An ulcer is defined as a breach in the continuity of the skin or a mucous membrane with molecular death of the cells due to underlying inflammation. Figure 1 depicts the different parts of an ulcer. The article describes four different types of ulcers of the lower limb commonly encountered in the surgical wards, with their major characteristics and markers of identification.
There are certain distinct features to identify the trophic ulcer in Figure 2 on visual inspection. The location of the ulcer is the heel of the foot which is an area under immense stress of body weight and is regularly exposed to traumatic insults when the patient is ambulatory resulting in development of an ulcer, if associated with reduced sensation. This could be due to a neurological problem and/or decreased perfusion consequent to vascular insufficiency. The margins of this ulcer are 'punched out' implying that they meet the edge of the ulcer at near right angles. The surrounding skin shows some roughness that can be appreciated visually. This indicates callous tissue and is a step in the progression towards ulcer, as callous lesions overtime enlarge and eventually ulcerate (either because of trauma or infection). The floor of the ulcer in this case appears clean because of surgical debridement of the wound. Classically, the ulcer floor is covered with slough. On examination, loss of sensation was elicited at the site of ulcer, confirming the diagnosis of a trophic ulcer. This type of ulcer can be seen in diseases which reduce peripheral cutaneous sensations such as spinal or peripheral nerve injury, diabetic neuropathy, tabes dorsalis, transverse myelitis or meningomyelocele.
The patient was a known case of Type 2 Diabetes Mellitus since 5 years, but was not compliant with the treatment for the same. This patient developed a diabetic foot ulcer secondary to vascular insufficiency. The ulcer's location on the dorsum of the foot is quite classical for diabetic ulcers. The base of the ulcer is covered with granulation tissue and has slopping margins. In addition to that, the ulcer has penetrated deep enough to expose the tendon on the dorsum. The surrounding areas show blackened skin as a result of gangrene. All these signs are consistent with and are quite typical of a diabetic ulcer. The absence of the digits of the foot suggest that they might have been amputated because of concurrent diabetic neuropathy as the patient also shows decreased sensations at both feet (Figure 3).
A lymphedematous leg can develop multiple ulcers of varying sizes. These generally have irregular shapes and margins. Additionally, the ulcer margins are steep while the base of the ulcer is covered with slough. The leg on inspection appears edematous. This also leads to some degree of inadequate perfusion. In this case, the lymphedema is complicated with papillomatosis and hyperkeratosis, which predisposes to infection and eventually leads to ulcer formation (Figure 4).
The patient presented to Emergency Medicine after suffering an accidental burn injury to the lower limb. This is a case of fourth degree burn ulcer on the dorsum of foot. It can be identified due to the presence of certain characteristic features. For instance, there is white charred skin on the ulcer floor. The ulcer has penetrated deep enough to expose the tendons on the dorsum of foot. Along with that, some part of bone is also visible on the ulcer floor. These features point towards a fourth degree burn. The surrounding skin shows dark pigmented burn marks. In some areas, the epidermis has burnt off to reveal the dermal part (seen on the toes) (Figure 5).
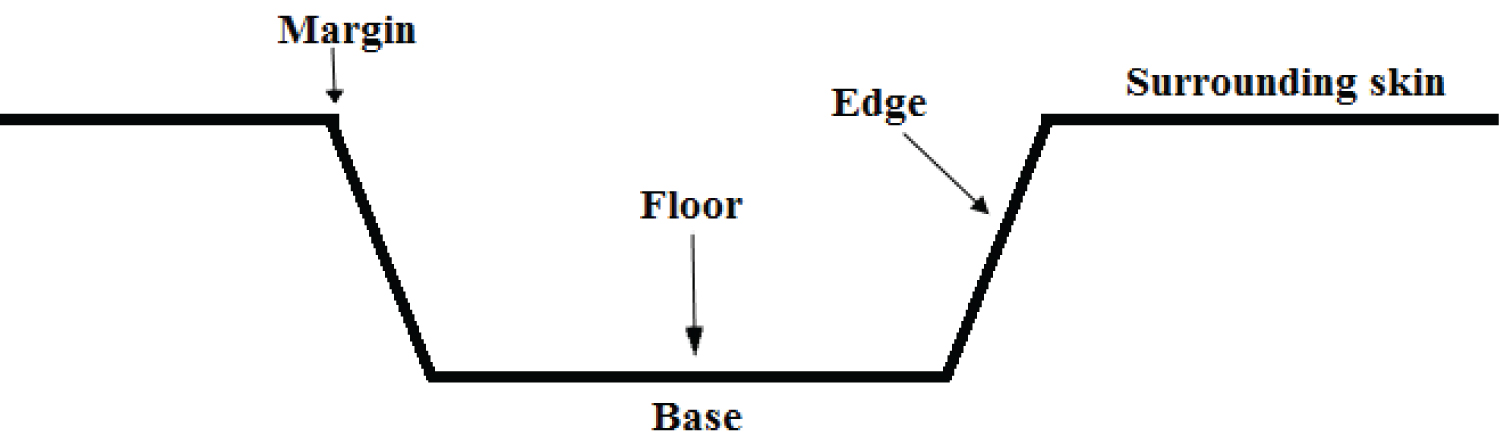
Figure 1: Different parts of a cutaneous ulcer.
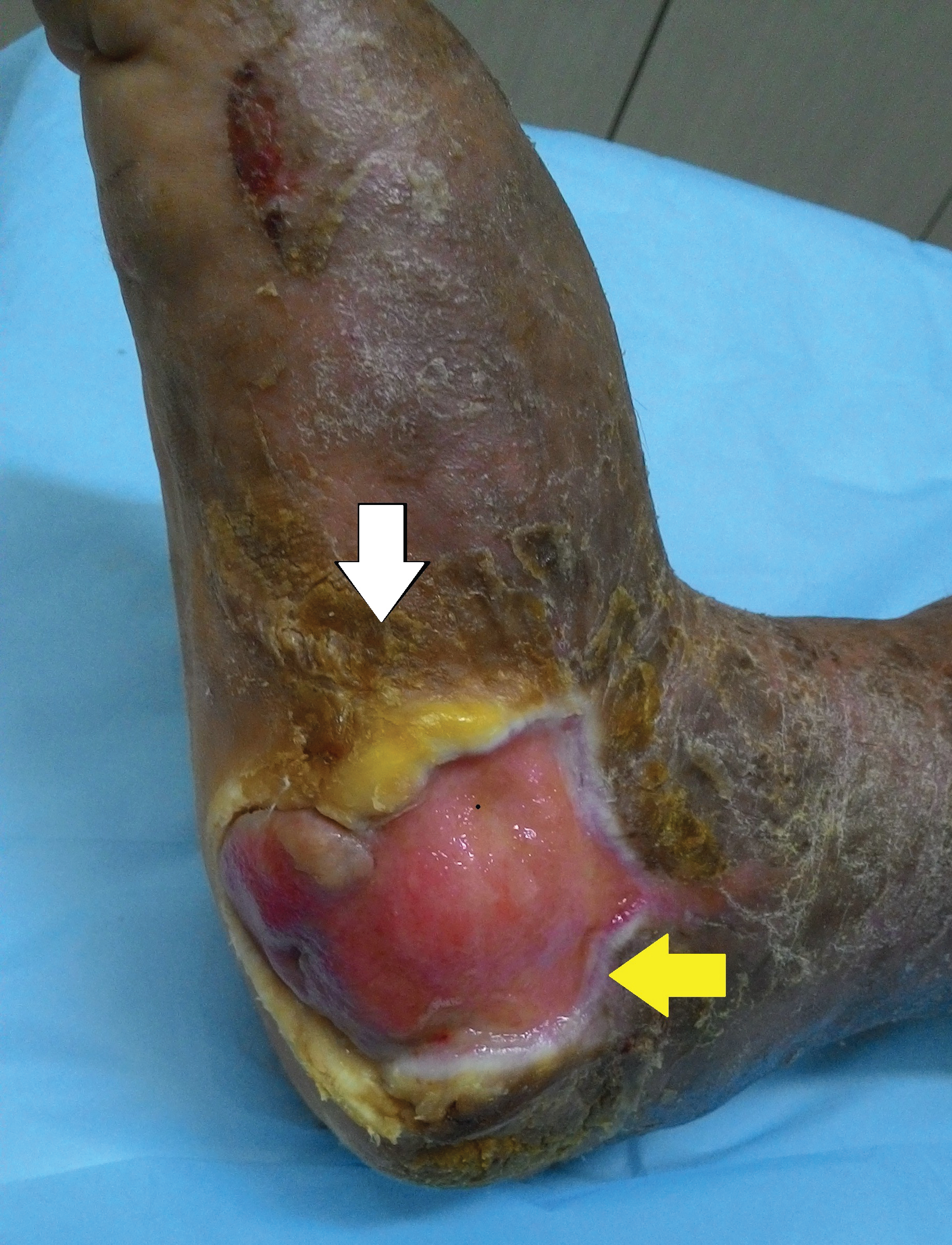
Figure 2: The ulcer shows punched out margins (yellow arrow) and callous tissue (white arrow).

Figure 3: The ulcer shows lots of granulation tissue with an exposed tendon (yellow arrow) and adjacent dark pigmented gangrenous areas (white arrow).

Figure 4: Two ulcers on the leg of the patient can be seen. Sloughing material can be observed on the floor. One of the ulcers has punched out margins (white arrow) while the other ulcer has irregular shape and margins, along which papillomatosis and hyperkeratosis can be observed. Pedal edema can be appreciated in the figure.
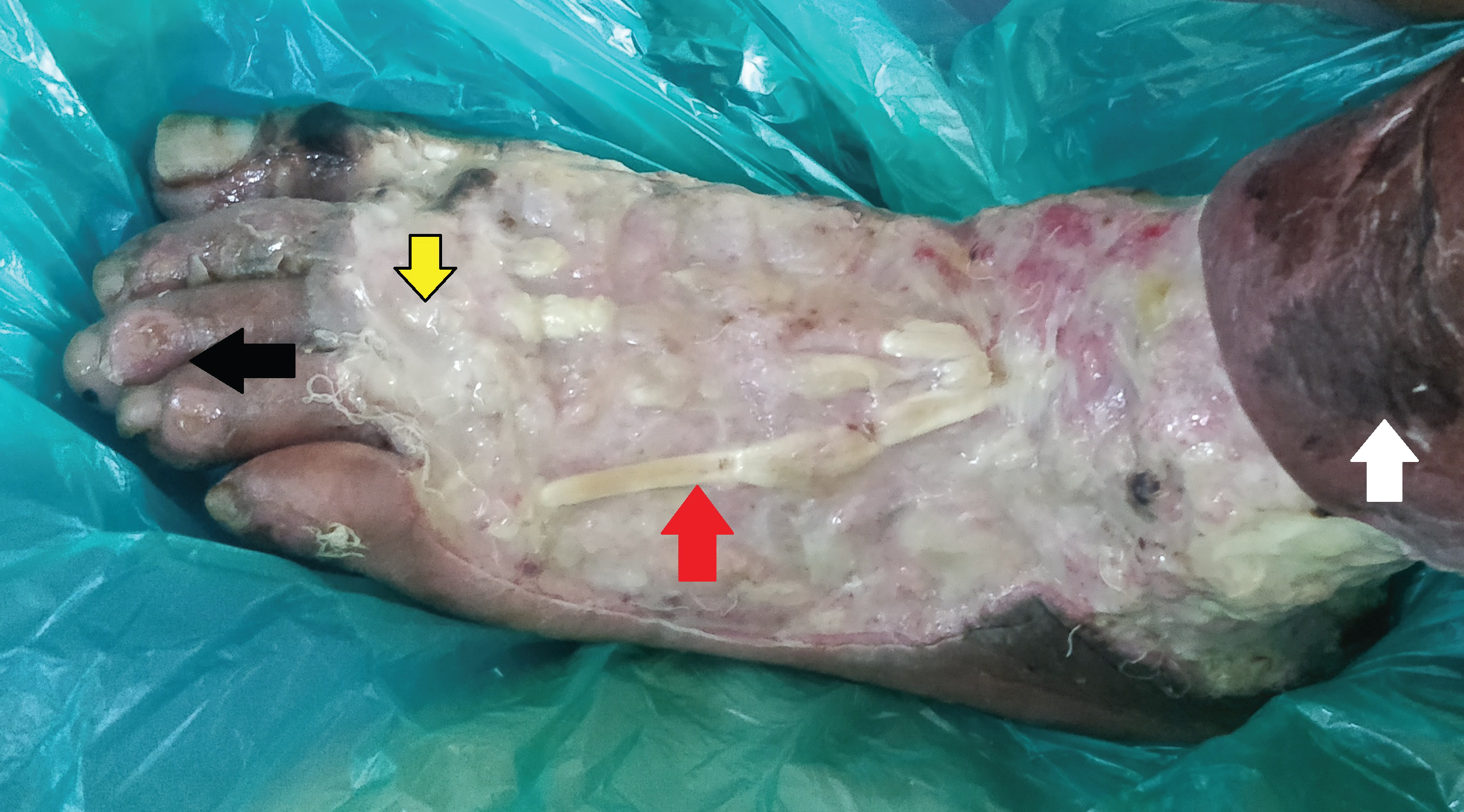
Figure 5: A large ulcer with white charred skin (yellow arrow) and exposed tendons (red arrow) can be seen. Surrounding areas show blackish burnt skin (white arrow) as well as exposed dermis (black arrow).