Extramedullary hematopoiesis, Thalassemia intermedia, Radiology
A 52-year-old male patient was referred to our outpatient clinic with complaints of cough, hemoptysis (minimal), and chest pain radiating to the back. The patient's smoking history was five packs/year, and he was yet an active smoker. On physical examination, respiratory sounds and other system examinations were normal. In laboratory tests, the hemoglobin level was 6.7 g/dL, platelet was 986000 u/L, leukocyte was 13500 u/L, ferritin was > 2000 ng/ml, sedimentation was 2 mm/h, and C-reactive protein was 0.1 mg/L, and renal and liver function tests were normal. The patient, who underwent intermittent erythrocyte transfusion for 15 years with the diagnosis of thalassemia intermedia, was splenectomized. A paraspinal mass was observed in the chest X-ray and then on the thorax computed tomography (CT) (Figure 1).
Extramedullary hematopoiesis (EMH) is hematopoiesis occurring outside the bone marrow, and it is most commonly seen in the most common hematological disorders such as chronic hemolytic anemia (thalassemia and sickle cell anemia), myelofibrosis, leukemia, lymphoma, congenital dyserythroblastic anemia, immune thrombocytopenic purpura, and infections and advanced-stage cancer. EMH may frequently occur in the spleen, liver, and lymph nodes, as well as in the thymus, heart, breast, prostate, ligaments, kidney, adrenal glands, pleura, retroperitoneum, skin, peripheral and cranial nerves, and spinal cord. Intrathoracic extramedullary hematopoiesis is usually located in the posteroinferior mediastinum, presenting as a bilaterally lobulated mass. Paraspinal EMH constitutes 11-15% of EMH cases, and the male/female ratio is 5/1. Differential diagnosis includes neuroblastoma, PNET/EWING, rhabdomyosarcoma, lymphomas, primary and metastatic malignancy, paravertebral abscess, lateral meningocele, and extrapleural cysts.
More than 80% of EMH is asymptomatic; however, chylothorax, hemothorax (in some cases massive and fatal), pneumothorax, and spinal cord compression are the complications that may occur. While the diagnosis is made in the presence of compatible hematological disease and computed tomography (CT) findings, magnetic resonance imaging (in case of spinal cord compression), 18F-fluoro-3'deoxy-L-thymidine PET/CT, and 99mTc-SC scintigraphy can be performed. Non-invasive methods should be preferred since the masses are of high vascularity [1]. If the diagnosis is controversial or surgical intervention is required for complications, a biopsy should be resorted considered. Bronchoscopy, transbronchial biopsy, transthoracic biopsy, mediastinoscopy, video-assisted thoracoscopic surgery, mediastinoscopy, and thoracotomy can be performed for biopsy. Generally, no treatment is needed [2], but low-dose radiation, blood transfusion, surgery, corticosteroid, and hydroxyurea are among the treatment options if there are complications. In the presence of spinal cord compression, pleural effusion, massive hemothorax, dyspnea, lung interstitium involvement, the mass or effusion can be reduced with low-dose radiation [2]. Rarely, EMH may occur entirely in the lung parenchyma and appear as scattered nodules on a CT scan. Pulmonary EMH can cause dyspnea, chest pain, hemoptysis, respiratory failure, and pulmonary hypertension; therefore, low-dose radiotherapy may be required [3].
EMH should be considered before attempting diagnostic interventions in lung masses in patients with hematological disorders, especially thalassemia, and should be thoroughly investigated by imaging methods.
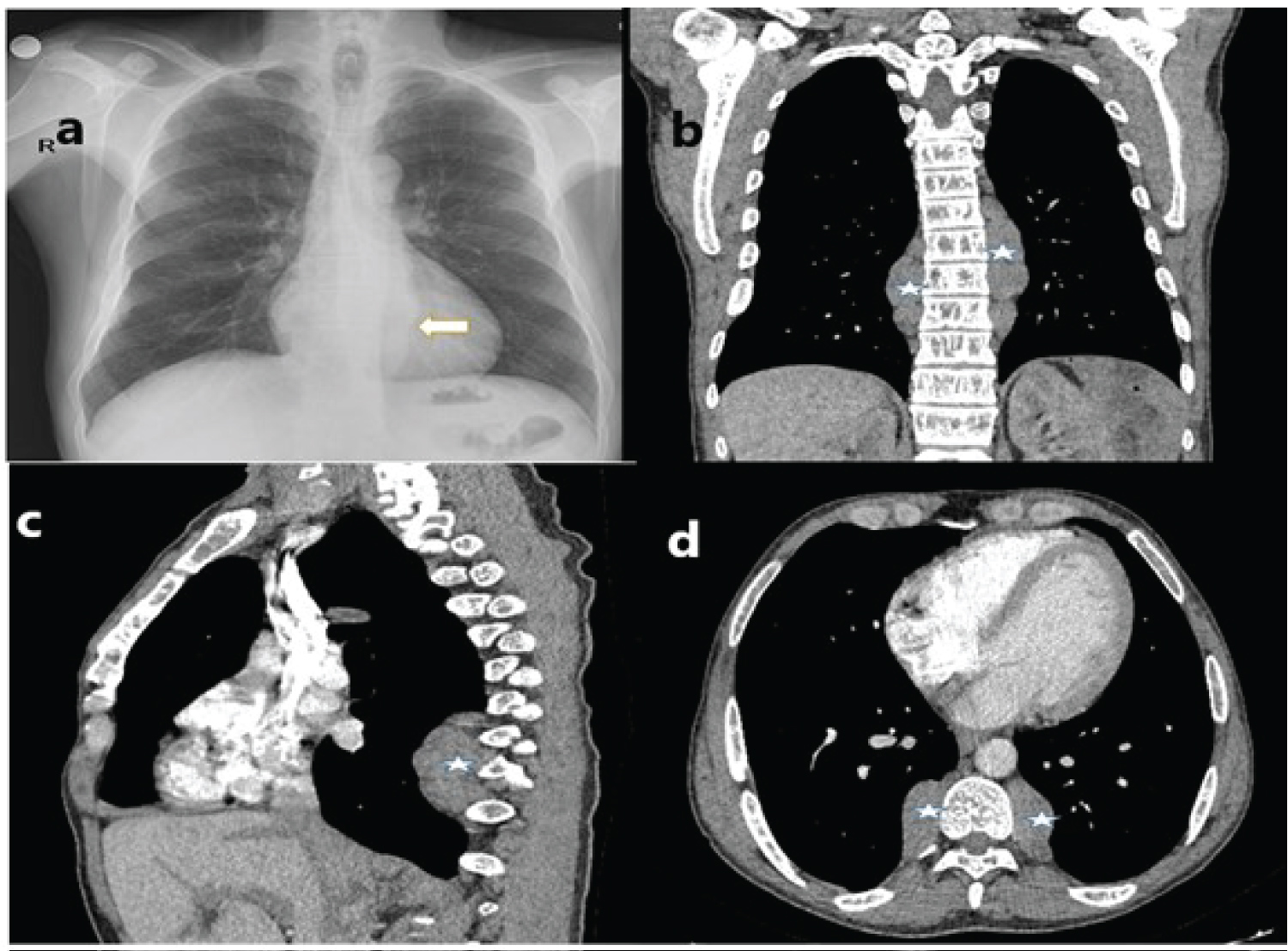
Figure 1: Radiological imaging findings (a) Increased paravertebral density marked by an arrow on chest X-ray; (b) A paraspinal mass marked by an asterisk is observed in the coronal section of the thorax CT; (c) In sagittal section; (d) In the axial section.