Uterine adenomyosis is a disorder in which endometrial glands and stroma are present within the myometrium, resulting in hypertrophy of the surrounding myometrium [1,2]. Its exact epidemiology is uncertain as data regarding this condition has often relied on the assessment of the uterus following hysterectomy. However, studies have reported that it seems to be present in a wide range of individuals undergoing hysterectomy (9-62%) [3].
It was previously described as a disease that developed in women in their 40-50s; nevertheless, studies using imaging diagnosis of adenomyosis suggest that it can frequently be detected at younger ages (with a reported prevalence of 20-35%) [4-6].
Patients will often present with uterine enlargement, painful menses, abnormal uterine bleeding (AUB) and chronic pelvic pain.
Adenomyosis often coexists with other uterine disorders, such as uterine leiomyoma and/or endometriosis, which can obscure its diagnosis.
We present a case of a 30-year-old patient who entered the emergency department complaining of an exuberant edema in the left lower limb with one week of evolution and no other associated symptoms.
She was healthy with no usual medication. The patient haven´t undergone any surgery and had no known drug allergies. Menarche at the age of 11; she denied any previous sexual intercourse. She reported regular and prolonged menses.
The initial clinical suspicion was that the signs and symptoms corresponded to a case of deep vein thrombosis of the lower limb. However, on physical examination, the patient was pale and on abdominal palpation, it was possible to denote a huge mass that occupied the whole abdomen and extended to the xiphoid process.
On the laboratory evaluation, she had serious anemia (Hemoglobin level of 4.6 g/dL), with no other major changes. To better characterize this mass, an abdominopelvic computed tomography (CT) was requested, which showed the existence of a large mass (with 17 * 28 cm of maximum diameters) with an apparent uterine origin - admitting possible leiomyomatous/sarcomatous lesion (Figure 1 and Figure 2). Lactic dehydrogenase and other tumor markers were all negative.
The patient was transfused with a total of 5 units of red blood cells in preparation for elective surgery. She was posteriorly submitted to an exploratory laparotomy.
Figure 3, Figure 4 and Figure 5 show the aspect of the patient´s uterus, which weighted a total of 2900 grams. Given the size of the uterus, we decided to perform a total hysterectomy with bilateral salpingectomy. The postoperative period was uneventful.
The histological result of the surgical specimen confirmed the presence of adenomyosis and uterine leiomyomas.
With this clinical case portrait, the authors propose to highlight the importance of approaching the patient as a whole; furthermore, it is also intended to warn that adenomyosis can affect young patients and have an important impact, which can result in significant uterus´ growth.
The authors declare that they have no conflict of interest regarding the publication of this case report.
No funding from an external source supported the publication of this case report.
All authors equally contributed to the execution of this paper.
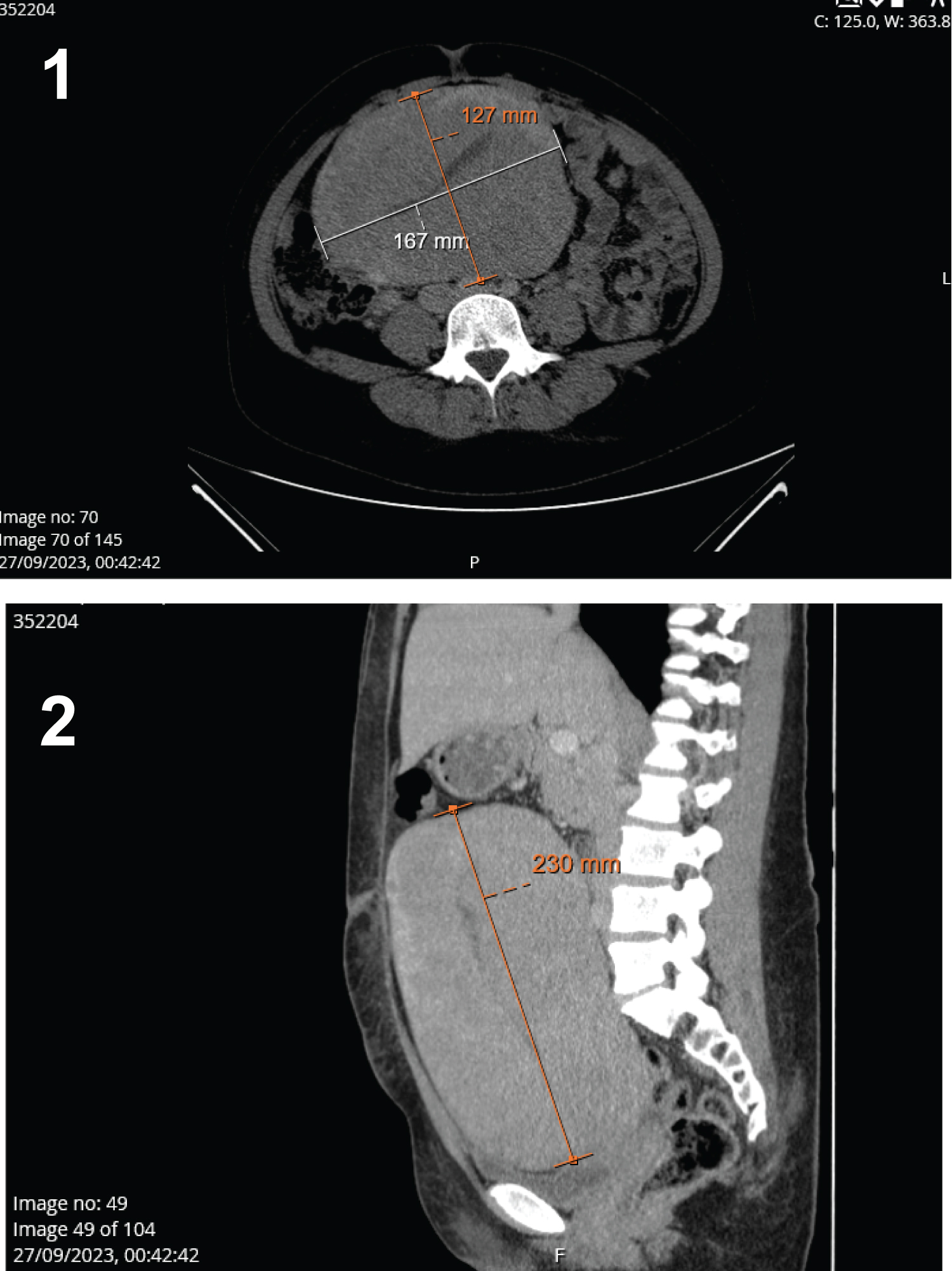
Figure 1 and 2: CT scan showing the enlarged uterus (with measures of its diameters).
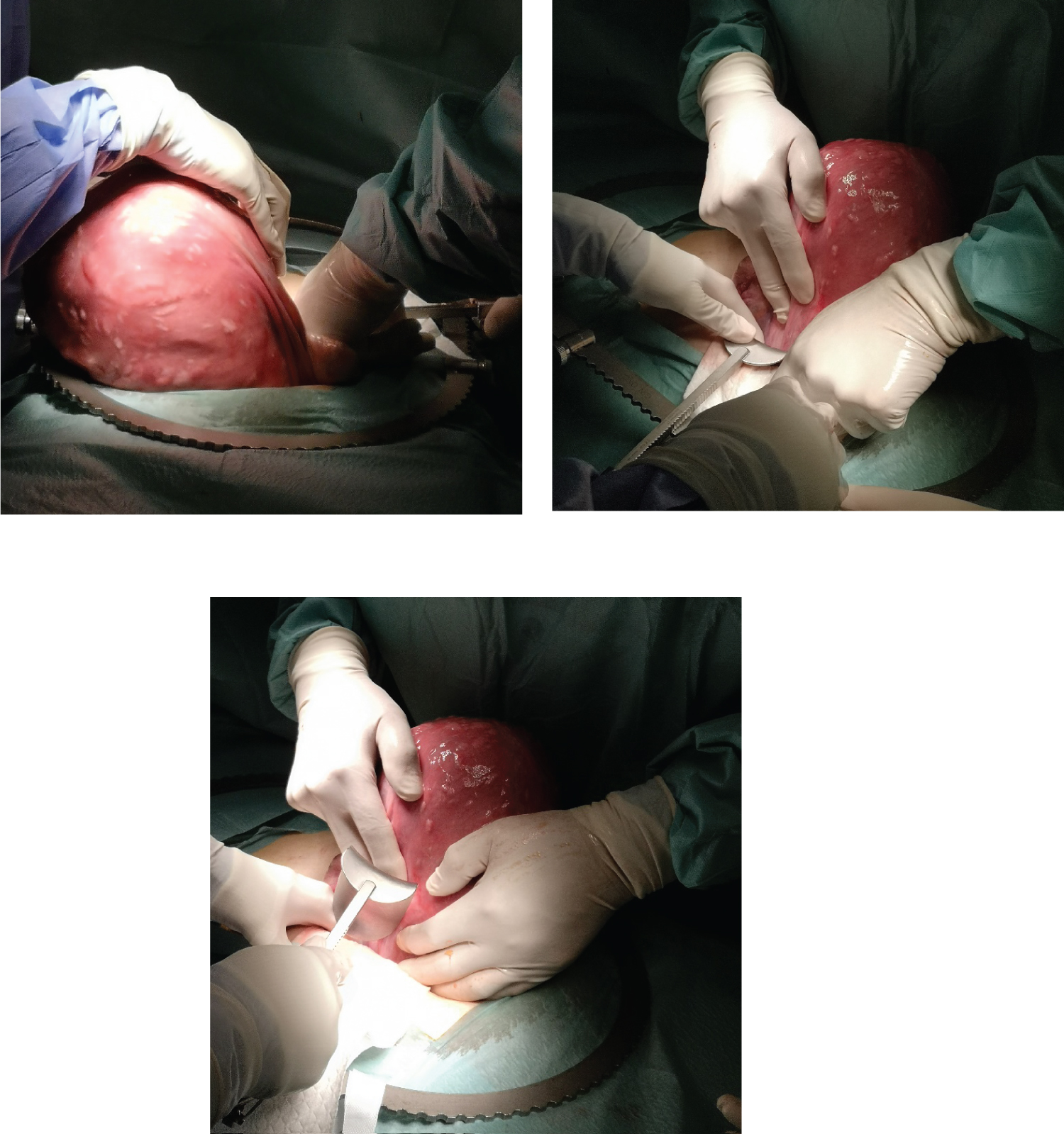
Figure 3-5: Corresponding images of intraoperative findings.