Mycosis fungoides represents the majority of the primary cutaneous T-cell lymphomas. Folliculotropic Mycosis Fungoides (FMF) is an aggressive variant of Mycosis Fungoides (MF) with a tropism at the follicular epithelium. Trichoscopic features of FMF are rarely studied in the literature. A case of FMF of the scalp in a 38-year-old female is discussed.
Folliculotropic Mycosis Fungoides (FMF) is an aggressive variant of mycosis fungoides characterized by preferential infiltration of the follicular epithelium by atypical T lymphocytes, with or without follicular mucinosis or infiltration of the intervening epidermis [1]. It mainly affects the face and scalp and lead to alopecia that is a common feature of FMF and can be scarring or non-scarring. Trichoscopic features of FMF are rarely studied in the literature. A case of FMF of the scalp in a 38-year-old female is discussed.
A 38-year-old woman presented with a 3-months history of pruritic alopecic plaques on the scalp. Histopathology and immunohistochemistry confirmed the diagnosis of CD8+ mycosis fungoides. On clinical examination, there were several alopecic plaques at the frontal and temporal areas of the scalp. Pull test from different areas of the scalp (lesional and nonlesional skin) showed anagen hairs with intact root sheaths. Plaques were erythematous and ulcerated with yellowish crusts and a circinate border (Figure 1). On dermoscopy, there were orange-yellow areas, unstructured white areas, milky white globules and white and black dots. The vessels were linear and some hairs were in zigzag and in exclamation point (Figure 2). The bacteriological sampling of the scalp was negative and the patient received retinoids at 25 mg/day and PUVA therapy with a healing start of the lesions after 4 weeks but with scarring alopecia (Figure 3).
Various trichoscopic aspects of FMF have been reported in the literature such as the presence of milky-white globules, yellow and white dots, white scales, and white dots with radial lines that replaced the hair follicles [2]. Zigzag hair, short hair with split-end, short hair with triangular-shape end, broken hair and pigtail appearance hair are also reported [2]. Others have described the presence of milky-red globules, orange-yellow patchy areas and the vascular granular well-margined milky-red areas surrounded by normal skin in MF patients with scalp involvement [3]. Another observation with comedonal lesions [4] and a spiky follicular Mycosis Fungoides were also reported [5].
Mycosis fungoides is a great imitator and can simulate a wide variety of benign inflammatory skin disorders. Trichoscopy can help in clinical diagnosis of FMF on the scalp but should be followed by histopathology and immunohistochemical study to definite diagnosis. Further studies are necessary to determine the sensitivity and specificity of each trichoscopic feature.
The authors declare no competing interest.
All the co-authors contributed to the realization of this work.
Nil.
None.
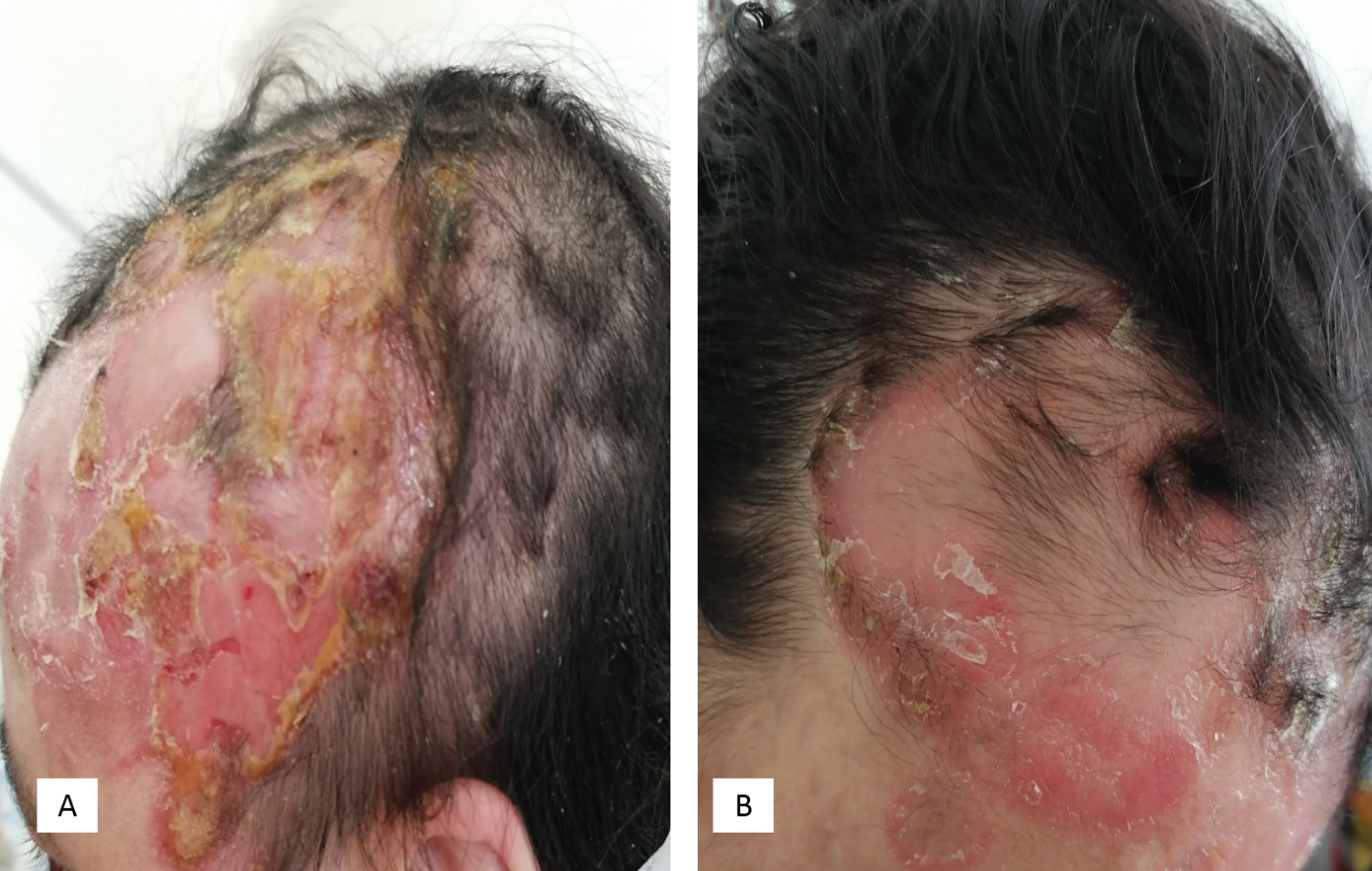
Figure 1: (A) Alopecic plaques of the scalp; (B) Erosive plaques of the scalp surmounted by yellowish crusts with circled edges.
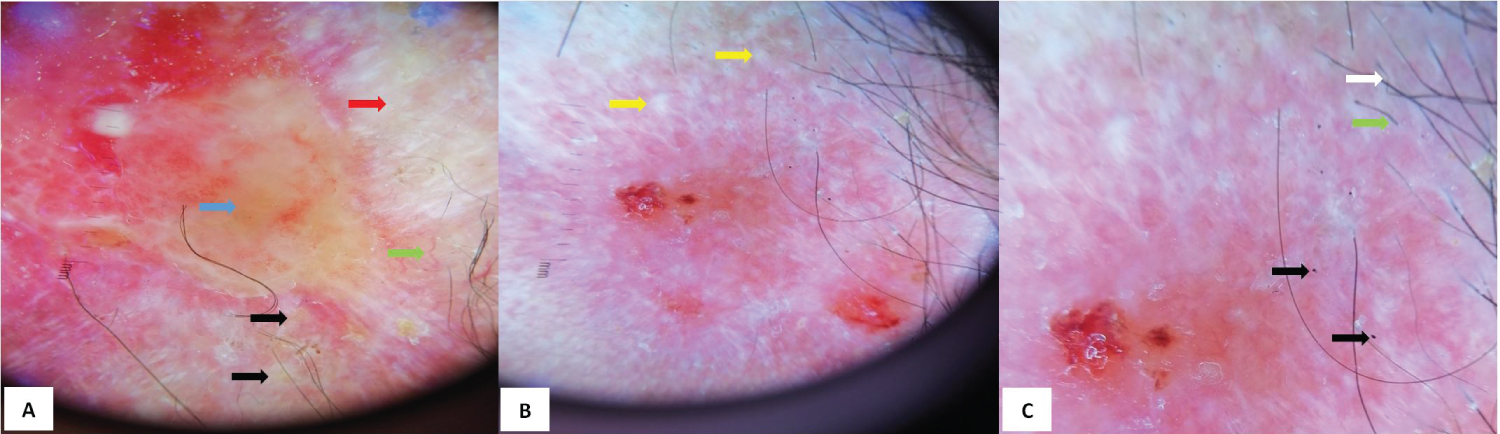
Figure 2: Dermoscopic features of scalp FMF (A) Yellow-orange areas (blue arrow), white areas without structure (red arrow), milky white globules (black arrow) and linear vessels (green arrow); (B) White dots (yellow arrows) with disappearance of hair follicles in the center of the lesion and persistence of some fluffy hairs in the periphery; (C) Zigzag hairs (white arrow), exclamation point hairs (green arrow), black dots/broken hair (black arrow).

Figure 3: Evolution of the lesions of the scalp after 4 weeks of RePUVA therapy: Almost total healing of the erosions with scarring alopecia.