A 60-year-old female with history of hypertension presented to the emergency department following a sudden fall while walking 3 hours prior. The patient was unable to move her both legs and unable to void. During evaluation, she also developed a sudden onset of sharp mid-sternal chest pain. Her blood pressure was 213/126 mmHg in right arm and 170/131 mmHg in left arm and heart rate was tachycardic at 110. Bilateral lower extremities motor strengths were not present with intact sensory functions. Ankle reflexes were absent bilaterally.
Chest X-ray showed mediastinal widening (Figure A, red arrow). Computed tomographic angiography of the chest, abdomen and pelvis revealed type A aortic dissection, which involved the ascending aorta (Figure B, blue arrow), descending aorta (Figure B and Figure C, purple arrow), right external iliac artery and left internal iliac artery. MRI spine was consistent with anterior thoracic spinal cord/cornus infarct at the level of T2.
The patient underwent successful emergent type A aortic dissection repair within 3 hours. Initially, bilateral lower extremities paraplegia remained unchanged and she continued to have neurogenic bladder requiring indwelling urinary catheter. Her lower extremities motor function started to improve 2 weeks after the surgery.
Acute aortic dissection can be a life-threatening condition which can result in spinal cord infarction [1]. In patients with acute neurologic symptoms which may be related with spinal cord infarction, aortic dissection should be considered and carefully investigated. A high clinical suspicion with prompt diagnosis can lead to emergent intervention and prevent morbidity and mortality [1-3].
All authors have reported that they have no relationships relevant to the contents of this paper to disclose.
All authors have contributed equally to this paper.
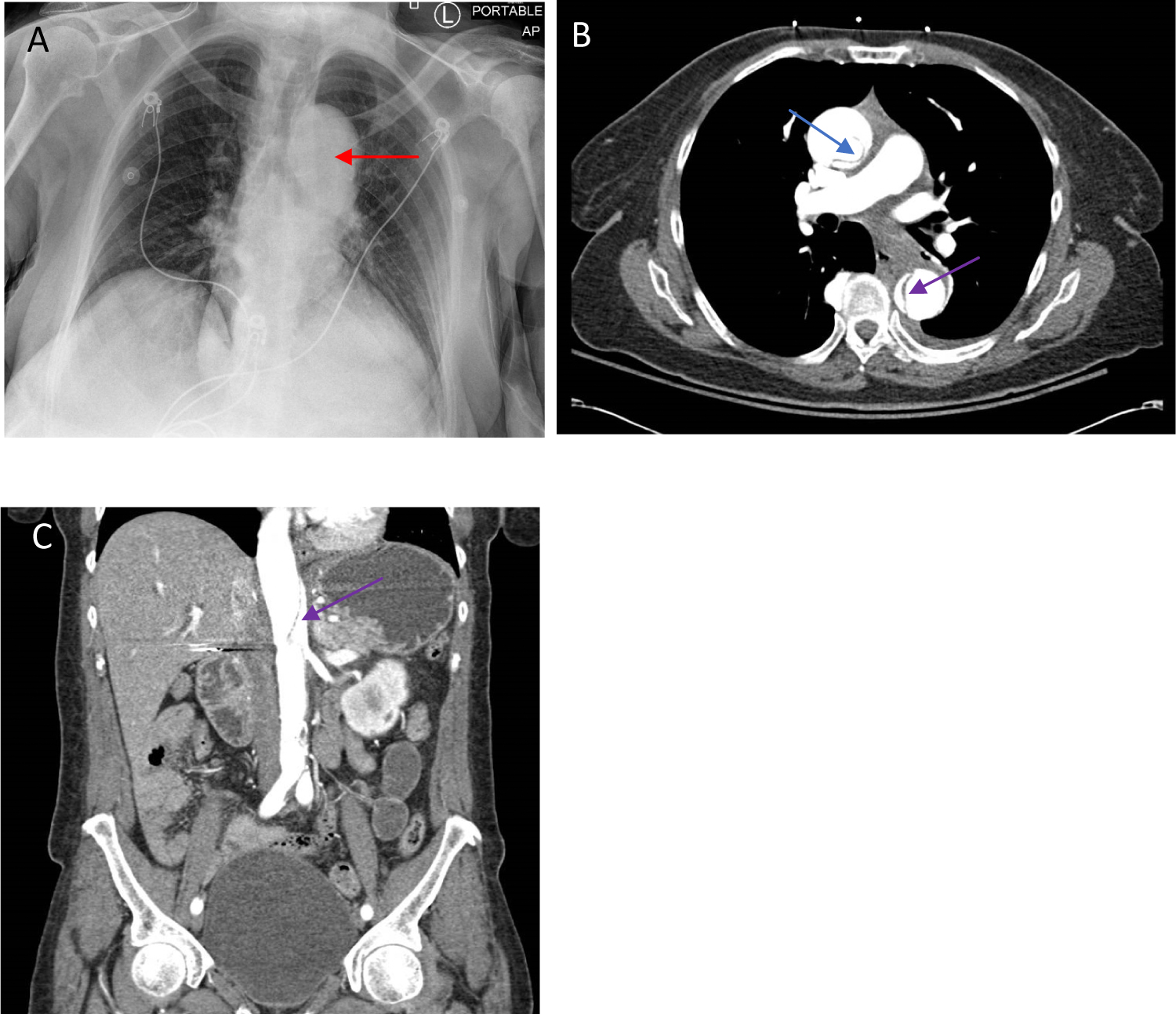
Figure 1: (A) Chest X-ray showed mediastinal widening (red arrow); (B,C) Computed tomographic angiography of the chest, abdomen and pelvis revealed type A aortic dissection, which involved the ascending aorta (Figure B, blue arrow), descending aorta (Figure B and C, purple arrow).