Introduction: An aggressive non-Hodgkin lymphoma, with subtype of diffuse large B-cell lymphoma (DLBCL) is most frequent lymphoid malignancy in this category, especially in the tonsillar region. However, despite the numerous clinical series available, there is a lack of clear clinicopathological and immunohistochemical characteristics available due to diverse patterns seen in this tumour. So, more directed approach is needed for the treatment which is presented with the case review in the following study.
Material and method: A 39-year-old male patient reported to the department with a complaint of swelling on left side of the neck in the past 5 months. Clinical, radiographic, histopathological as well as immunohistochemical were conducted to reach the diagnosis.
Result: The lesion was diagnosed histopathologically as DLBCL, with immunoreactivity for LCA, CD20, and BCL6 and negative for BCL2, CD3 CD10, and MUM1.
Conclusion: A more directed approach is needed to improve the quality of treatment and life expectancy in patients diagnosed with such lesions.
Non-Hodgkins lymphoma, Waldeyer ring, Diffuse large B-cell lymphoma
Malignant neoplasms that affect the lymphatic system are called lymphomas and include a wide range of diseases that originate from B cells. Lukes defined malignant lymphoma as “a neoplastic proliferative process of the lymphopoietic portion of the reticuloendothelial system, that involves cells of either the lymphocytic or histiocytic series in varying degrees of differentiation, that occurs in an essentially homogeneous population of a single cell type” [1]. Lymphoma can be broadly classified as Hodgkin Lymphoma (HL) and non-Hodgkin Lymphoma (NHL) [2]. NHLs are a heterogeneous group of lymphoproliferative malignancies that are much less predictable than HL and have a far greater predilection to disseminate to extra-nodal tissues. Nearly 25% of cases arise in extra-nodal locations and the majority of them may be observed in both sites [3].
NHL of primary extra-nodal type involving the oral cavity as well as oropharynx amounts to 13% with almost 70% fraction occurring in the tonsils. The most common high-grade rapidly growing NHL is considered to be diffuse large B-cell lymphoma (DLBCL), reaching about 80% in some of the studies [4]. A comprehensive review of the literature is necessary due to the significantly varying clinicopathological features of DLBCL tumours, despite the fact that a significant number of cases are documented in the tonsillar region. Along with this, the immunohistochemical (IHC) markers showed diverse patterns among the reported cases. According to recent studies, it has been demonstrated that patients react differently to the same treatment. With the high degree of aggressiveness of DLBCL, up to one-third of patients experience recurrence or develop refractory illness [5,6]. Autologous stem cell transplantation (ASCT) is the conventional salvage treatment for patients with relapsed or refractory DLBCL that is still susceptible to chemotherapy; nonetheless, low success rates in the present era underscore the critical need for new therapeutic options for these patients [7].
A diverse and attentive research on the IHC markers is need of the hour to identify the most important and consistent genes involved. A panel of genes that is comprehensive and directed towards the lesion is inessential to identify in order to treat the patient successfully, and this will also be a boon for situations where surgery is not practical, such as in the tonsillar area. A need of more personalized medicine is needed in the near future. In this case review, we tried to describe our institutional case and highlight the important areas of DLBCL that needs urgent attention in terms of the current therapeutic approach.
A 39-year-old male patient reported to the Department of Oral Pathology with a complaint of swelling on the left side of the neck for 5 months which was insidious in onset and gradually increased in size. The patient also gave a history of lump resection surgery on the right lacrimal fossa region due to the finding of Myolipoma. On clinical examination, facial asymmetry was present due to the swelling on the left side of the neck extending to the back of the ear as shown in Figure 1. On palpation, the swelling was firm, fixed, non-fluctuant, non-tender, and with normal temperature to the surrounding area. Intraoral examination shows erythematous growth over the left tonsillar fossa which is associated with bleeding while tongue cleaning and difficulty in eating food. No history of sweating, fever, or weight loss was present. The CECT of the face and neck shows a moderately ill-defined heterogeneously enhancing soft tissue lesion measuring approximately 49 × 39 × 31 mm on the left tonsillar fossa region. The lesion was also seen infiltrating the left lateral oropharyngeal wall, soft palate, and left parapharyngeal space as depicted in Figure 1. Multiple heterogeneously enlarged lymph nodes are also seen in the left, upper, mid, and lower cervical region (53 × 51 mm) with compression to the left internal jugular vein. The FNAC (fine needle aspiration cytology) sample collected from the left upper cervical swelling reveals singly scattered dispersed atypical cells with round to irregular nuclear outline, salt and pepper-like nuclear chromatin, conspicuous nuclei, and a scant amount of cytoplasm. The FNAC gives an impression of nasopharyngeal carcinoma, lymphoma, and neuroendocrine carcinoma. The microscopic examination of the histologic section shows a hypercellular connective tissue tumor invaded by the collection of small rounds to oval cells arranged in sheets. The cells show a minimal amount of cytoplasm and pleomorphic & hyperchromatic nuclei giving the impression of a round cell tumor. The immunohistochemical findings show a positive expression of LCA, CD20, and BCL6 while negative for BCL2, CD3, CD10, and MUM1 (Figure 2). The final diagnosis proved to be a Diffuse Large B-cell Lymphoma (DLBCL). A thorough review of the cases reported in the literature for DLBCL in the tonsillar area with their clinicopathological and IHC characteristics are described in Table 1. It has been seen that in the reported cases most consistent markers involved are CD20, Bcl2, and Bcl6. Along with it more recent potential markers have also shown expression in DLBCL.
Table 1: Demographic, clinical, radiographic, histological, and immunohistochemical features of reported cases of Diffuse Large B Cell Lymphoma in the tonsillar area. View Table 1
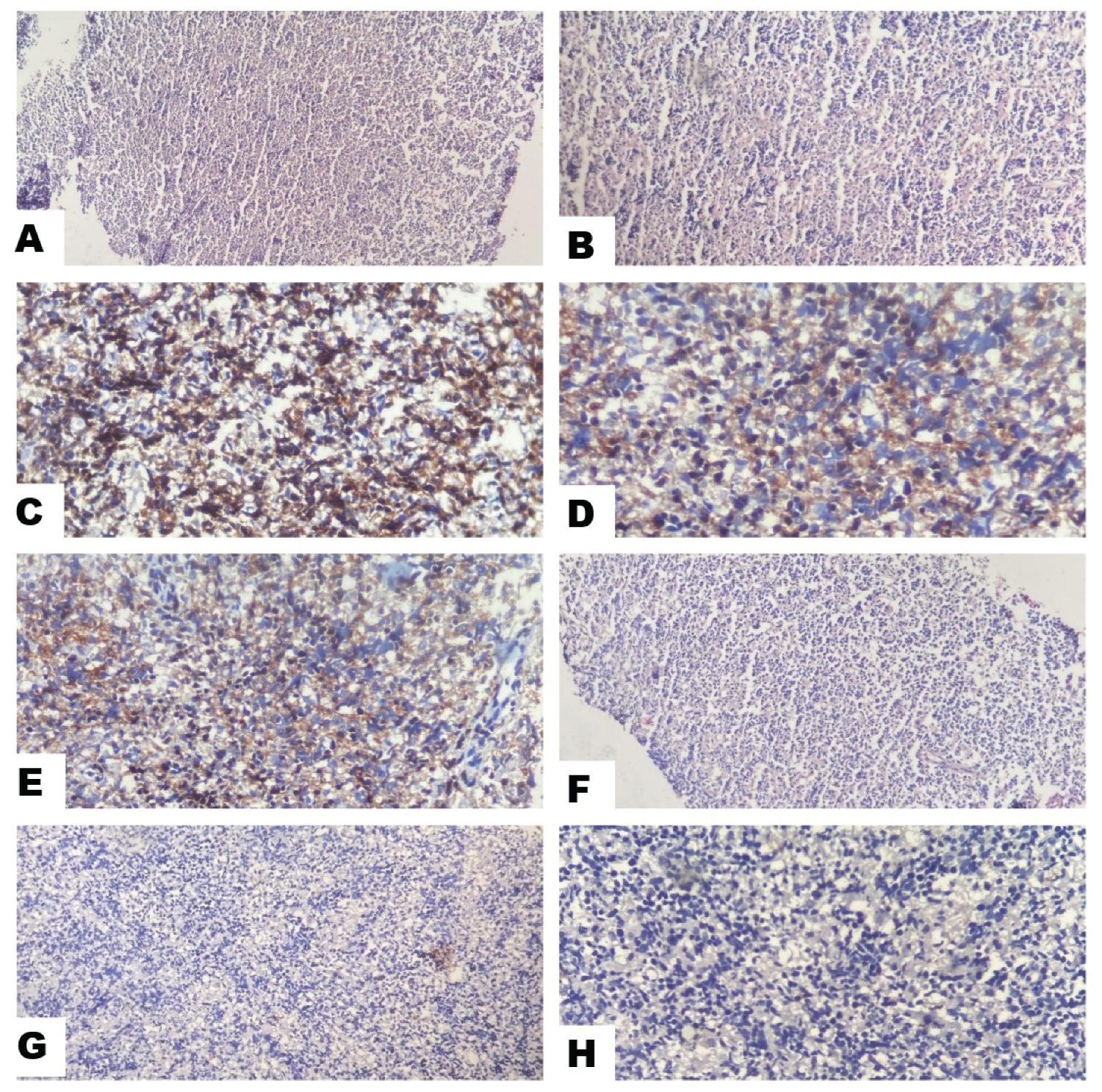 Figure 1: (A) Intraoral clinical presentation with an erythematous mass over the tonsillar region; (B) Depicting the facial asymmetry extra orally; (C) Extraoral swelling in the left side of the neck; (D) Radiographic presentation of the lesion infiltrating the left tonsillar region; (E) Radiographic presentation of the lesion infiltrating the left tonsillar region; (F) Radiographic presentation of the lesion infiltrating the left tonsillar region.
View Figure 1
Figure 1: (A) Intraoral clinical presentation with an erythematous mass over the tonsillar region; (B) Depicting the facial asymmetry extra orally; (C) Extraoral swelling in the left side of the neck; (D) Radiographic presentation of the lesion infiltrating the left tonsillar region; (E) Radiographic presentation of the lesion infiltrating the left tonsillar region; (F) Radiographic presentation of the lesion infiltrating the left tonsillar region.
View Figure 1
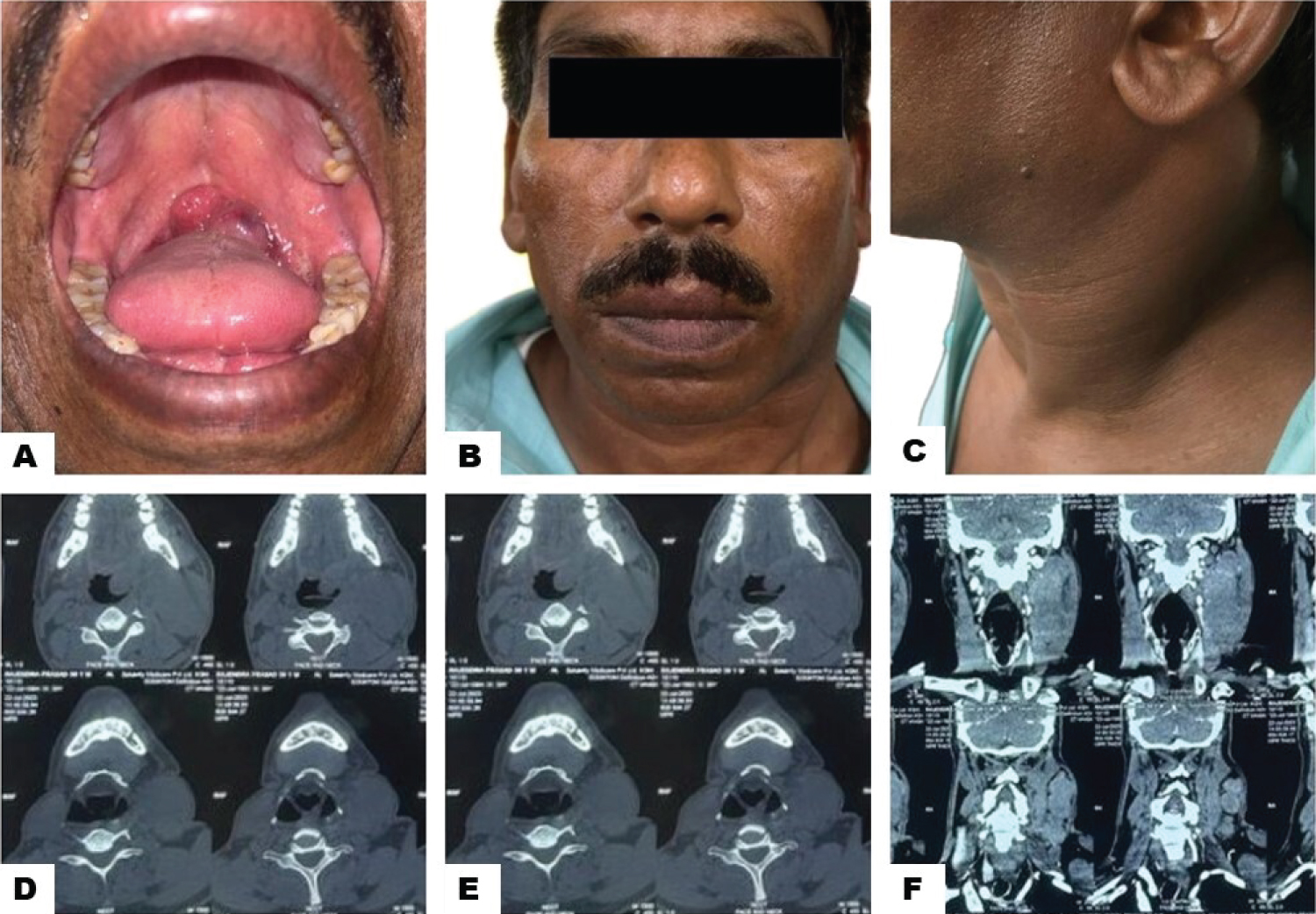 Figure 2: (A) Histological picture of the present case (H&E) showing hypercellular connective tissue tumour with the collection of small round to oval cells arranged in sheets, minimal amount of cytoplasm and pleomorphic & hyperchromatic nuclei; Immunohistochemical characteristics of markers; (B) Histological picture of the present case (H&E) showing hypercellular connective tissue tumour with the collection of small round to oval cells arranged in sheets, minimal amount of cytoplasm and pleomorphic & hyperchromatic nuclei; Immunohistochemical characteristics of markers; (C) Positivity for LCA; (D) Positivity for CD20; (E) Positivity for Bcl2; (F) Negativity for CD10; (G) Negativity for CD3; (H) Negativity for MUM1.
View Figure 2
Figure 2: (A) Histological picture of the present case (H&E) showing hypercellular connective tissue tumour with the collection of small round to oval cells arranged in sheets, minimal amount of cytoplasm and pleomorphic & hyperchromatic nuclei; Immunohistochemical characteristics of markers; (B) Histological picture of the present case (H&E) showing hypercellular connective tissue tumour with the collection of small round to oval cells arranged in sheets, minimal amount of cytoplasm and pleomorphic & hyperchromatic nuclei; Immunohistochemical characteristics of markers; (C) Positivity for LCA; (D) Positivity for CD20; (E) Positivity for Bcl2; (F) Negativity for CD10; (G) Negativity for CD3; (H) Negativity for MUM1.
View Figure 2
Lymphomas refer to a group of tumours that develop in the lymphatic and reticuloendothelial systems. When it comes to tonsillar lymphomas, most of them are non-Hodgkin's lymphomas (NHLs) [8]. The most commonly occurring subtype of NHLs is diffuse large B-cell lymphoma (DLBCL), which accounts for about 30% of all NHLs [9]. The incidence and mortality rates of this tumor have been rising in India for the last few years [10]. But when it comes to clinical presentation, genetic advancements, treatment choices, and prognosis, DLBCL exhibits a wide range, and new entities are often identified and later excluded from this group. Contemporary modifications to the WHO classification scheme for hematolymphoid tumors have identified new entities as: cases showing Epstein-Barr virus (EBV) positivity are now classified as EBV-positive DLBCL, while genetic analyses of DLBCL illustrating mutations in Bcl2, Bcl6, and/or MYC now result in the so-called double-hit and triple-hit high-grade lymphomas [11].
Despite being the most frequent lymphoma to emerge in the oral cavity, only a few small series of DLBCL are available and little information on the clinical course or prognosis of this tumor is available in the literature. According to a recent systematic review, DLBCL primarily affects men and the elderly, while it can also sporadically affect children and young people. The most affected areas in the orofacial region are the salivary glands and Waldeyer's ring, which includes the tonsils, nasopharynx, and base of the tongue [12].
Even with significant advancements in DLBCL therapy, up to 50% of patients experience a recurrence or develop resistance to the therapy. Improvements in patient outcomes have been seen after the introduction of rituximab, a monoclonal anti-CD20 antibody, in conjunction with the CHOP regimen (cyclophosphamide, doxorubicin, vincristine, and prednisone) [13]. Nevertheless, only a small proportion of patients may benefit from this so-called first-line treatment; 30-40% of them remain resistant or may relapse following an initial response. Over the past ten years, a great deal of work has been done to find new treatment options for relapsed/refractory cases and seek to enhance the prognosis for DLBCL patients treated with the R-CHOP regimen [14]. Extensive research has been conducted on the molecular pathogenesis of DLBCL in order to meet this demand. More recently, two groups identified MYC-driven subgroups of DLBCLs using complementary gene expression techniques. A particular signature was obtained from the subgroup of double-hit lymphomas that possessed translocations of MYC and Bcl2/Bcl6 [15].
The variety of genetic characteristics and phenotypes within DLBCL is the biggest obstacle to the effective introduction of targeted treatment in this clinical entity. The fact that DLBCL is a group of diseases rather than a single illness is becoming increasingly evident. Each DLBCL has unique biological and molecular characteristics, and they will all react differently to the therapies currently in use. In order to develop a unique molecular and immunohistochemical characteristic for that patient, it is crucial to investigate further the immunohistochemical and molecular features of DLBCL. This will enable us to give patients more personalized and targeted therapy options to achieve the desired outcomes.
Even though DLBCL is a very aggressive tumor, it is treatable, and combination therapy has proven beneficial for many patients. A significant proportion of patients, meanwhile, still experience tumor recurrence despite repeated treatment. This leads us to hypothesize that the tumor shows varied growth patterns in different individuals. Therefore, a more personalized treatment approach is required to achieve the desired outcomes.
Not applicable.
The authors declare that they have no known conflict of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
All the authors contributed significantly to this manuscript.