detected, this study focused exclusively on the SARS-CoV-2 Omicron variants of which represented 92.90% of the variants detected during our study period.
Men were the most affected (51.21%) in this study. In their study on the risk of severe COVID-19 from the SARS-CoV-2 Delta and Omicron variants in relation to vaccination status, sex, age and comorbidities, Kahn, et al. made a different observation by reporting high proportion of women infected with SARS-CoV-2 Omicron variant both in vaccinated and unvaccinated Sweden population [18]. High proportion of female participants (55.2%) was also indicated in the study of Andrews, et al. among persons infected with SARS-CoV-2 Omicron variant [19]. This disparity could lie on the high proportion of men infected with the SARS-CoV-2 in the general population of Burkina Faso as per the data of the Health Emergency Response Operations Centre (HEROC) [20]. Indeed, the latter, which has made it possible to monitor the evolution of the pandemic in Burkina Faso since 9th March 2020 [21], revealed that men were more infected with SARS-CoV-2. This would justify that the SARS-CoV-2 Omicron variant infected the population in the same way as the other previous variants. Also other studies conducted before the emergence of the SARS-CoV-2 Omicron variant reported a male dominance among the infected [22,23]. This would justify the fact that the SARS-CoV-2 Omicron variant had the same circulation as other SARS-CoV-2 variants in the population according to gender. This may be reinforced by the fact that men are more likely to engage in activities that require them to interact with others and to travel. It remains to be seen which age group will confirm this hypothesis. In this study, the most represented age group was 40-64 years with participants of an average age of 46.38 ± 17.72 years. This finding was different from that of the study conducted in the US among patients infected with the SARS-CoV-2 Omicron variant, predominantly in the age group 18-39 years where it correlated with the study conducted in Europe (Sweden) in which the Omicron infection was predominant in the age group of 40-64 years representing 46.7% of the vaccinated participants [24]. Indeed, the rate of transmissibility of SARS-CoV-2 Omicron variant is so high and any age group can be infected with this SARS-CoV-2 variant compared to the Delta variant [25].
The highest number of SARS-CoV-2 Omicron variant cases was observed in January 2022 in this study. Similar results were pointed out in the study of Lambrou, et al. in the USA [26]. Indeed, in the US, the authors showed that the increase in COVID-19 cases in January was due to the SARS-CoV-2 Omicron variant. Indeed, the SARS-CoV-2 Omicron variant first wave started in December 2021 in Burkina Faso and might have reached its peak in January 2022 before starting declining in March 2022. Similar results were observed by Laghdaf, et al. in their study on the characterization of a cluster of COVID-19 cases linked to the SARS-CoV-2 Omicron variant, in Mauritania [27]. Padane, et al. in their study entitled "Rapidly rising cases with Omicronin Senegal" also reported that the 1st case of SARS-CoV-2 Omicron variant was detected in Senegal in December 2021 [28]. This period corresponds to the harmattan in Burkina Faso, which is conducive to the transmission of respiratory diseases. This period is said to be conducive to respiratory diseases linked to the cooling of the body due to the amplitude of the thermal difference between the evening and the morning. It is said to be the period of "cold illnesses" [29]. The SARS-CoV-2 Omicron variant, which is responsible for a highly transmissible respiratory infection, is said to spread easily during this period [28]. It would be important at this time to strengthen protective measures against respiratory infections in general but specifically against SARS-CoV-2. These measures would contribute enormously to stopping the circulation of the SARS-CoV-2 Omicron variant in Burkina Faso.
Although the circulation of SARS-CoV-2 Omicron variant appears to be seasonal, we found isolated cases in June 2022. Indeed, these cases were detected as a result of mass screening of pilgrims expected to travel to Mecca. This would explain that the months in which no cases of the SARS-CoV-2 Omicron variant were found could be due to the low screening rate. Hence the need to strengthen SARS-CoV-2 surveillance in the country to avoid being surprised by a new and more dangerous SARS-CoV-2 variant.
The SARS-CoV-2 Omicron variant being highly transmissible, human movement has favored dissemination locally but also in the surrounding areas of Bobo Dioulasso.
Almost the entire population lives in the city of Bobo Dioulasso 204 (98.55%). Indeed, there are many outpatients from this locality compared to other localities in this study. This could justify the higher SARS-CoV-2 Omicron variant cases in the city of Bobo Dioulasso. Importantly, this study pointed out the presence of SARS-CoV-2 Omicron variant in other cities such as Banfora, Hounde and N'Dorola. This demonstrates the widespread nature of the SARS-CoV-2 variant of concern. Therefore, we recommended the reinforcement of COVID-19 prevention measures nationwide in the advent of new outbreak of SARS-CoV-2 variants.
Our study finally showed that asymptomatic people (non-suspected COVID-19 cases) were infected with Omicron. It would be important to increase the capacity of PCR tests and to raise awareness of the need for regular screening to prevent the development of severe forms of the disease.
This work highlights the importance of actively searching for SARS-CoV-2 variants in order to be proactive in pandemic surveillance.
Overall, this descriptive cross-sectional study provided information on the socio-demographic characteristics of patients infected with SARS-CoV-2 Omicron variant in Burkina Faso. Importantly, our study highlighted that the SARS-CoV-2 Omicron variant can spread in different age groups, gender, and asymptomatic patients. Also, the SARS-CoV-2 variant would circulate throughout the year but would take advantage of favourable periods to cause new waves. These findings could guide on the transmission dynamics of SARS-CoV-2 variants and optimization of future public health measures targeting the COVID-19 in Burkina Faso.
The authors declare that they have no competing interests.
ASO and YS suggested the initial hypothesis, designed the study, acquired and analysed all data presented. The first drafting of the manuscript was undertaken by ASO, YS, JJCS, MS, NFM, AZ, AO, IT, CAO, DK, OK, NDC, EB and ED were equally involved in helping to develop the hypothesis and the critical appraisal/re-writing of the manuscript. All authors have read and approved the final manuscript.
The authors acknowledge Dominique Ouedraogo, Ky Agustin, Maxime Damolga and Abdoul Aziz Belem for their technical helps. Our thanks to Doctor Nicole Prada, General Coordinator of the AFROSCREEN project for her support. We would like to thank medical practitioners at Sourô Sanou University Hospital, Muraz Center, Do, Dafra and Lena district (Bobo Dioulasso) for accompagning us in the inclusion of our participants. Our hearty thanks also to our worthy Souro Sanou University Hospital center and all those that we have inadvertently forgotten for their immense support and encouragement. We cannot finish without saying a big thank you to all the participants in this study.
- Sourô Sanou University Hospital center of Bobo Dioulasso (Burkina Faso)
- Muraz Center of Bobo Dioulasso (Burkina Faso)
This work was supported by the Souro Sanou University Hospital center. Also, this work has been supported by Agence Française de Developpement through the AFROSCREEN project (grant agreement CZZ3209), coordinated by ANRS Maladies infectieuses emergentes in partnership with Institut Pasteur and IRD.
We would additionally like to thank members from the AFROSCREEN Consortium for their work and support on genomic surveillance in Africa [30].
We the authors certify that this work has not been published anywhere else and that all authors contributed significantly to this work.