A 38-year-old man with past medical history of epilepsy presented to the emergency room complaining of 1 day of abdominal pain without nausea or vomiting. He had similar symptoms 4 months ago that resolved spontaneously.
He denied previous alcohol or tobacco use, and his serum alpha fetoprotein level was normal at 3.8 ng/mL. Computed tomography (CT) imaging of his abdomen and pelvis demonstrated a 10.4 cm mass in the right liver with heterogeneous areas of mixed high and low attenuation (Figure 1A).
Core needle biopsy demonstrated numerous dyshesive malignant cells with enlarged nuclei, prominent nucleoli, and oncocytic cytoplasm with intracytoplasmic lumens and granules.
He underwent right hepatectomy and pathological examination demonstrated a solitary 10.5 × 10.1 × 7.0 cm fibrolamellar hepatocellular carcinoma with negative margins (Figure 1B and Figure 1C).
He recovered uneventfully and was doing well at his follow-up appointment 1 week after discharge.
None of the authors have any conflicts of interest to disclose.
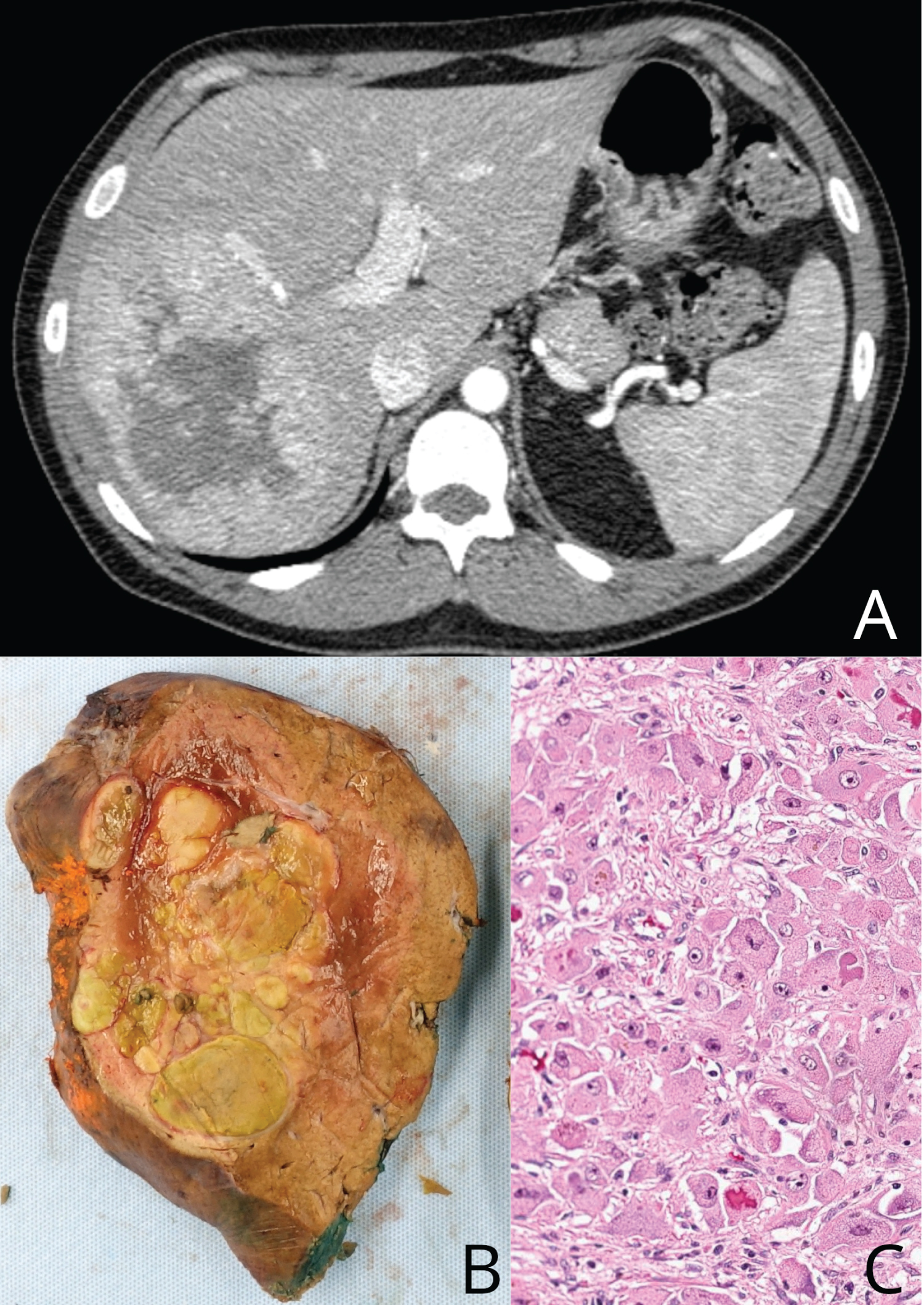
Figure 1: Liver cancer. (A) Computed tomography (CT) imaging of his abdomen and pelvis demonstrated a 10.4 cm mass in the right liver with heterogeneous areas of mixed high and low attenuation (Panel A); (B and C) Right hepatectomy and pathological examination demonstrated a solitary 10.5 × 10.1 × 7.0 cm fibrolamellar hepatocellular carcinoma with negative margins (Panel B, Panel C).