The patient was a 15-year-old man with no known medical History. He had also no surgical history. He presented to the general surgery clinic with a history of a mass measuring 10*7 cm on the left side of lower abdomen above the iliac crest. It was neither growing nor painful. Examination revealed a soft, compressible, non pulsatile mass with indistinct borders on the left flank (Figure 1). Ultrasound (US) sonography of the soft tissue showed a large solid lesion measuring approximately 10 × 8 cm in the anterior abdominal wall on the left side. This mass was intramuscular between the abdominal wall muscles. Abdominal tomography showed diffuse lesion of 10*8cm in the left iliac region along right lateral abdominal wall and involving anterior abdominal wall muscles with no abdominal extension (Figure 2).
Abdominal MRI with contrast (Figure 3) showed a large intramuscular mass in the right anterior abdominal wall with presence of internal linear and nodular high T2 components.
A well-differentiated liposarcomas was suspected rather than lipomas. The patient was informed of the results, and consent for surgery was obtained. Surgery was undergone under general anesthesia. We observed a lateral bulge on the right side of the abdominal wall. We decided to perform an oblique flank incision because the medial extension was only to the medial border of the rectus muscle. A 10-cm incision was made. A left thoraco-abdominal parietectomy removing the entire angioma and the 2 lower sides was done. Coverage was made with a pedicles rectus abdominis flap on the upper epigastric vx (prepared by ligation of the lower epigastric pedicle-4 weeks before). A bifacial prosthesis was placed under the flap. The specimen was retrieved and addressed for histopathological examination.
A drain was inserted. Postoperative period was uneventful. Sutures were removed on 10th day and patient went home with no complications. Follow up after 3 months revealed no recurrence. Histopathology proved the diagnosis of intra muscular haemangioma.
Intramuscular hemangiomas were first reported by Liston in 1843 [1]. They are rare tumors comprising less than 1% of all vascular malformations [2-4]. The most common sites are the limbs, followed by the head and neck. The abdominal wall muscle is the rarest site for intramuscular hemangiomas. Because of its rarity, more than 90% of intramuscular hemangiomas are misdiagnosed [5].
Magnetic resonance imaging (MRI) is more specific in evaluating the lesion and its extension. It is better than computed tomography (CT). Tumor histopathology reveals blood vessels in addition to various amounts of fibro fatty tissue, smooth muscle and thrombus. Complete excision provides good results [6]. Partial excision results in high recurrence rate. The defect in abdominal wall created by wide local excision can be covered by prosthesis.
None
No conflict of interest.
The author confirms sole responsibility for the following: study conception and design, data collection, analysis and interpretation of results, and manuscript preparation.
Written consent has been obtained from the patient.
The data supporting the findings of this study are available from the corresponding author upon reasonable request.

Figure 1: Pre-operative picture showing the abdominal wall haemangioma
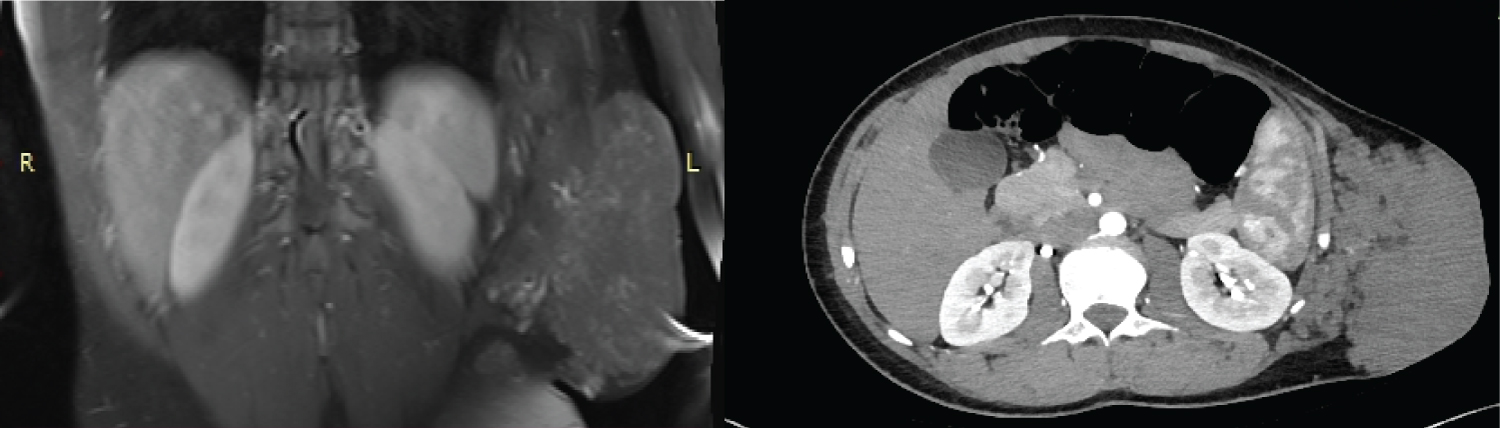
Figure 2: 2A: Magnetic resonance imaging of the abdomen showing a large intramuscular mass in the left anterior abdominal wall
2B: Computed tomography showing a large echogenic solid lesion in the anterior abdominal wall on the right side between the abdominal wall muscles measuring approximately 10 × 8 × 2.4 cm
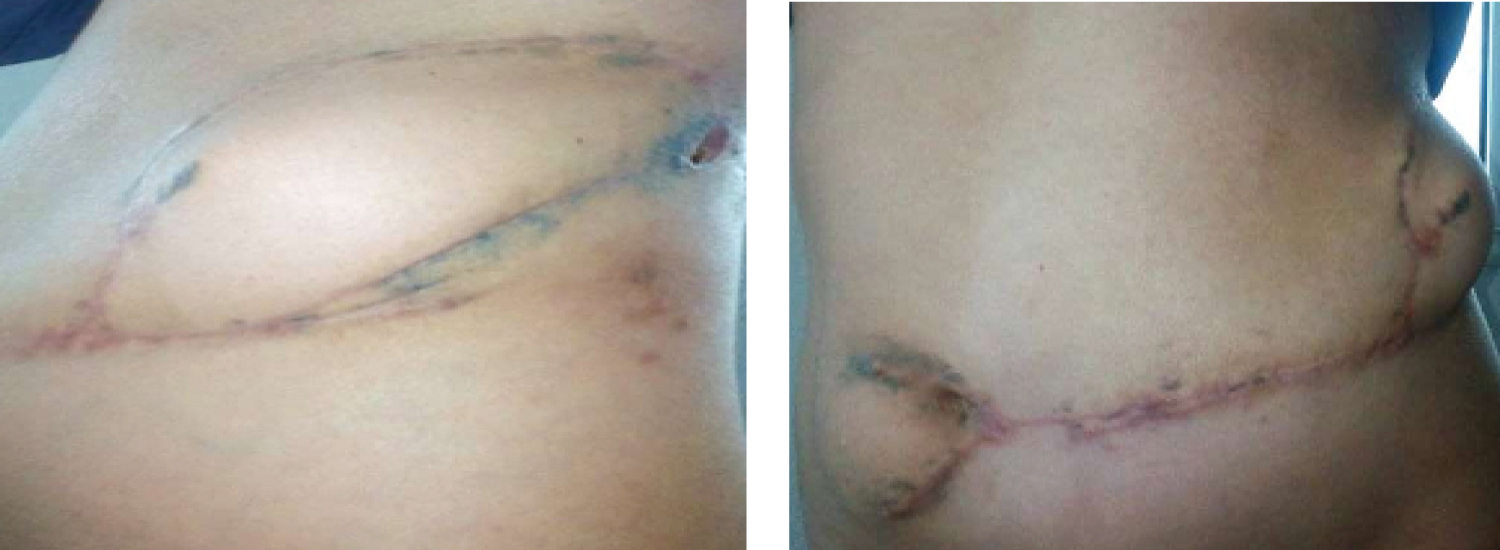
Figure 3: Post-operative picture