Pacemaker, Tricuspid Valve, Vegetation, Tricuspid Regurgitation
Pacemaker implantation has a very fascinating history. Since the first implantation of human pacemaker technological advancement has helped tremendously in the evolution of different types of pacemaker. Dedicated work by different scientist at different times has enriched the knowledge of several aspects of implantation gradually. Over the time the technology has been modernized to adapt the need of pacing in different clinical situations. However one thing remained constatnt throughout this long history of pacing technique and that is chances of infection and its complications. Infection of the pacemaker lead itself is not uncommon in medical literature. Formation of vegetation, clot, and mass has been reported in pacemaker lead. Here we have reported one such case of pacemaker lead vegetation in a 56-years-old lady. VVIR pacemaker was implanted in this lady 6 years back due to occurrence of syncope in the background of complete heart block. She was doing well until few months back when she had fever. She took medications from nearby healthcare facility but fever persisted. Complete blood count revealed increased TLC with neutrophilic predominance. CRP, ESR was also found to be high. She was started on antibiotics therapy which resulted in defervescence for 2 weeks after which she had fever again. She was advised for CXR and echocardiography. Echocardiogram revealed echogenic structure attached to RV pacing lead and moving along with the lead from RA to RV (Figure 1 and Figure 2). Patient had severe tricuspid regurgitation which is evident in Video 1. Patient was admitted empirical antibiotics therapy started after sample of blood culture was sent. Reports of blood culture including fungal culture were negative. Although percutaneous extraction of pacemaker lead could be done but considering the size, tethered nature of vegetation, fibrosis of the lead due to long history of pacemaker she was transferred to department of Cardiothoracic surgery for extraction of lead. Figure 1 and Figure 2 depicting the pacemaker lead vegetation which is visible from RA to RV attached with the RV lead and moving along with it. Tricuspid valve leaflet was free from any attachment to vegetation. Video 1 showing the vegetation mass along with severe tricuspid regurgitation and dilate RA.
None.
None.

Figure 1: Depicting the pacemaker lead vegetation which is visible from RA to RV attached with the RV lead.
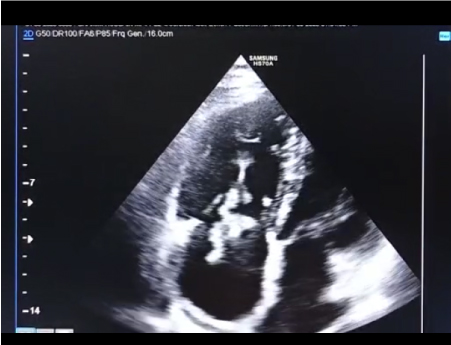
Figure 2: Showing the vegetation attached to RV lead and septal leaflet is free along with dilated RA.