We report the case of a male preterm at 27 weeks of gestational age, born by emergency cesarean section with 1195 g, of an untreated HIV-infected mother, with an unsupervised pregnancy. After immediate resuscitation, he was admitted to the neonatal intensive care unit (NICU). He was started on standard neonatal antiretroviral HIV prophylaxis and completed seven days of ampicillin and gentamicin. Due to Staphylococcus epidermidis late sepsis, he completed 21 days of cefotaxime and vancomycin, but on day 14 of antibiotics, there was clinical and analytical worsening. Candida albicans was isolated in blood and cerebrospinal fluid cultures. Brain imaging identified several microabscesses which evolved to microcalcifications, as shown in Figure 1 and Figure 2. The patient completed six weeks of amphotericin B with clinical improvement. A multidisciplinary approach and follow-up including electroencephalogram, echocardiogram, abdominal and renal ultrasound, and ophthalmological exam were unremarkable, and HIV antibody tests were negative at 18 months of age.
Candida spp. is a relevant cause of neonatal infection, especially in very low birth weight (VLBW) infants, with significant morbidity and mortality [1,2]. The most frequent complication from hematogenous spread of candidiasis to the central nervous system is meningitis, while brain abscesses are uncommon [1].
Facing late-onset neonatal sepsis, particularly in VLBW neonates without antifungal prophylaxis, it's crucial to recognize an invasive Candida as a possible cause of infection while timely adjusting antimicrobic therapy. Another risk factor for a Candida infection was the possibility of a vertical transmission HIV infection but ruled out afterward.
We highlight the importance of sequential cranial ultrasounds for diagnosing and following preterm neonates [3]. Also, brain magnetic resonance imaging is required, especially when central nervous system complications are present, as reported in this case.
A multidisciplinary approach and long-term follow-up are required to evaluate possible neurological sequelae [3].
None declared.
The authors declare no conflict of interest.
All authors have given their input and approved the final manuscript.
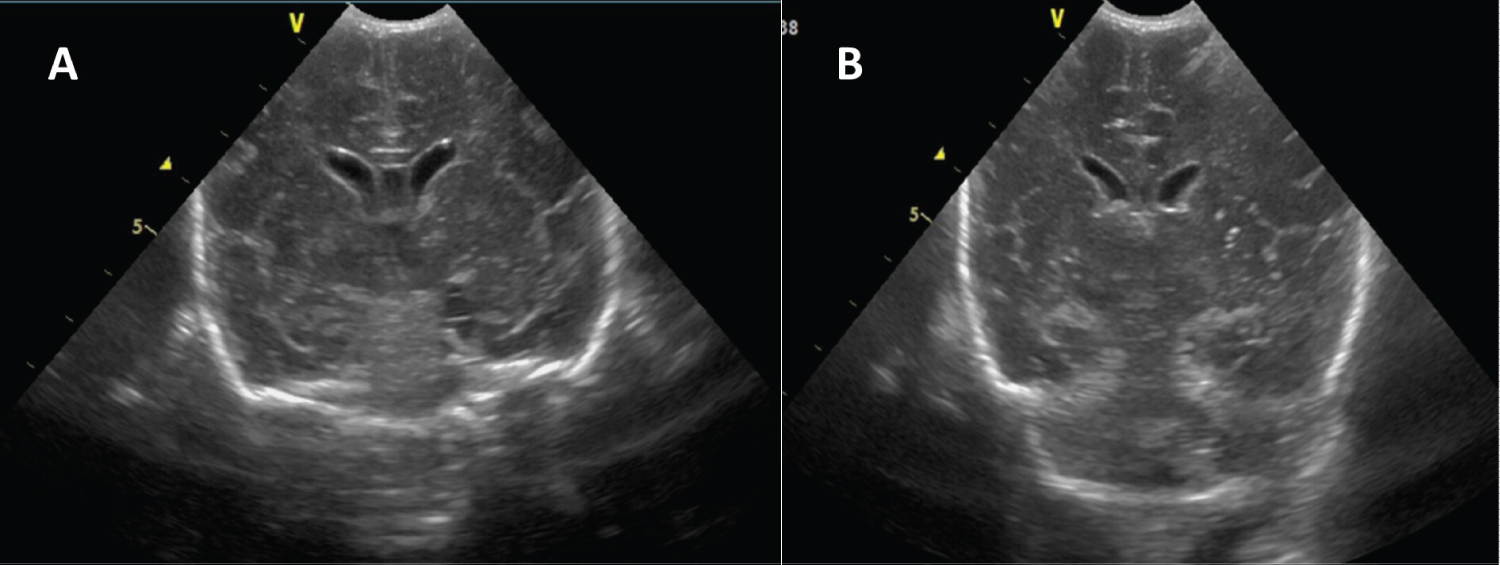
Figure 1: Coronal view of neonatal transfontanellar ultrasound- multiple echogenic frontoparietal and basal ganglia lesions (A) which progressed to microcalcifications after 2 weeks (B).
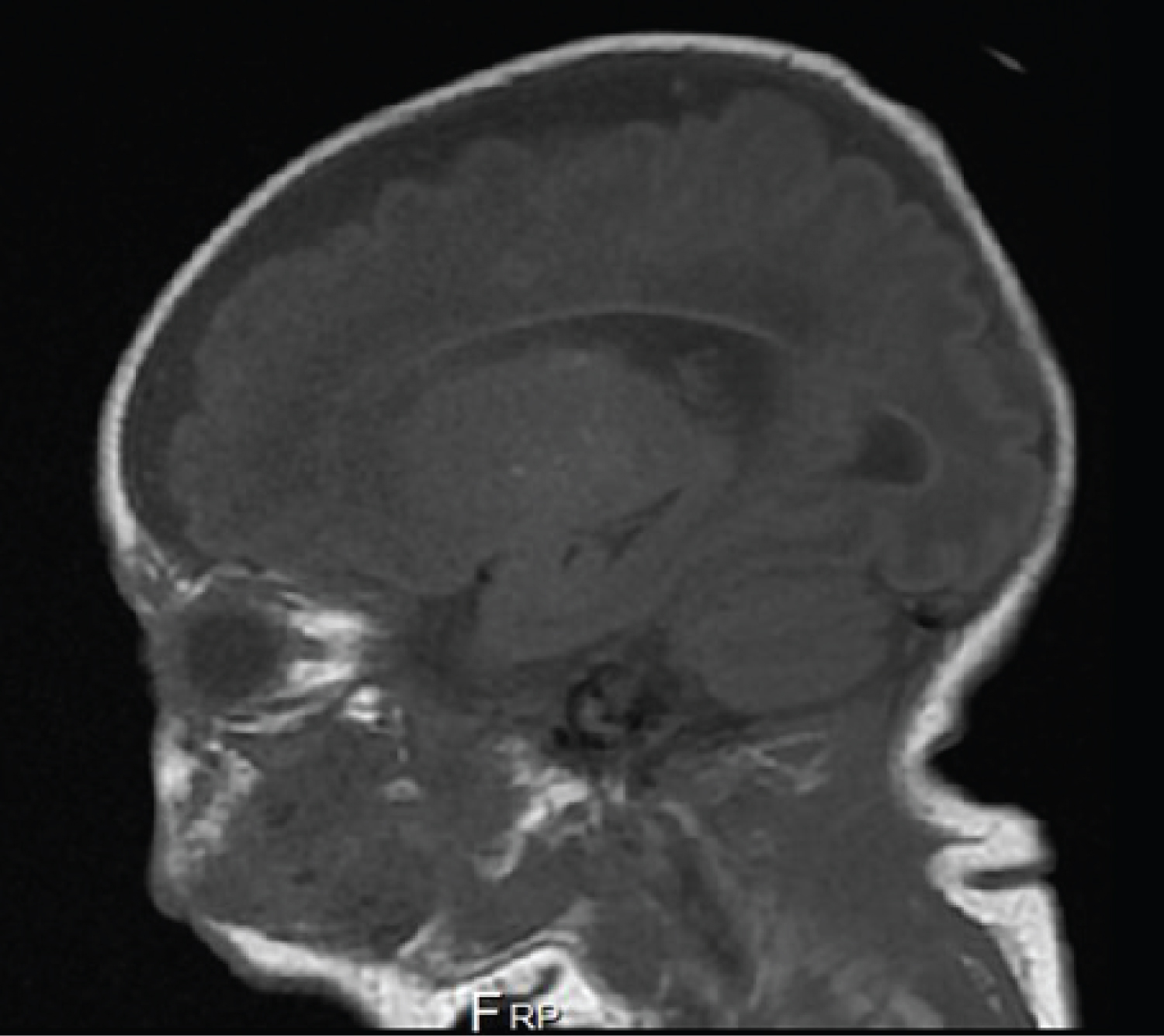
Figure 2: Brain magnetic resonance T1 sagittal image after 4 weeks of amphotericin B - multiple rounded and punctate infectious lesions in different stages of evolution, mainly in periventricular white matter.