Zinner syndrome is indeed a rare congenital condition characterized by urogenital system malformation, specifically involving abnormalities of the mesonephric/Wolffian duct. It typically presents with the triad of unilateral renal agenesis, ipsilateral seminal vesicle cyst, and ipsilateral ejaculatory duct obstruction. We present a case of an 8-year-old male child with a prenatal diagnosis of solitary kidney (right renal agenesis) and the subsequent identification of a globose right seminal vesicle with a cystic appearance. This finding is consistent with Zinner syndrome.
Diagnosis of Zinner syndrome relies on imaging studies, with magnetic resonance imaging (MRI) being the most accurate diagnostic tool. In the majority of cases, treatment is conservative, aimed at managing symptoms and complications as they arise rather than surgical intervention.
Zinner syndrome, Renal agenesis, Seminal vesicle cysts, Infertility
We present a case of an 8-year-old male child, with irrelevant family history, and a prenatal diagnosis of solitary kidney- right renal agenesis. He performed a renal and bladder ultrasound at 4 weeks of life, which confirmed the presence of right renal agenesis and left kidney with mild vicarious hypertrophy, without other alterations. He also performed DMSA renal scintigraphy, which confirmed right renal agenesis (Figure 1). He began follow-up in a pediatric nephrology consultation and at 10-month-old, a renal and bladder ultrasound identified a solitary kidney and a globose right seminal vesicle, with a cystic appearance (Figure 2), alterations compatible with Zinner syndrome. The patient remains asymptomatic and without alterations in the physical exam, performing ultrasound control every 6-12 months, presenting alterations compatible with Zinner syndrome.
Zinner syndrome is a rare congenital condition, due to the urogenital system malformation (abnormalities of the mesonephric/Wolffian duct), presenting as a triad of unilateral renal agenesis, ipsilateral seminal vesicle cyst and ipsilateral ejaculatory duct obstruction [1-4]. This condition is quite uncommon, with fewer than 200 cases reported in the medical literature, and its estimated incidence is approximately 0.00035% to 0.0046% [2].
Patients with Zinner syndrome are often asymptomatic during their early years but may develop symptoms in their second or third decades of life due to the enlargement of the cysts. Infertility is a significant concern, affecting approximately 45% of individuals with this syndrome. Other clinical manifestations, while nonspecific, can include urinary tract infections, hematuria, dysuria, urinary urgency, suprapubic/perineal pain, pain after ejaculation, epididymitis, and prostatitis [1-4].
Imaging is essential for the diagnosis of Zinner syndrome, with magnetic resonance imaging (MRI) being the most accurate exam. In the vast majority of patients, treatment is conservative (rather than surgical), aimed at managing symptoms and complications as they arise [2,3].
The authors emphasize that despite being a rare disease, it is important to alert the family about the follow-up of patients with solitary kidney and cystic seminal vesicle. The control of vicarious hypertrophy and the surveillance of proteinuria are mandatory.
However, if you suspect that a child may have Zinner syndrome due to specific symptoms or circumstances, here are some steps to consider:
1) Consult a Pediatric Specialist: If a child exhibits unusual urological or reproductive symptoms or has a family history of related conditions, start by consulting a pediatric urologist or nephrologist. They can conduct a thorough evaluation and order appropriate tests.
2) Imaging Studies: The primary diagnostic tool for Zinner syndrome is imaging, with MRI being the most accurate. An MRI can help identify any structural abnormalities in the urogenital system.
3) Medical History: Provide a detailed medical history, including any relevant family history, to the healthcare provider. Be sure to mention any urological, reproductive, or abdominal symptoms the child may be experiencing.
4) Clinical Evaluation: The healthcare provider will perform a physical examination to assess any signs or symptoms that may be suggestive of the condition.
5) Additional Testing: Depending on the clinical findings and the results of imaging studies, additional tests may be required to confirm the diagnosis.
The authors declare no conflict or competing interests.
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
These authors contributed equally to this work.

Figure 1: DMSA renal scintigraphy, confirming right renal agenesis.
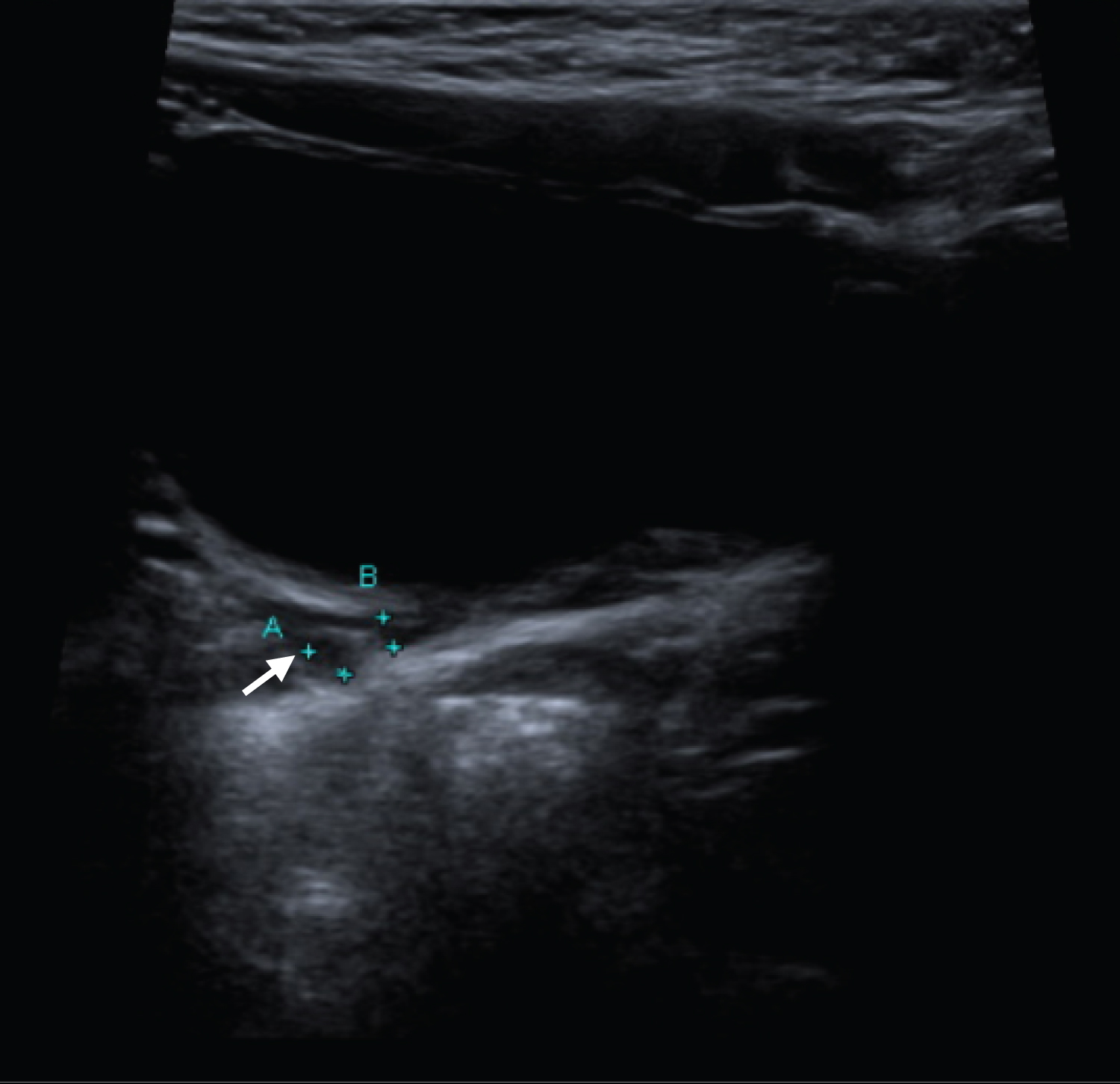
Figure 2: Suprapubic bladder ultrasound, showing the right seminal vesicle with a cystic appearance (white arrow).