Introduction: A number of complications are known to occur in the course of inflammatory bowel diseases. However, perianal fistulas and fissure can occur with or without active inflammatory bowel disease, occurrence of which prior to the development of ulcerative colitis is a rare occasion.
Case presentation: Here we report a case of ulcerative colitis, which was misdiagnosed, treated as a perianal fissure and anal pressure ulcer without recognizing inflammatory bowel disease.
Conclusion: In case of anal fistulas and fissures a multidisciplinary approach should be considered, including both surgical and internal medicine professionals.
Anal fissure, Ulcerative colitis, Misdiagnosed
IBD: Inflammmatory Bowel Disease; GI: Gastrointestinal; CD: Crohn disease; UC: Ulcerative Colitis; MRI: Magnetic Resonance Imaging; TPUS: Transperineal Ultrasonography
Inflammmatory bowel diseases (IBDs) are chronic immune-mediated diseases of gastrointestinal (GI) tract with a periods of remission and relapse. For development of IBD is crucial a complex interaction between host immune system, environment and microbiota in genetic susceptible host. Intestinal dysbiosis leads to different mucosal immune response. Therefore is considered diet is a risk factor for IBD development. Studies in humans showed difference between gut microbiota in patients with IBD and in healthy controls [1,2]. Although perianal disease is typical for patients with crohn disease (CD), it should not be neglected in patients with ulcerative colitis (UC). Patients with UC often suffer from perianal disease which includes hemorrhoids, anal fissures, abscesses and fistulae [3]. History and physical examination which include anorectal examination are first step in diagnosis perianal CD [4]. Colonoscopy with ileoscopy and biopsy is necessary to confirm diagnosis and see which part of gastorointestinal tract is affected. Initial laboratory test should include complete blood count, complete metabolic panel, C-reactive protein level, erythrocyte sedimentation rate, blood urea nitrogen, creatinine, liver enzymes, stool culture and testing for Clostridium difficile toxin. If inflammation is presented, acute phase reactants are at increased levels. Typical endoscopic findings in CD are skip lesions, cobblestoning, ulcerations and strictures whereas in UC pseudopolyps and continuous areas of inflammation are seen [5]. Fecal calprotectin is protein which reflects intestinal inflammation and is used to distinquish IBD from other non-inflammatory GI conditions [6]. Ulcerative proctitis is form of UC in which endoscopy shows diffuse inflammation limited to the rectum [7]. Magnetic resonance imaging (MRI) and transperineal ultrasonography (TPUS) are radiological techniques useful for evaluation of perianal disease in patients with IBD. A pelvic MRI is used as first diagnostic procedure, but TPUS is cheaper and it can be used to follow-up patients with perianal disease [8]. EUS is useful for showing all sphincter structures. Pelvic MRI is gold standard for evaluation of perianal fistula because it is noninvasive. It can also detect silent abscesses and inflammation [4]. There are no reports in the literature of patients with ulcerative colitis who first appeared with perianal disease without other symptoms typical for IBD.
We report a case of a 78-year-old female who was admitted to our clinic with the complaint of fever, rectal bleeding, abdominal cramps and progressively worsening bloody diarrhea. For the last 4 years she has had in few occasions alternating constipation and diarrhea with ingredient of fresh blood. She has been immobile since 2003.
The patient has been controlling ambulatory by the proctologist in other medical institution since 2004 who has verified anal fissure and anal pressure ulcer. Last rectoscopy without biopsy was preformed 2.5 years ago and it showed few rectal erosions. On admission a linear to ovoid shaped ulcerating, bleeding anal fissure was observed (Figure 1).
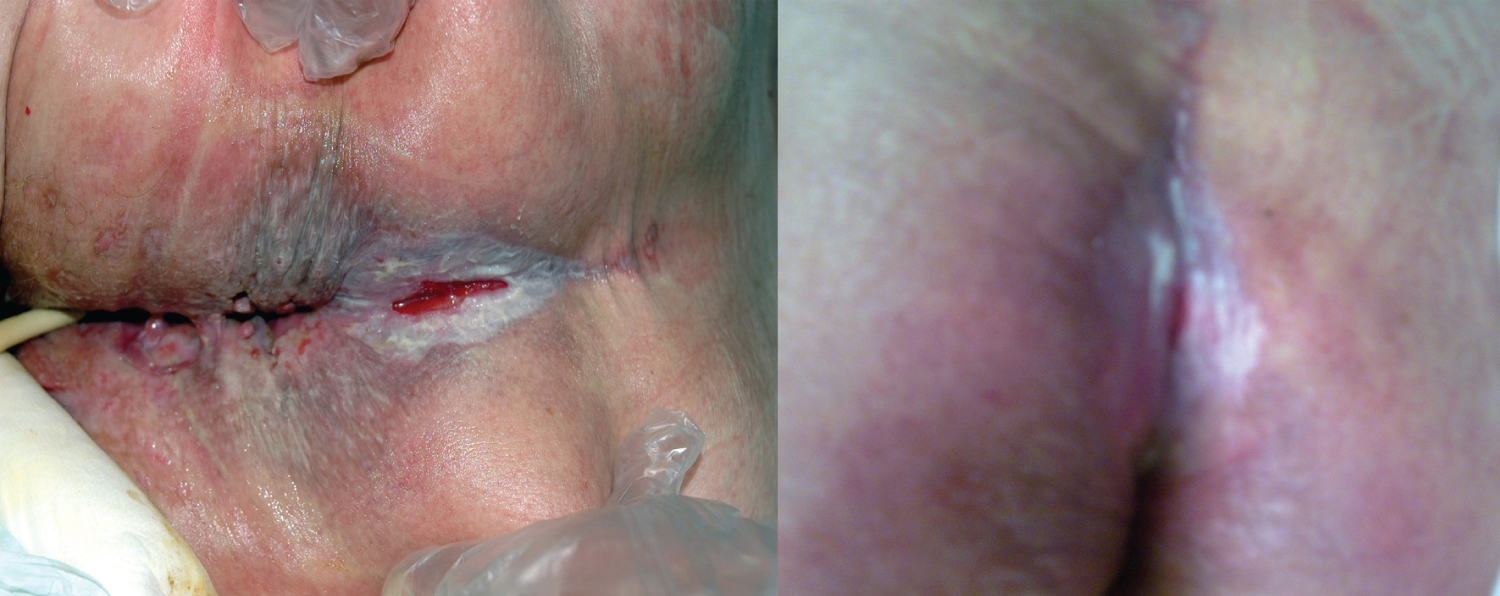 Figure 1: Picture shoes anal fissure, perianal inflammation and a moisture lesion on admission day. View Figure 1
Figure 1: Picture shoes anal fissure, perianal inflammation and a moisture lesion on admission day. View Figure 1
Laboratory data showed microcytic hypochromic anemia, iron deficiency, normal total leukocyte and platelet count, elevated ESR (45 mm/hr) and CRP (165 mg/L). Other values were normal. A stool studies were negative, as the C difficile toxin A/B assay. Esophagogastroduodenoscopy with biopsy showed chronic gastritis changes. Total colonoscopy with terminal ileoscopy showed diffusely hyperemic and edematous mucosa of the rectum, sigma and descending colon, with disappearance of the submucosal vascular network, granular appearance, and few scattered shallow ulcerations with fibrin and clots. Pathology revealed the inflammation limited to the mucosa, neutrophilic infiltrate along with few crypt abscesses. MSCT showed significant wall thickening from left colic flexure in continuity to the rectum, and in right anal region anal fistula leading to the skin surface (Figure 2). Videoendocapsule investigation did not detect any lesion of small intestine.
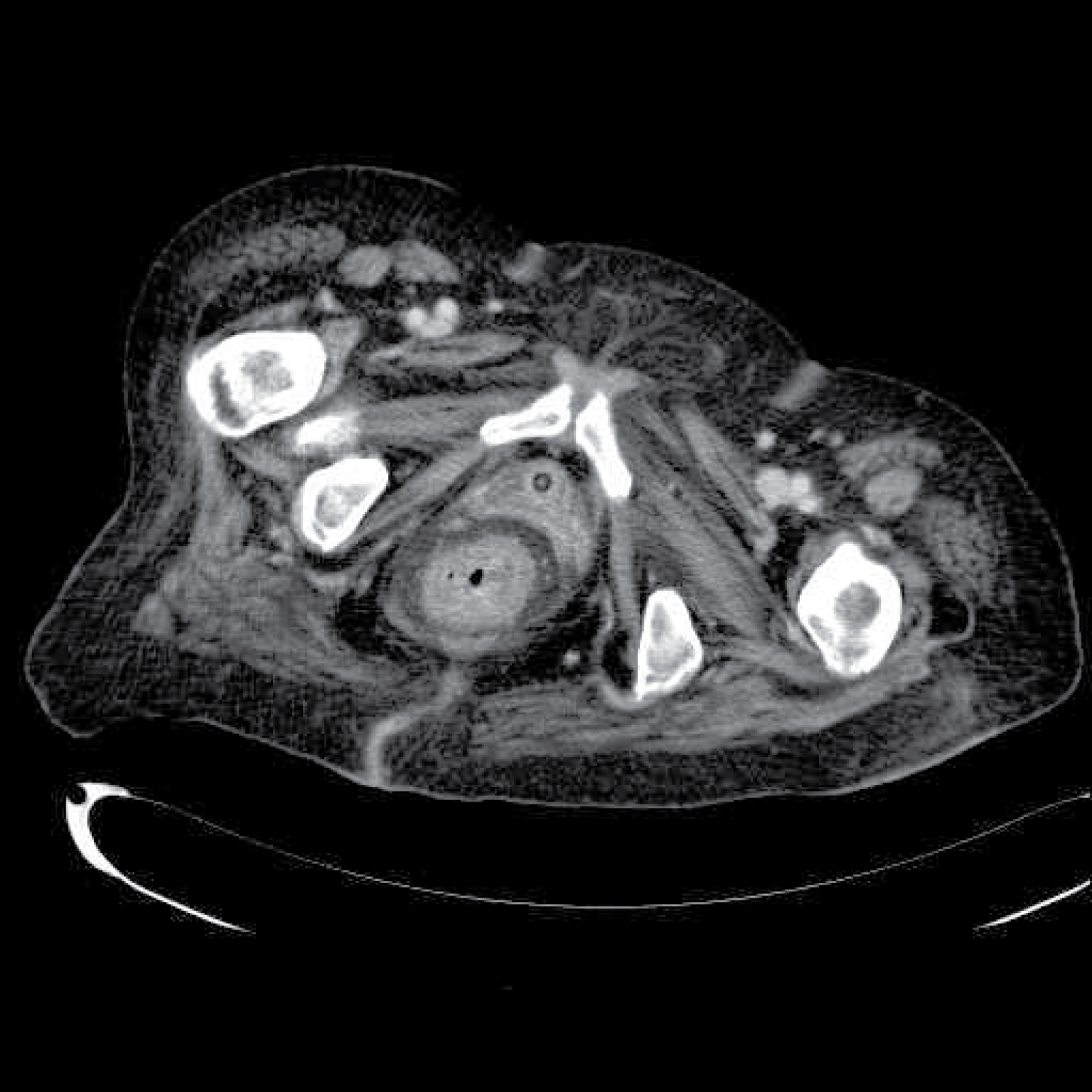 Figure 2: MSCT shoes rectal wall thickening, blurring of perirectal fat tissue due to inflammation, rectocutaneus fistula on the right side of the pelvis. View Figure 2
Figure 2: MSCT shoes rectal wall thickening, blurring of perirectal fat tissue due to inflammation, rectocutaneus fistula on the right side of the pelvis. View Figure 2
According to current clinic, endoscopic, histopathologic diagnostic criteria, the findings were suggestive of ulcerative colitis (UC) [9].
After introducing peroral medical therapy with corticosteroids and 5-ASA with antibiotic combination of ciprofloxacin and metronidazole, erythrocyte concentrate supplementation, albumins and parenteral iron replacement, clinical and subjective improvement were noticed, and anal fissure was in regression [9] (Figure 3).
 Figure 3: Picture shoes closed anal fissure, perianal inflammation and a moisture lesion healed after treatment. View Figure 3
Figure 3: Picture shoes closed anal fissure, perianal inflammation and a moisture lesion healed after treatment. View Figure 3
One month later, her bloody diarrhea disappeared, fissure was significantly smaller, and results of the control laboratory investigations were within normal range. Endoscopy showed improvement. Two years after discharge patient underwent a MSCT scan which reviled normal thickness of the rectal wall, no signs of perirectal fat tissue inflammation and the rectocutaneous fistula was not visible anymore (Figure 4).
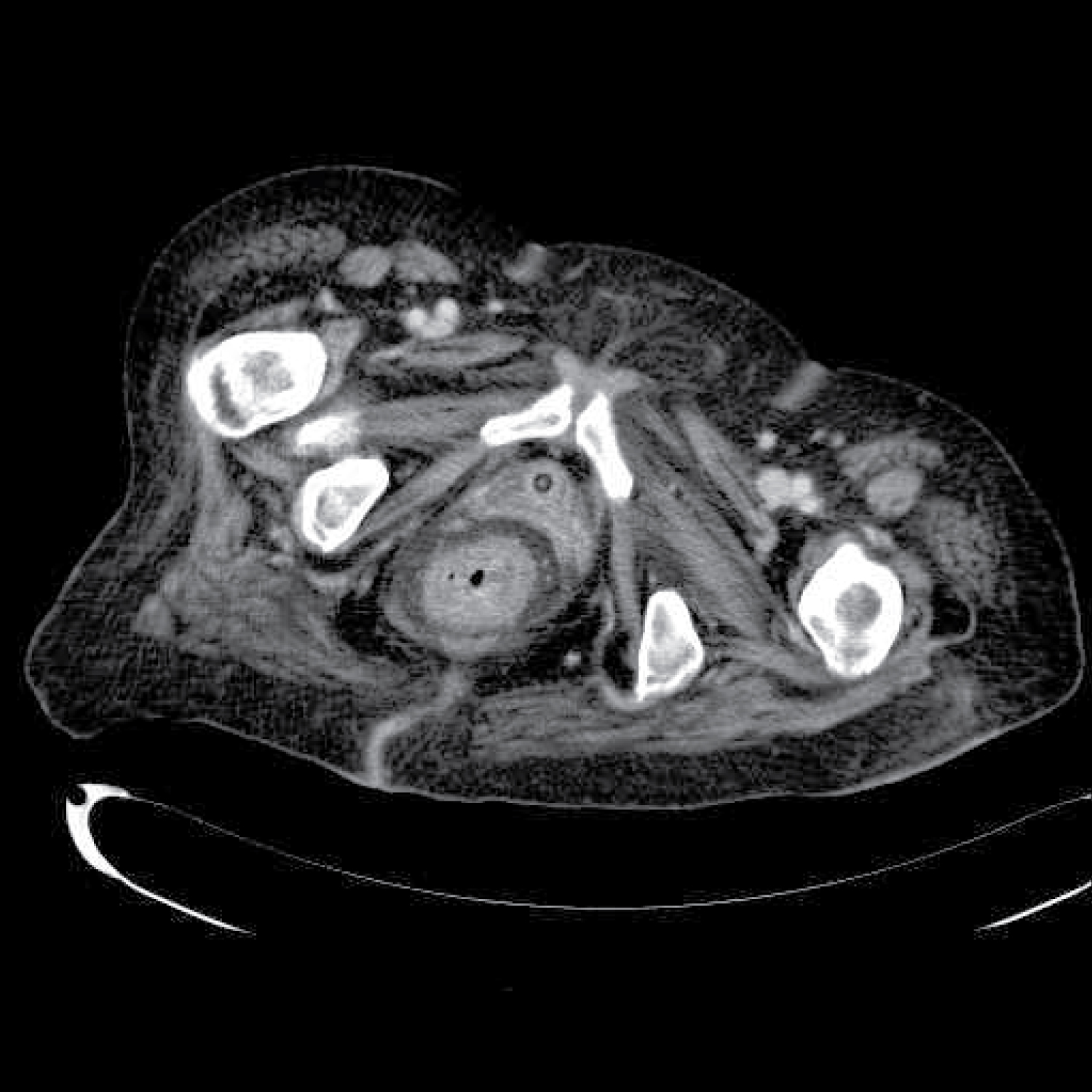 Figure 4: MSCT shows closed anal fistula in anal region and no wall thickening or fat tissue inflammation. Only the fibrous track formed after the regression of the fistula can be seen. View Figure 4
Figure 4: MSCT shows closed anal fistula in anal region and no wall thickening or fat tissue inflammation. Only the fibrous track formed after the regression of the fistula can be seen. View Figure 4
Fistulizing perianal disease is quite common in patients with crohn disease (CD) and when fistulas occur in the setting of UC, the diagnosis is often questioned [10]. The reported incidence of fistula in CD ranges from 17% up to 50% [11], and fissures up to 27.6% [12]. In approximately 10% of patients, perianal fistulization is the initial manifestation of Crohn’s disease [3]. Contrary to CD, incidence of fistulas in UC is up to 4.2%, and fissures up to 4.5% [10,13].
Although the literature reports that perianal disease can occur with or without other symptoms of UC [11,13], we didn’t find any data of the incidence of fissures and fistulas before presenting other manifestations of ulcerative colitis.
In our patient, according to her history and medical documentation, fissure developed before the full clinical feature of IBD and fistula was recognized at the same time as the diagnosis of UC.
• In chronic fissures the association with other pathologies should be considered.
• Patient reports symptoms of weight loss, weakness or abdominal symptoms referable to the gastrointestinal track.
• When presenting with perianal disease patient should be check for inflammatory bowel disease.
The authors declare that there is no conflict of interest.
All authors contributed equal to the creation of this case report.