Calcinosis cutis is a condition in which calcium salts are deposited in the skin and subcutaneous tissue. It may be associated with connective tissue disease and rarely with lupus disease. We report a historical case of extensive calcinosis cutis universalis secondary to Systemic Lupus Erythematosus (SLE) associated with lupus panniculitis.
Calcinosis cutis is a condition in which calcium salts are deposited in the skin and subcutaneous tissue. They constitute a heterogeneous group of connective tissue disorders and may be associated with connective tissue diseases. We report a historical case of extensive calcinosis cutis universalis secondary to Systemic Lupus Erythematosus (SLE) associated with lupus panniculitis.
We report the case of a 37-year-old woman with SLE associated with lupus panniculitis diagnosed in the year 2000. Ten years after diagnosis, she spontaneously developed several isolated, hard, erythematous, and painful plaques with ulceration on the entire skin. She suffered from the progression of purulent and chalky, milk-like discharge from the ulcerative wounds (Figure 1A and Figure 1 B); even with oral prednisolone treatment (the dose was 20 mg per day).
The laboratory data showed normal serum calcium, phosphorus, parathyroid hormone, and muscle enzyme levels. A plain film X-ray showed numerous small soft tissue calcifications extensively scattered over her pelvic region (Figure 2A), thigh, knee, and lower leg (Figure 2B). However, computed tomography revealed that the calcified lesions were only present in the skin and subcutaneous tissues, with no muscle, vessel, or visceral organ invasion (Figure 3A). Pathology of the skin and subcutaneous tissue showed multiple calcified nodular formations and moderate dermal lymphocyte infiltration (Figure 3B). The diagnosis was extensive calcinosis cutis universalis. The patient received bisphosphate 10 mg/kg/day for 6 months and diltiazem 30 mg/day for more than 1 year, and intralesional corticosteroids. However, the general condition still progressed.
Calcinosis cutis is classified into five main types: Dystrophic, metastatic, idiopathic, iatrogenic, and calciphylaxis. Dystrophic calcification is the most common cause of calcinosis cutis and is associated with normal laboratory values of calcium and phosphorus [1]. It is frequently observed in connective tissue diseases, including systemic scleroderma (CREST: Calcinosis cutis, Raynaud's phenomenon, Esophageal dysfunctions, Sclerodactily and Telangiectasia), dermatomyositis and overlap syndromes. However, the association with systemic lupus erythematosus is more rarely reported [2]. All reported cases have shown a female predominance with an average onset of 9.8 years after the diagnosis of SLE [2]. Clinically, it may present as "calcinosis circumscripta" mainly in the fingers and periarticular regions or even more rarely as "calcinosis universalis" [3]. Due to the rarity of this entity and the uncertainty of the pathophysiological mechanism, there are no guideline standards of treatment. However, various treatments have been reported to be beneficial such as Probenecid, Diltiazem, Aluminum hydroxide, Wafarin, colchicine or bisphosphonates. Surgical excision remains an option in cases of functional discomfort, compressive phenomena, or painful symptoms in case of ulceration or superinfections [4].
We report a historical case of extensive calcinosis cutis universalis secondary to SLE associated with lupus panniculitis. To our knowledge, no case has been described in the literature associating this triad. To date, there is no "validated" treatment for skin calcifications. The management of secondary complications is a constant challenge in the follow-up of these cases.
The authors declare that they have no competing interests.
All the co-authors contributed to the realization of this work, read and approved the final manuscript.
Written consent for publication of this article has been obtained from our patient.
Nil.
None.
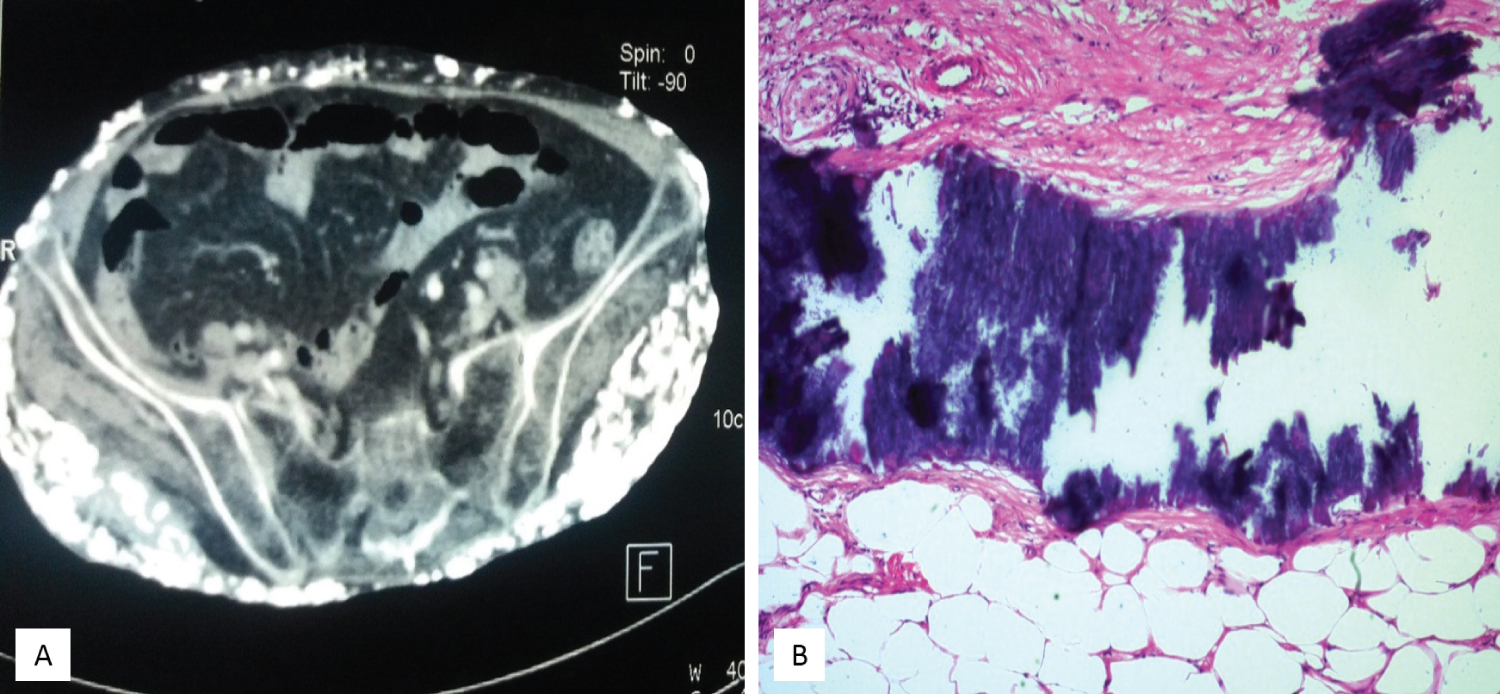
Figure 1: (A) Generalized calcifications in a patient with SLE associated with panniculitis; (B) Trans-epidermal removal of chalk whish material.
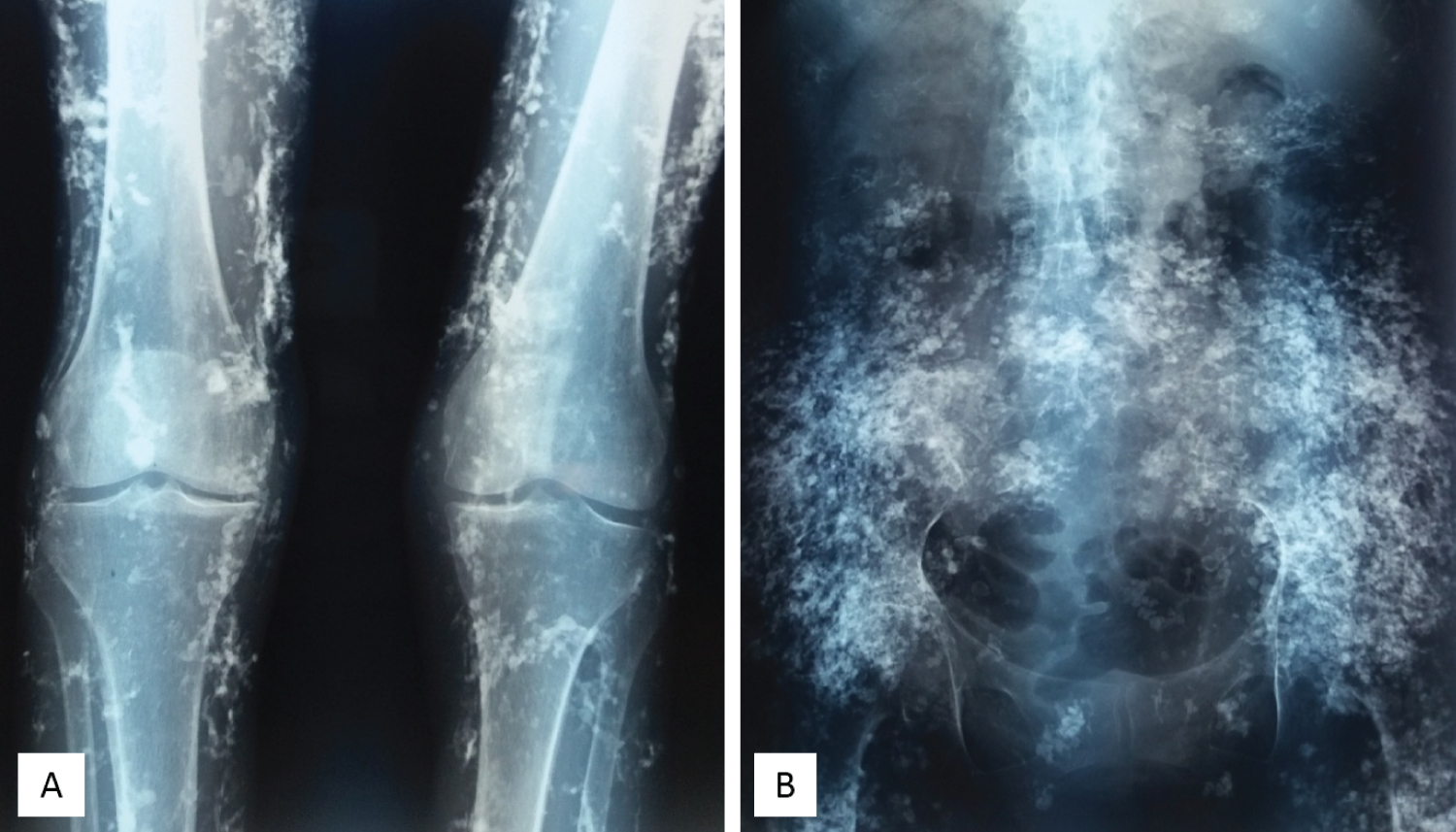
Figure 2: Plain film X-ray shows (A) Extensive soft tissue calcifications over the thigh, knee, and lower leg; (B) Numerous small soft tissue calcifications extensively scattered over the patient's pelvic region.
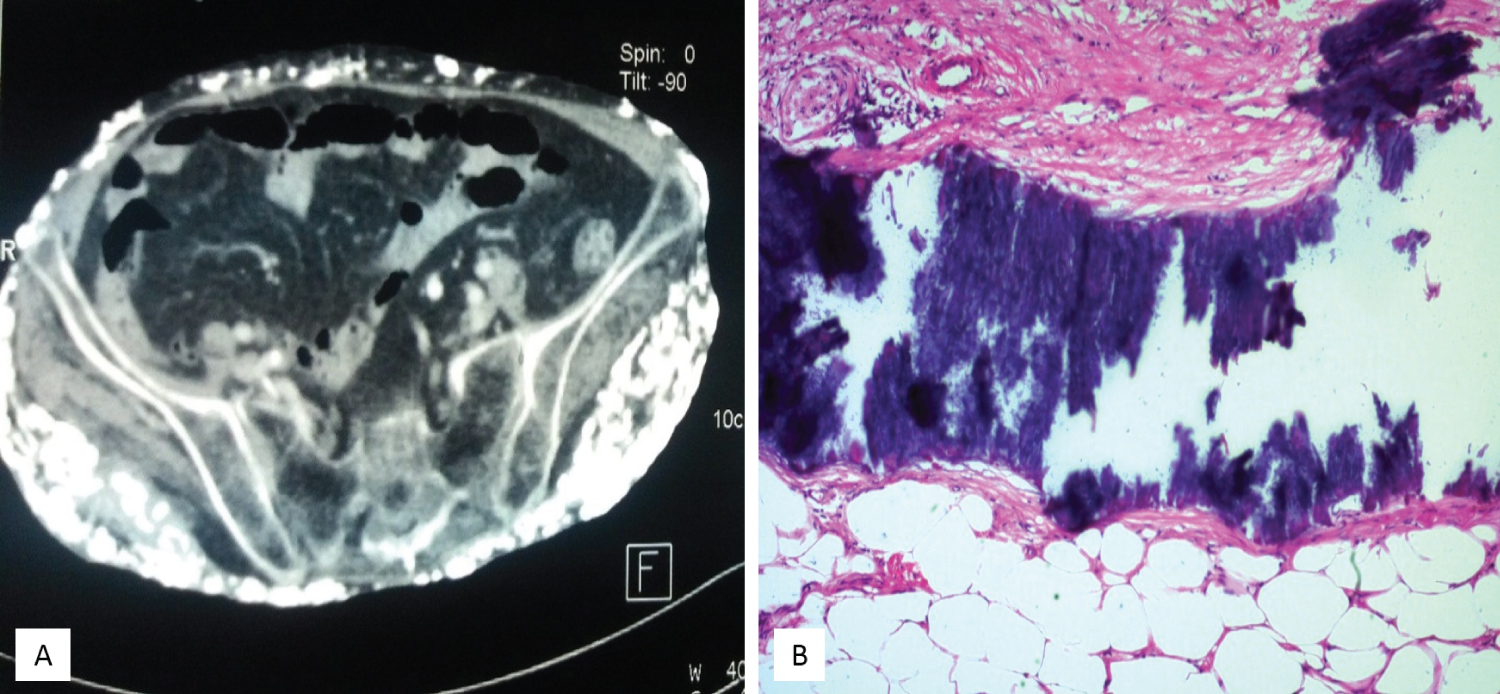
Figure 3: (A) Computed tomography shows calcifications involving the subcutaneous fat space and respecting the muscle planes and fascias; (B) Pathology of the skin and subcutaneous tissue reveal patches of black-colored staining, indicating tissue calcification.