The blunt laryngotracheal traumatism can be frequently ignored by the patient itself due to the scarcity of symptoms related to this form of injury within the first hours. The importance of the damage can be not proportional to the rarity of clinical signs. In this article we are about to present a serious form of laryngeal damage in a patient with no vital signs.
Laryngeal, Traumatism, Fracture, Tracheotomy
Laryngeal fracture is not a frequent type of injury. It could present some serious and severe complications which are unpredictable within the first hours after traumatism. The management is time dependent and needs close supervision of the patient whose prognosis can change at any time.
This paper is about to describe clinical and laryngeal damages through a case of a young man who suffered from a blunt laryngeal traumatism.
It's a 28-year-old victim of neck traumatism, an anterior cervical impact that causes within the 24 hours after the injury a painful dysphonia. The patient was presented to the ENT emergency where CT-Scan was made. It shows a laryngeal fracture: Thyroid cartilage, associated to cervical emphysema (Figure 1).
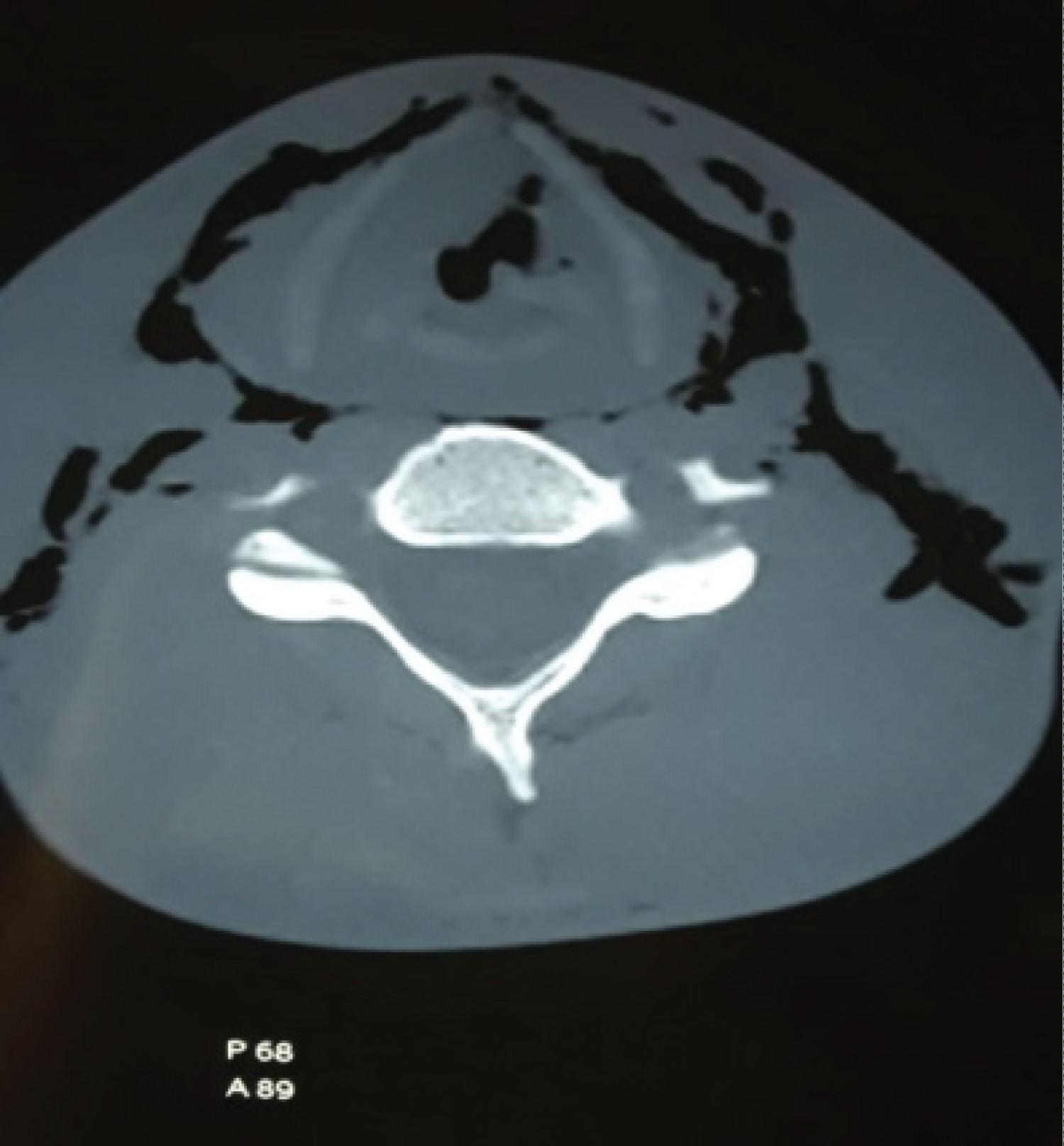 Figure 1: Cervical emphysema associated to a laryngeal fracture.
View Figure 1
Figure 1: Cervical emphysema associated to a laryngeal fracture.
View Figure 1
The endoscopic examination shows a reduction in mobility of the left arytenoid and tumefaction of the left ventricle.
The patient went under surgery. A primitive tracheotomy was done then an anterior cervicotomy in a goal to explore the laryngeal cartilages: thyroid and cricoids cartilages. During the operative procedure we noticed a large fracture in the thyroid cartilage that we have stabilized and sutured (Figure 2). We have done a padding using under-hyoid muscles.
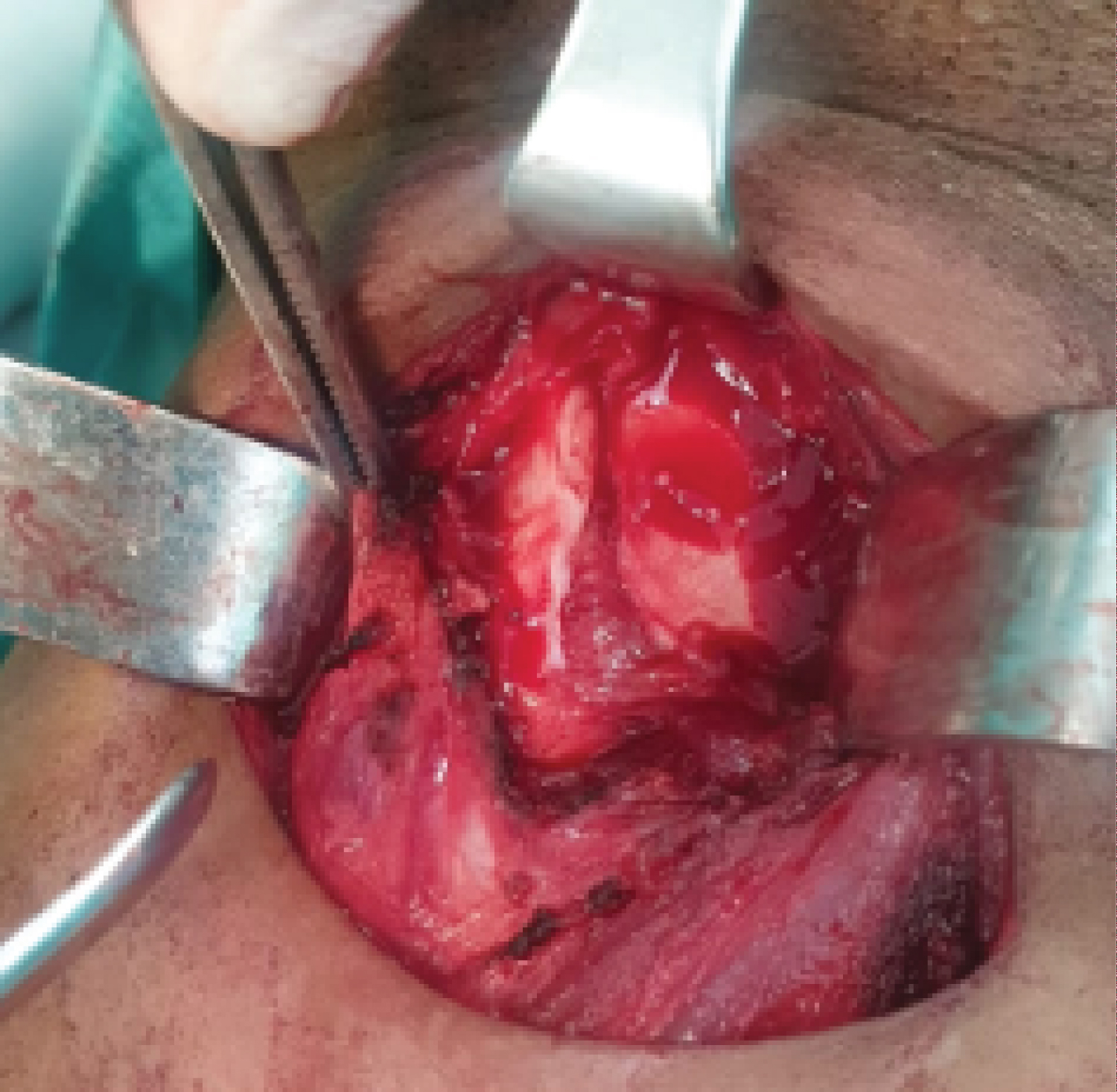 Figure 2: Displaced fracture of cartilage thyroid of the larynx.
View Figure 2
Figure 2: Displaced fracture of cartilage thyroid of the larynx.
View Figure 2
The tracheotomy canula was removed on the fifth day after surgery and the patient had been under inhaled and systemic corticotherapy for 1 month.
Four months after the surgery, the patient presented an aggravation of his dysphonia. The endoscopic exam revealed a polyp of the anterior commissure, and then the inhalated corticosteroids were given for 2 months. Two weeks later, the patient came with the polyp in hand; he spit it out during a cough.
Actually, we are at about 1 year after surgery, with some rehabilitation sessions, the patient still got a dysphonia, but it doesn't disturb him in communicating or practicing any physical activity.
The laryngeal fracture is not a common injury. Due to the important flexibility of the larynx and especially its protecting structures such as the mandible and sternum [1]. That makes the larynx protected from direct mechanisms of traumatism. Despite all of this, laryngeal traumatism can lead to severe complications if not treated within the first hours after the injury. It's related to the increasing use of motor vehicles and violent sports [1].
We understand through that, that a high proportion of men are exposed to this kind of traumatism. Adult men also present some characteristics in their cartilage structure which is ossified and can fracture easily comparing to young people or children [2]. Another risk factor of laryngeal fracture has been reported is a lower socioeconomic status [3].
The most important fact in the management of laryngeal traumatism is time. The better outcome occurred according to patients who were treated earlier compared to those who received delayed treatment [4].
Quick management can prevent complications. Asphyxia can occur due to the instability of cartilage fragments for example or due to a hematoma and can lead to death if not threatened within the first hours. Their also chronic complications according to the trauma, such as hoarseness, stenosis, or recurrent granulation formation [4] such as what occurred to our patient, but luckily, he spit it out spontaneously during a cough effort. The tracheotomy can be one of the solutions to avoid acute complications. In a recent study, about 564 cases of laryngeal trauma were analyzed (Mendelsohn, et al.) and it was recommended to go for a tracheotomy within the first 24 hours after the trauma in a goal to secure airways [5].
The surgical treatment consists of repairing the lesions. In displaced and instable fractures, it's recommended to explore the laryngeal cartilages and do the reparations required; a thyrothomy can be needed in some cases [1].
Laryngeal trauma should not be misdiagnosed, and we must be aware of the acute and chronic complications. Early management will for sure avoid serious damage.