A 38-year-old female with a history of pancreatitis presented with breathing difficulties and tested positive for COVID-19. A CT of her chest, abdomen and pelvis with contrast showed a 8.5 × 13.1 × 25.4 cm (AP × ML × CC) multilobulated abdominal cyst extending into the posterior mediastinum with bilateral pleural effusion (Figure 1A). CT scan MipPR reconstruction showed the relation of the pseudocyst with abdominal and thoracic vessels (Figure 1B). Magnetic resonance cholangiopancreatography (MRCP) showed communication between the pseudocyst and the main pancreatic duct (Figure 1C). Esophagogastroduodenoscopy (EGD) with EUS confirmed a pancreatic pseudocyst through elevated amylase levels, and subsequent cystogastrostomy and cystoduodenostomy reduced the cyst [1]. A pancreatic pseudocyst is a complication of acute and chronic pancreatitis in which pancreatic secretions are found enclosed in a fibrous membrane [2]. While management of the patient was complicated by COVID-19 as a comorbidity, the pseudocyst was successfully treated through an endoscopic approach.
None of the authors have anything to disclose and have no conflict of interest. This research did not receive any specific funding or grant from agencies in the public, commercial, or not-for-profit sectors.
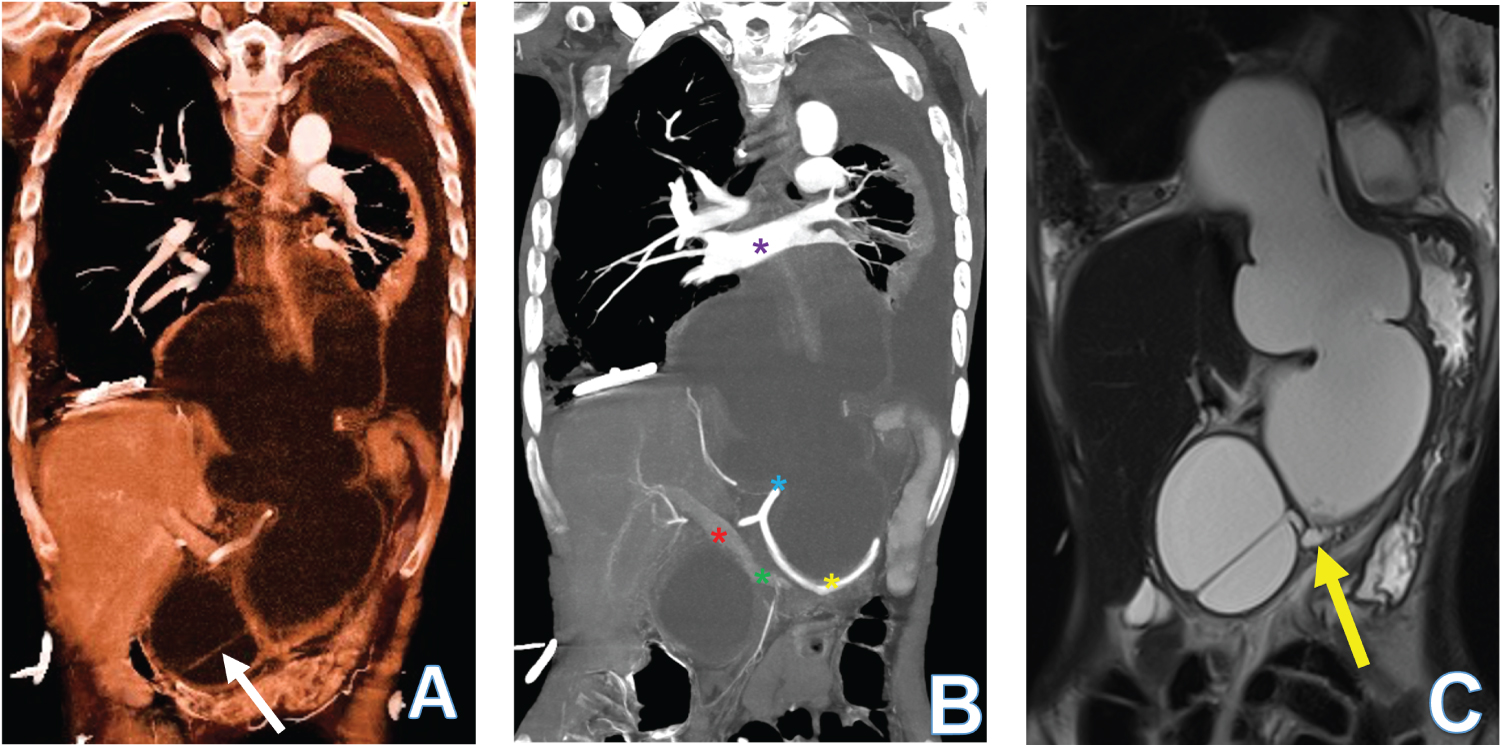
Figure 1: 38-year-old woman presenting with COVID-19 and a large pancreatic pseudocyst. (A) 3D reconstruction volume rendering using CT abdomen liquid algorithm shows a large, encysted fluid collection with septation. The epicenter is in the abdomen and extends into the posterior mediastinum primarily behind the left lung and bronchial tree. The pancreas is not seen separately; (B) CT scan 3D reconstruction using MipPR shows the relation of the pseudocyst with the celiac trunk (blue star), splenic artery (yellow star), main portal vein (red star), splenic vein (green star) and the pulmonary veins (purple star); (C) The MRCP study HASTE coronal image shows communication between the large cyst and the main pancreatic duct (yellow arrow).