HIV recency is used to distinguish between a recent HIV infection i.e., within the last 12 months, and a long-term HIV infection. In the era of test and treat, identifying and preventing new HIV infections in undiagnosed individuals remains a high priority in our response to the epidemic especially in effectively interrupting HIV transmission within the population. Recent infection assay helps to diagnose people with recent infection, recent infection data has been used to identify/map out active infection cohorts and areas for targeted HIV testing. Recently, Nigeria adopted recency testing within the HIV case surveillance systems and routine testing services across the country. In this study, we analyzed the implementation of recent infection and its implication for HIV epidemic control.
The Asante recency test kit was used to test newly diagnosed HIV-positive clients on the USAID PEPFAR project in Nigeria for recent infection. SPSS version 22 was used for descriptive analysis and data summary. One way Welch ANOVA was conducted to determine if there was any significant difference in the recency testing yields of the different age groups and the Welch T-test was done to determine if a significant difference exists in the recent infection yield for males and females. Using multinomial logistic regression, we determined how well gender and age range can predict recent infection yield in different regions.
Recent infection assay was conducted for 10,070 clients who were newly diagnosed with HIV over a 12-month period from 10 states across Nigeria. Of these, 1,010 (10%) were recently infected with HIV (Male, N = 389 (3.9%), Female, N = 621 (6.1%)). Clients aged 20-24 years had higher chances of recent infections within the past 12 months compared to the other age ranges within the study. A multinomial regression analysis showed a statistically significant likelihood ratio test for both gender and age range. This means that gender and age significantly improve the yield prediction for recent infection in the states.
The study shows recent infection is higher among females, certain areas, and age groups using RTRI. Programs should include viral load in the algorithm as part of a recent infection testing algorithm (RITA) to improve the classification of recency status of individuals testing recent on rapid test for recent infection (RTRI). Approaches are needed to reach those who are recently infected and map out recent infection clusters/areas for targeted case identification that will ensure we halt the HIV disease transmission to achieve HIV epidemic control.
HIV, Recency tests, PEPFAR, Epidemic control, Recent infection
Globally, HIV/AIDS still remains a major public health issue. Nigeria currently ranks third among the countries with the highest number of People Living with HIV (PLHIV) with an estimated 1.9 million Nigerians living with HIV [1]. Remarkable progress has been made through the concerted efforts of donor agencies and the government of Nigeria, resulting in a steady decline in the HIV prevalence over the years. Improved continuity in treatment and access to antiretroviral therapy (ART) as well as optimal viral suppression rates have also decreased HIV transmission rates in populations [2]. In 2019, the Nigeria AIDS Indicator and Impact Survey (NAIIS) estimated the country's national HIV prevalence to be 1.4% among men and women aged 15-49, with women aged 15-49 years twice more likely to be living with HIV than men (1.9% vs. 0.9%) [3]. This demonstrates an impressive decrease from about 3.4 in 2013 [4].
Recent statistics estimate that about 1.6 million out of the 1.9 million PLHIV in Nigeria have been placed on ART [5]. The implication of this is that although about 85% of PLHIV in Nigeria are on treatment, thus potentially putting Nigeria in a position of achieving epidemic control by 2030, much still remains to be done to sustain control efforts. Effective, and targeted strategies are needed to sustain the drive towards epidemic control. These strategies will ensure HIV testing resources are efficiently directed to finding clients who have never been diagnosed [6-8]. Among such strategies used include index testing and the use of risk stratification tools, which have been effective in targeting PLHIV [9-12]. Nevertheless, such strategies should be complemented by approaches that will ensure we focus on the control of new infections. To achieve this, it is critical to understand the ever changing dynamics of new infections while identifying the populations and areas where active HIV transmission is occurring. This ensures that HIV programs can distinguish those who have acquired recent infections from those with old infections among those newly diagnosed PLHIV [13].
In line with these ever changing dynamics, U.S. President's Emergency Plan for AIDS Relief (PEPFAR) modified its approach to HIV testing and services in a bid to focus testing resources towards areas and populations with the highest transmission rates. In 2020, the PEPFAR program in Nigeria introduced recency testing as part of the country's HIV programming requirement [14]. The program utilized recency tests among new HIV-positive persons to characterize geo-locations and populations among whom new HIV infections are occurring, and to guide prevention efforts to curb ongoing HIV transmission as well as targeted interventions to improve treatment adherence and retention in care among key population groups across the country. In addition, through collaboration with PEPFAR implementing partners across Nigeria, training, supportive supervision, and integrated continuous quality improvement activities were conducted to assure quality service delivery. Currently, USAID/Nigeria is supporting recency testing services in seventeen out of thirty-six states.
This is an interventional study focused on eliciting persons with recent infection believed to drive the HIV epidemic in order to achieve geographically driven targeted HIV testing. We conducted recency testing for newly diagnosed HIV-positive clients on the PEPFAR project using a Asante recency test kit over a 12 month period (October 2020 to September 2021). Recency testing discussions were integrated into pre- and post-tests counseling to sensitize and prepare clients for the test. Clients were then offered a recency test during the retesting for verification of positives prior to treatment initiation phase, in line with the national testing guidelines. The same samples collected for retesting were also used to conduct the recency test. Following the recency test, two lines known as the control and the verification lines will appear on the Asante Rapid HIV-1 Recency test kit. A control "C" line is constant. The appearance of a third line known as the Long Term (LT) line indicates a long-term infection. Consent was sought from every client who made an informed decision following robust pre-and post-test counseling sessions.
The data was summarized using descriptive analysis on SPSS version 22. One way Welch ANOVA was conducted to determine if there was a statistically significant difference in the recency testing yields of the different age groups and the Welch T-test was done to determine if a statistically significant difference exists in the yield for males and females. Pearson Chi-square was used to determine if the data from one state, Niger state disaggregated by gender was due to chance or not. Multinomial logistic regression was done to determine how well gender and age range can predict recency yield in the states.
1. Newly positive HIV clients in the last 12 months who had a recency test to elicit recent infection.
2. Clients with recent HIV test results within the same period.
1. HIV-positive clients outside the 12-months window.
2. Recent infection results outside the assessment period of 12 months.
A total of 10,070 newly diagnosed HIV positive clients from 10 states were tested for recent HIV infection in 12 months across the program. Of those, 4260 (40%) identified as male while 5801 (60%) identified as female. A total of 1,010 (10%) out of the 10,070 newly diagnosed PLHIV tested positive with the Asante recency diagnostic kit and were therefore classified as having a recent HIV infection. This implies that 9060 PLHIVs (90%) were found to have long-term HIV infection. A higher proportion of those with recent infection was found among clients within the age group 20-24 years (Figure 1). With the exception of 1 state (Niger state), female clients had higher recent infections than males (Figure 2 and Figure 3).
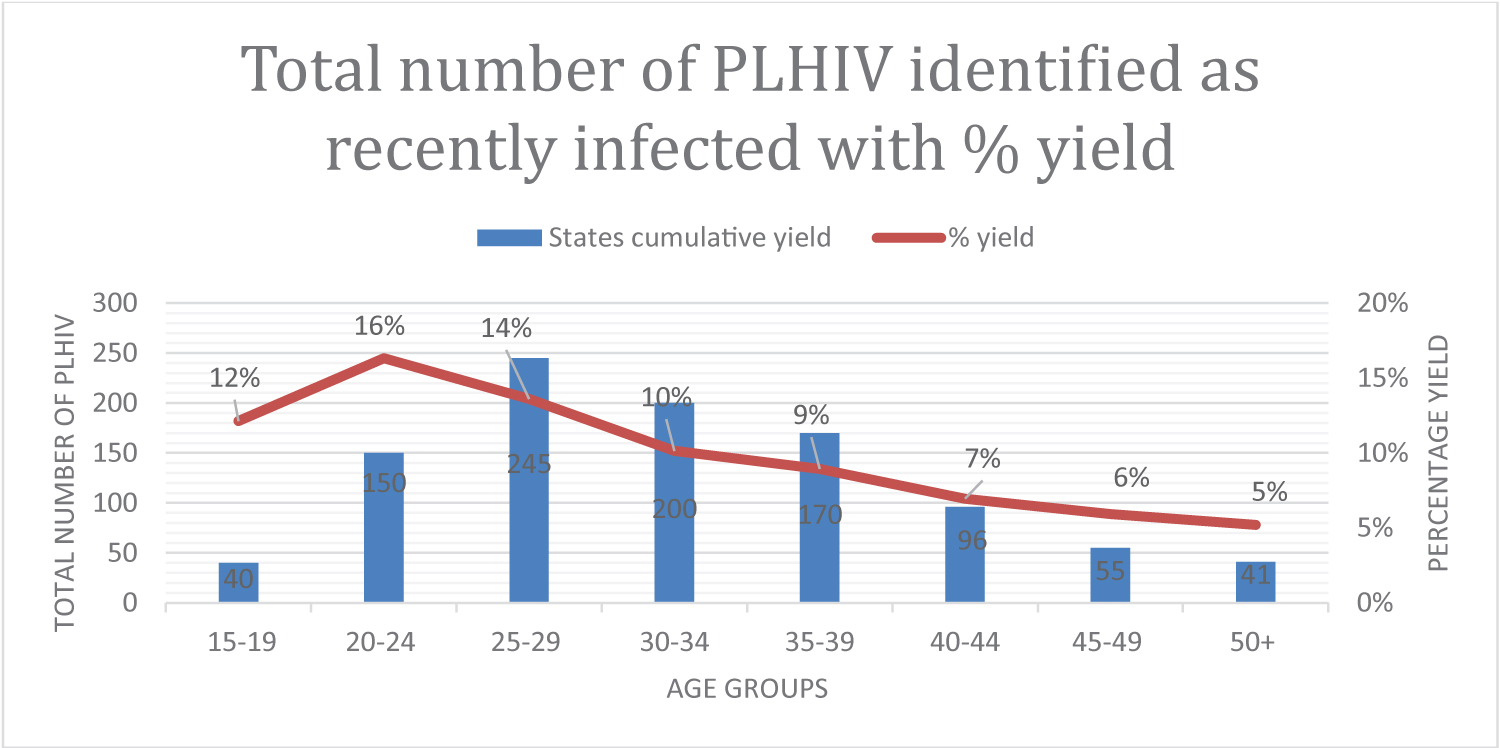 Figure 1: Newly diagnosed and recent HIV infections by age. Cumulative yield and percentage yield disaggregated by age range.
View Figure 1
Figure 1: Newly diagnosed and recent HIV infections by age. Cumulative yield and percentage yield disaggregated by age range.
View Figure 1
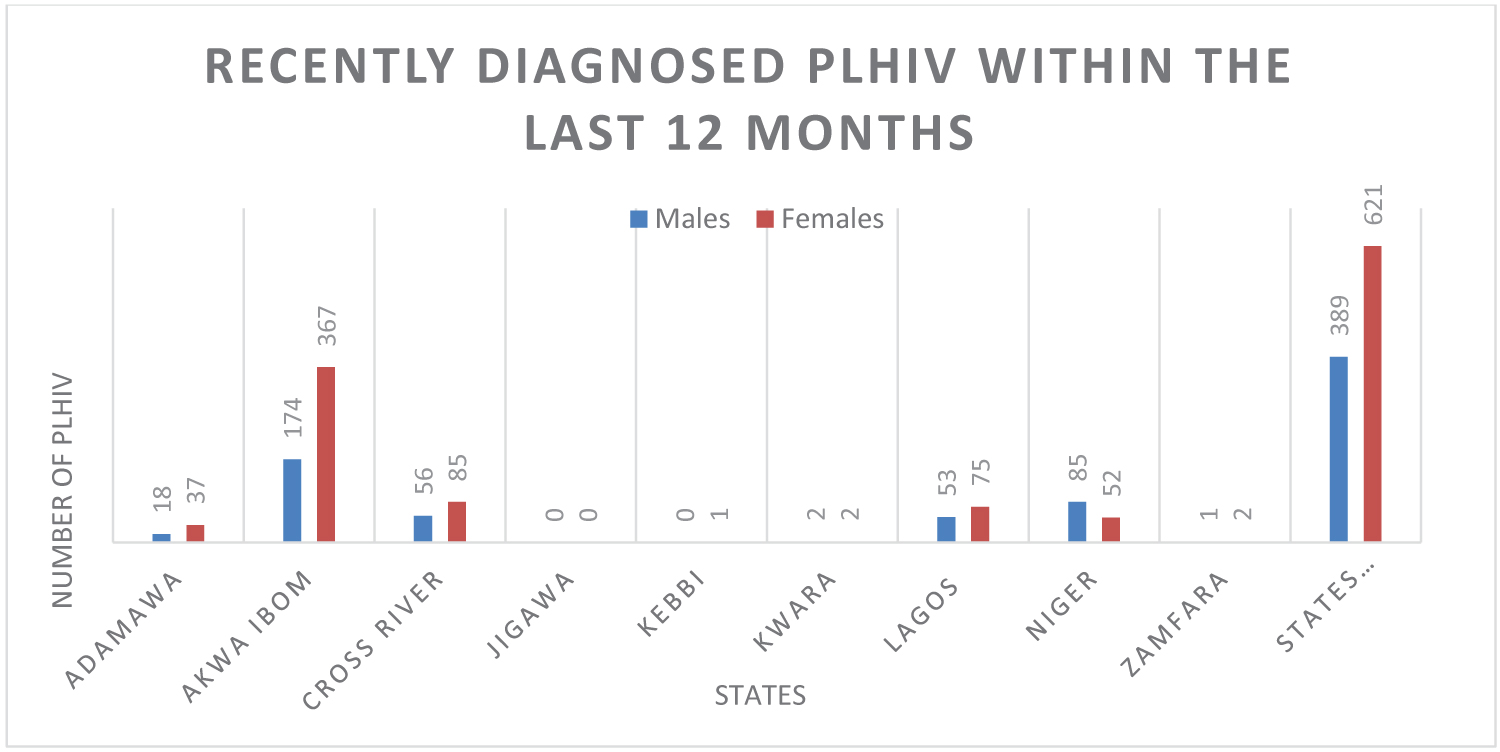 Figure 2: Newly diagnosed and recent HIV infections by States. PLHIV recency test numbers disaggregated by geographic location and sex.
View Figure 2
Figure 2: Newly diagnosed and recent HIV infections by States. PLHIV recency test numbers disaggregated by geographic location and sex.
View Figure 2
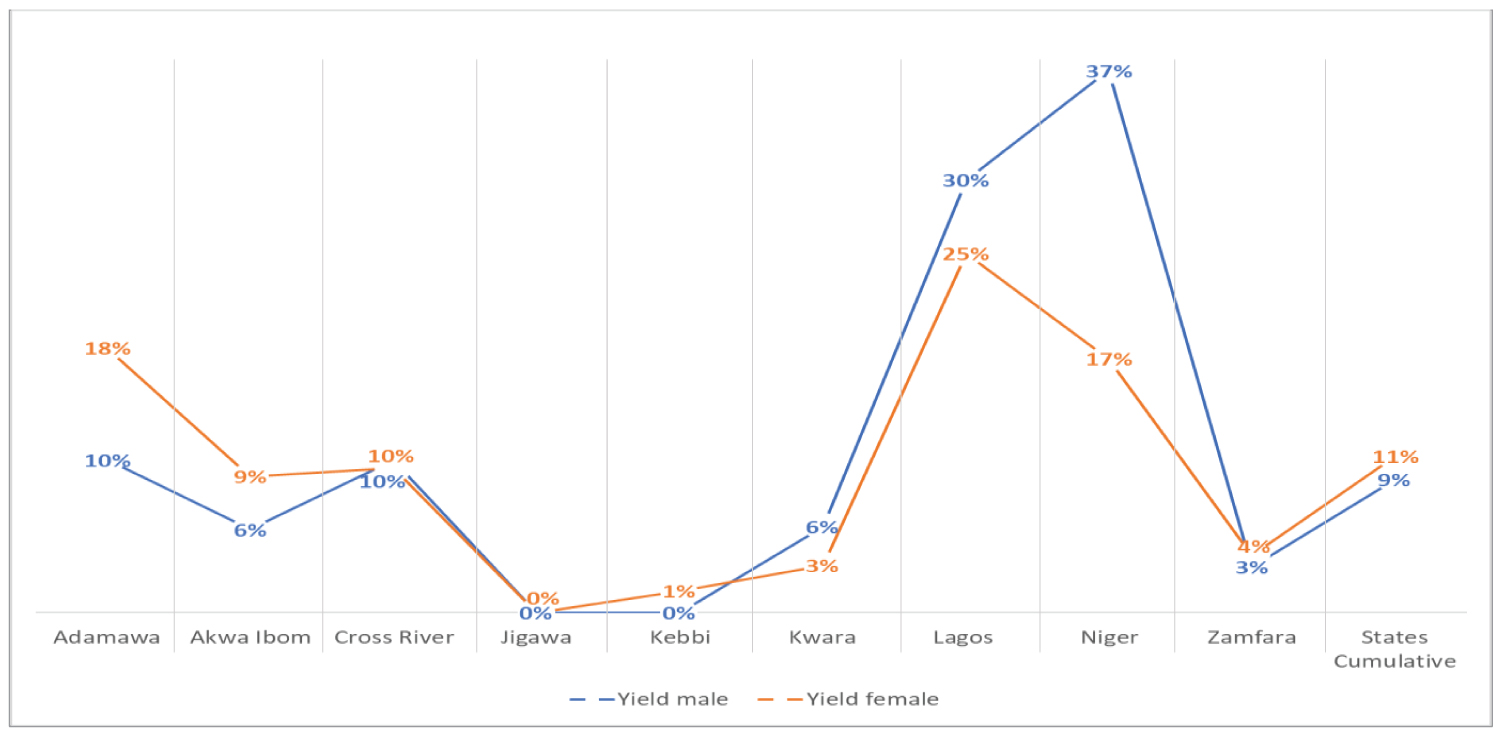 Figure 3: Proportion of recent infections in states with newly identified HIV infection. Percentage recency test yield per state yield disaggregated geographic location by sex.
View Figure 3
Figure 3: Proportion of recent infections in states with newly identified HIV infection. Percentage recency test yield per state yield disaggregated geographic location by sex.
View Figure 3
There was a statistically significant difference between the yield in the different age groups as demonstrated by one-way Welch ANOVA (Welch's F (7, 304.463) = 183.574, p < 0.0005). A Games-Howell post hoc analysis revealed that the difference in the mean for the age groups with the highest (20-24 years) and lowest (15-19 years) recency yield was statistically significant. A Welch T-test showed the difference in the mean yield between males and females was statistically 131 significant, with a mean difference of 131. 624 (95% CI = -144.635 to -118.613); t (873.43) = 132 19.855; p < 0005.
There was a strong association and a significant positive trend between gender and recent infection classifications in Niger state. A Pearson Chi-square demonstrated a statistically significant association between gender and recent infection in Niger state with the males more likely to have a recent infection than the females (X2 = 15.467; p < 0.0005). A multinomial regression analysis showed a statistically significant likelihood ratio test for both gender and age range (Table 1 and Table 2). This means that gender and age range significantly improve the yield prediction in the states. A Welch t-test was run to determine if there was a difference in recency test yield between males and females.
Table 1: Age Result of Likelihood ratio test of multinomial regression. View Table 1
Table 2: Gender Result of Likelihood ratio test of multinomial regression. View Table 2
Recency tests are now being used in several settings across sub-Saharan Africa, such as in HIV trials, population surveys and routine surveillance based on PEPFAR guidelines [13,15-17]. In this study, we conducted a retrospective multicenter analysis of USAID Nigeria's recency testing data over a 12-months period. To the best of our knowledge, our study is the first to analyze recency data after Nigeria launched recency testing in 2020 to map and identify new HIV infections.
Our study collected data from 10,070 HIV-positive clients (male = 40% (4269); female = 60% (5801)) in 10 states in Nigeria who were tested for recent HIV infection. Of those, 9,060 (male = 43% (3880); Female = 57% (5180)) were found to have long term infection while 10% (n = 1010) were identified to have acquired HIV infection recently. When comparing the 10% recent new infection rate of clients in our study, we found that this proportion of recent infections among those diagnosed with HIV mirrored new incidence trends in sub-Saharan Africa in studies conducted in Rwanda and Kenya [15,18]. Rwibasira, et al. in their study conducted in Rwanda
between 2018 and 2020 found that 9.5% of clients whose samples were sent for a recency assay tested positive for newly acquired HIV infection [18]. In the other study conducted in Kenya, the authors found that 8.6% of clients in their study population who had been newly diagnosed with HIV infection received results that showed that they had recently been infected in the prior 12 months of the study period [15]. However, when comparing our rates to that of a study conducted in the UK which used a more sensitive assay, the recent infection testing algorithm (RITA), we found that they had a higher recent infection rate of 14.7% [19].
Gender stratification of new infections in our study showed that females accounted for 61% (621) of the total HIV recent infections compared to their male counterparts (39% (389)). This finding is consistent with a study conducted in Kenya which found that females accounted for 67% of new HIV infections [15]. We theorize that this might be as result of increased health-seeking behavior among females thereby necessitating increased HIV testing among this group. This corroborates with findings from another study in Rwanda, which found that women represented 70% of the total HIV recent infections when compared to men in the study population [18]. Reasons such as the imbalances in the negotiating power for safe sex among females, and the complex interplay of biology, socioeconomic and cultural factors may explain why women are at an increased risk for new HIV infections [20].
Our findings showed that the age group 20-39 years accounted for 76.7% (n = 765) of recent infections identified. Further stratification showed that the highest number of recent infections was found in clients in the age range 25-29 years (n = 245) accounting for 25% of recent infections, however, recent infection yield was higher in the age range 20-24. Clients in the age range 15-19 years accounted for the lowest yield of recent infection. This observed difference could be because of increased transgenerational transactional sex within these age groups. This finding is similar to that of a study conducted in Rwanda, which found that the age group 20-39 had the highest rate of recent infection in the study population [18].
Geographically, the southern part of Nigeria (Lagos, Cross Rivers, and Akwa-Ibom states) had the highest rate of recent infections compared to the other states in the study. This observed difference could be because of the cosmopolitan nature of these states in the southern part of Nigeria. High- risk behaviors are common in these areas [4], and thus there are more HIV-specific intervention programs located therein. One of such interventions is the PEPFAR ART surge program which is implemented in Lagos and Akwa-Ibom States (both states were classified as red states based on the National AIDS survey) [21]. This has resulted in a higher HIV-testing volume in these states than other states. Also, since residents in these states are more likely to get tested for HIV than the other states, they have an advantage of increased access to HIV-testing services, facility mentoring of staff as well as education about HIV prevention, HIV testing and treatment services. All of these, which have implications for HIV resource management.
Our study findings have implications for the Nigeria HIV control program. The data has improved the understanding of current transmission trends and the identification of epidemiological clusters, populations, and geographies with the highest recent infection rates in the country (age group with the highest new recent infection rate: 20-39 years; geography most affected: Southern Nigeria; and gender with highest rates: Females), which is currently informing our targeted approach to reducing new HIV infections. This will also help to judiciously manage limited resources for HIV prevention, testing, and treatment services on groups of people or geographic locations with the greatest potential benefit. The outcome of this study will also be used to improve HIV case identification through other critical epidemiologic clusters that drive the HIV epidemic in Nigeria.
Nigeria's inclusion of recency testing as part of their HIV strategy to achieve epidemic control by 2030 has proved effective in identifying high-risk individuals, population, and areas with undiagnosed HIV infections. Since its introduction and use in the country, there has been increased identification of new or undiagnosed HIV infections. The information from this study and recency data has been triangulated with other data sources such as program and national survey data, and used to map hot spots and population groups with higher infection risk and are more likely to transmit the HIV virus. In addition, the recency data has promoted and enhanced the use of real-time HIV surveillance data to improve the granularity of control efforts to monitor HIV incidence trends and identify concentrated and generalized epidemics in the population. However, according to the PEPFAR COP 23 technical guidance, the use and results of recent infection assays should not solely lead to targeting specific areas for HIV testing, but that the assessment of the direction of the HIV epidemic through ongoing surveillance of newly diagnosed HIV infections remains essential to ensure that prevention and clinical interventions are efficiently and effectively delivered to persons at risk of acquiring or transmitting HIV infection’ [22].
Recency testing needs to be fully integrated into the HIV testing services because it supports monitoring trends of active transmission even as HIV Testing services are being provided to all who require the services and active linkage to prevention /and or treatment services is being ensured. This approach will help Nigeria to achieve epidemic control of HIV/AIDS by 2030 based on UNAIDS 95-95-95.
The analysis focused on using data obtained from rapid test for recent infection (RTRI). There are concerns about the reclassification rate for recent infections when RITA is used in addition to RTRI.
Further studies that will include viral load in the algorithm is recommended as part of a recent infection testing algorithm (RITA) to improve the classification of recency status of individuals testing recent on rapid test for recent infection (RTRI). This is due to the high reclassification rates (ranging from 30-60%) of recent infections when using RITA.
The authors declare that they have no competing interests.
MK conceptualized the study and drafted the initial version of the manuscript. MK, AU, AA, AA, and AA contributed to data collection tool design, data collection and analysis. MK and AA did the statistical analyses. MK, AU, AA, AA contributed to the interpretation of the findings, drafting the manuscript, and provided significant input into the paper. HM, and RG provided leadership for the HIV program for USAID Nigeria. MK, AA and MB prepared and revised the manuscript for submission.
We would like to thank all the study participants. This project was made possible thanks to PEPFAR and USAID funding and support. We would like to thank the support of the implementing partners, health workers and states. The funding bodies had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript. The findings of the study do not represent the views of the funding agency, but those of the authors.
Funding for this research has been supported by the President's Emergency Plan for AIDS Relief (PEPFAR) through USAID. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The datasets generated and/or analyzed during this current study are not publicly available due their sensitive nature but are available from the corresponding author on reasonable request.