Dengue is a very common viral infection in tropical zones, it is transmitted by vectors to humans by mosquito bites of the genre: Aedes. Oriental Mediterranean, Americas, Southeast Asia, Pacific, and Africa are all known as endemic zones for dengue. The treatment of severe dengue is based on the administration of intravenous fluids (IVF) and the management of complications. The mainstay of the management is the meticulous administration of fluids to ensure adequate intravascular volume to restore vasculopathy, watching carefully for overload risk. We carried out a state of the art on fluid-therapy during the critical phase of dengue, including the type (crystalloids versus colloids, hypotonic and hypertonic solutions), volume to infuse and duration of therapy from the most recent publications. This is an area where urgent research is needed.
Dengue, Fluid requirement, Plasma leakage, Fluid overload, Critical phase
Dengue has a cyclic epidemic behavior, with approximately half of the global population in risk of infection [1-3]. At least 390 million infections are reported each year, causing high morbidity and mortality among young adults, with an important cost for society through the loss of productivity of the affected population [3-6]. Delays on fluid therapy during critical phase has been identified as the leading cause of death [1,7].
Plasma leakage during the critical phase (48 to 72 hours after febrile defervescence) provokes shock, multiple organic dysfunction, and death [8], unless there is an adequate intravenous fluid (IVF) management to correct hypovolemia without delay [9]. Once the plasma leakage ceases, the extravasated fluids are reabsorbed into the intravascular space in most of the patients [2]. In other cases, there are complications; some of which are related with fluid overload beyond the tissue damage caused by the viral infection [6].
Since there is no specific antiviral treatment that modifies the natural history of the disease [7], the meticulous IVF administration has become the most effective strategy [6]. The recommendations of the different societies on IVF management in adult population with dengue are mainly extrapolated from studies performed on pediatric population [9-11], or based on consensus of expert opinions, assumptions from observational studies with poor methodological rigor. We present a review of current literature on fluid requirement in dengue critical phase, including the options of fluids (crystalloids versus colloids, hypotonic and hypertonic solutions); volume to infuse and duration of therapy.
The review involved keyword searches of electronic databases in January 2022. Review search terms included 'dengue', 'crystalloid solutions', 'saline solution', 'Ringer's lactate', 'colloids' and 'fluid therapy'. The review included observational studies, clinical trials, systematic reviews describing the choice of fluid in adult dengue patients. Research was limited to English. Duplicated records were excluded. The reference lists of the final papers were checked to ensure inclusion of further relevant papers (Figure 1).
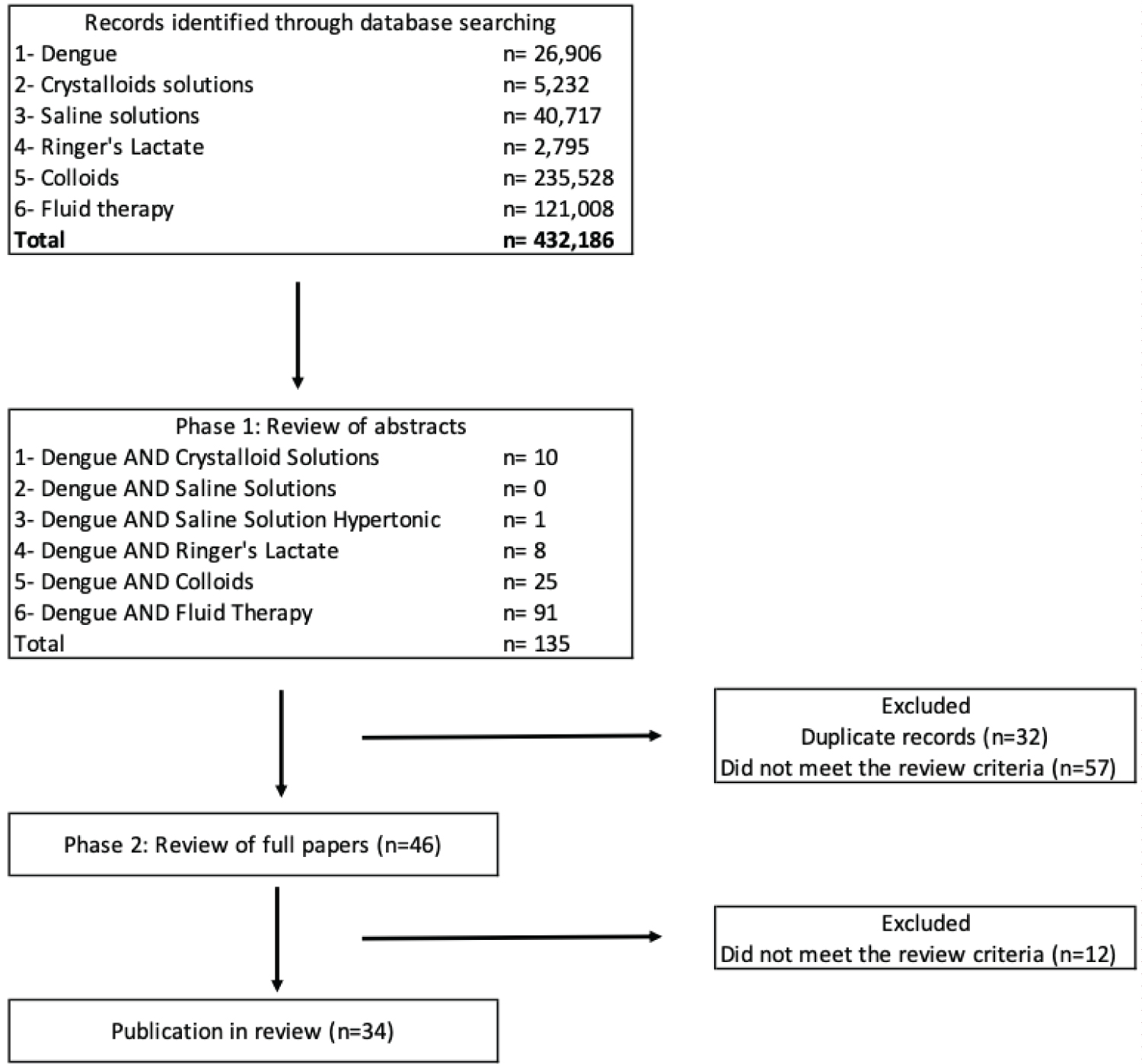 Figure 1: Literature search process and study selection.
View Figure 1
Figure 1: Literature search process and study selection.
View Figure 1
Many patients infected with dengue virus remain asymptomatic [12]. Nevertheless, symptomatic illness begins abruptly after the bite of an infected Aedes mosquito, incubation period (4 to 10 days), followed by three phases: febrile, critical, and recovery phase [13]. The febrile phase is characterized by sudden high fever and dehydration (2 to 7 days), other signs include asthenia, headache, retro-orbital pain, myalgia, chills, vomiting, diarrhea, and a generalized maculopapular rash [1].
The critical phase starts around the time of defervescence, generally lasts 24 to 48 hours [12]. It is characterized by plasma leakage, shock, and organ hypoperfusion (hepatitis, encephalitis, myocarditis) resulting in multiple organ failure, acidosis due to hemodynamic collapse, and coagulation disorders [13,14]. Patients in this phase require close monitoring and urgent treatment to correct volume depletion [6]. The objective of fluid therapy during this phase is to guarantee an adequate intravascular volume until the vasculopathy is reversed, preventing progression to shock without causing volume overload [5,7,9]. Once plasma leakage ceases at the end of 48 to 72 hours, the patient's symptoms resolve and gradual fluid reabsorption into the intravascular space occurs, which is the recovery phase [2].
The endothelial dysfunction in dengue is the hallmark of severe dengue, causing plasma leakage to the interstitial space affecting tissue perfusion and generating multiple organ dysfunction and death [12]. Several components of the virus have been related to this event, for example it has been found that the NS1 protein of the virus induces damage to glycocalyx proteins by activating enzymes such as human sialidases, cathepsin L and heparanase that degrade the glycocalyx independently of receptor patterns associated with pathogens such as TLR4 or inflammatory mediators such as TNF-alpha, IL6 and IL8 [15].
Additionally, this protein decreases the expression of the intercellular binding protein CD44 in human endothelial cell cultures, increasing the expression of hyaluronan and macrophage chemoattraction [16]. In patients with critical dengue, the increase in NS1 levels during the plasma leakage phase is associated with high levels of hyaluronan in serum and the induction of antibodies against certain NS1 epitopes that, due to cross-reactivity and molecular mimicry, recognize intercellular junction proteins in the endothelium and weaken the interactions favoring more capillary leak [17].
Current management of dengue infection does not have any specific treatment except cautious monitoring and appropriate fluid replacement therapy [2]. Research evidence is scarce regarding fluid requirement or the choice of IVF during critical phase. In recent years, studies have supported the use of balanced solutions over those containing high concentrations of chloride given the risk of kidney injury associated with acidotic states [18]. Other studies have shown harmful potential of colloids in the resuscitation of critically ill patients [19]. Though these studies were not carried out in patients with dengue, they provide important data for the management of severe forms of this disease, possible risks associated with the type of fluid and amount of volume that are traditionally used in clinical practice.
Dengue patients respond differently to fluid therapy when compared to sepsis patients because fluid loss is roughly equivalent to plasma loss [7,20]. IVF management in this patients' should be based on the principle of adequate replacement of fluid loss oriented to achieve euvolemia state, minimizing the risk of fluid overload [5, 21]. In dengue, the choice of the specific fluid is limited; crystalloids continue to be the WHO/PAHO recommendation [12].
There is a theoretical benefit known of colloid solutions for plasma expansion and oncotic pressure increase over crystalloid solutions [22]. Nevertheless, the magnitude of such effect is determined by the average molecular weight of the colloid molecule and the retention time in circulation, effects on coagulation, interference with organ function, and anaphylactoid reactions, are some of the known limitations for the use of dextrans or starches in different clinical scenarios [23,24].
One of the biggest concerns regarding the use of colloids is the impact on coagulation [22]. For example, dextrans bind to the von Willebrand factor/factor VIII complex and alter coagulation in vitro; however, this has not shown to be of clinical significance. Gelatin has a minor effect on coagulation, but the risk of allergic reaction is higher [25]. Allergic reactions have also been observed in patients treated with dextran-70 and dextran-40 and may cause osmotic renal damage in hypovolemic patients [25].
Colloids were used for many years as the fluid of choice in dengue shock to urgently restore blood pressure in patients with profound shock (pulse pressure < 10 mmHg) based on clinical, paraclinical (decreased hematocrit) and hemodynamic benefits (cardiac index) during the resuscitation phase [22]. However, such benefits are not sustained over time, with no differences between the various fluid regimens in terms of either clinical outcomes and/or severity of fluid overload in 48 to 72 hours [10].
Crystalloid solutions, which contain water-soluble electrolytes including sodium and chloride, lack proteins and insoluble molecules [24]. They are classified by tonicity, so that isotonic crystalloids contain the same amount of electrolytes as the plasma [24]. Hypertonic and hypotonic crystalloids contain more and less electrolytes than the plasma respectively [24].
The most widely used crystalloid is 0.9% saline, a hypertonic solution with an osmolality of 308 mOsm/L that has higher sodium and chloride levels than normal plasma [23,24]. Normal saline is a suitable option for initial resuscitation as they equilibrate freely across the intravascular and extravascular compartments; however, high volumes can cause fluid overload as well as hyperchloremic acidosis which might aggravate or suggest lactic acidosis from prolonged shock [20]. Therefore, if serum chloride begins to exceed the normal range, alternatives such as Ringer's lactate may be preferable because of its lower sodium and chloride content with an osmolality of 273 mOsm/L [25]. Anyway, it should be avoided in people with liver failure, in whom the ability to metabolize lactate is reduced [20].
There is less evidence for hypotonic solutions (0,45% solution). In the past it was recommended by the World Health Organization (WHO), concerning sodium overload in patients with severe malnutrition, being appropriate when the main problem was decreased intracellular volume due to dehydration [12]. Today, hypotonic solutions are not currently recommended for shock correction until circulating volume has been restored with isotonic solutions [26].
Evidence for hypertonic (7,5%) saline solutions in dengue is limited, its clinical application has been described predominantly in surgical cases or trauma [26]. Hypertonic saline solutions restore intravascular physiology by mobilizing fluid from the intracellular compartment to the intravascular space, it also serves as a plasma volume expander [27]. Knowing its advantages, it could be an alternative in cases of hemorrhagic shock with minor fluid requirement and less risk of fluid overload [28].
Novel crystalloid solutions have become available [29]. "Balanced solutions" is used generally to describe different solutions with diverse electrolyte composition similar to plasma composition, precising that balanced solutions are neither physiological nor plasma-adapted [29]. This solution has been proved in critically ill patients with hypotension or shock from a variety of etiologies, demonstrating a significant reduction in hospital or 28-/30-day mortality compared with 0.9% saline [30]. Nevertheless, comparative clinical effects in dengue infection remain uncertain.
A randomized, double-blind comparison of four intravenous fluids (6% dextran-70, 3% gelatin, Ringer's lactate, or 0.9% saline) in 50 children with dengue shock found that colloids restored cardiac index, blood pressure and hematocrit more rapidly than crystalloids over a two-hour period during the initial resuscitation. Nonetheless, in the different regimes, all children recovered, and no difference was observed in the effects assessed after two hours [9]. In another study of 230 children with dengue shock, there was no clear superiority between four fluid regimes (0.9% saline, Ringer's lactate, dextran, and gelatin) during initial resuscitation; though the use of colloids in dengue shock led to more rapid reversal of shock, it did not show clear advantages between fluids in terms of final cardiovascular stability or the need for rescue colloid [11]. In a randomized trial of 383 children with dengue shock, crystalloids were compared to colloids (dextran-70 or 6%, hydroxyethyl, starch). Children who received Ringer's lactate for primary resuscitation took longer to achieve initial cardiovascular stability than patients who received colloids, but the degree of compromise during this period was generally not sufficient to warrant colloid intervention, and time to final cardiovascular stability did not differ between fluid treatment groups [10]. Whereas there is some controversy as to the whether colloids or crystalloids are best, it appears that both can be effective in terms of hospital stay and mortality.
In conclusion, most dengue patients respond adequately to judicious treatment with crystalloid solutions. Routine colloid intervention is not indicated. There are no significant differences in the adverse effects (clinical fluid overload, or furosemide requirement) of the various fluids, except in the incidence of allergic-type reactions against colloids [26].
Rapidly correcting hypovolemia without causing volume overload should be the goal of therapy during the critical phase [9]. Considering giving uncontrolled fluids can end up in fluid overload that could exacerbate plasma leakage into the extravascular compartments and lead to negative repercussions such as respiratory distress from massive pleural effusion and circulatory overload leading to pulmonary oedema, ascites [5], it is important to strike a balance between maintaining adequate organ perfusion and preventing fluid excess. There are no randomized controlled trials comparing rates and amount of fluid to be given during the critical phase of the illness.
Based on hemodynamic status (conscious level, heart rate, peripheral pulse, blood pressure, capillary refill time, urine output) and laboratory parameters (hematocrit and platelet count) the volume and amount of fluid infused can be guided [31]. Its worthy to mention that the minimum volume of IVF required, or target endpoint will be surrogated to maintain good perfusion and urine output of at least 0.5-1 mL/kg/h during the critical phase [5].
The 2009 WHO classifies patients according to severity, warning signs and associated conditions (pregnancy, morbid obesity, diabetes mellitus, renal or cardiovascular impairment, hepatopathy, hemolytic diseases, age under 1 year or over 65 years) and depending on it, treatment decisions are made [12].
In patients with dengue with warning signs IVF are indicated, figure 2. Immediately administer crystalloid solutions at 10 ml/kg of bodyweight in the first hour; preferably give balanced electrolyte solutions, such as Ringer's acetate or lactate or 0.9% saline solution [12]. Monitor IVF with hematocrit, nevertheless, the lack of a hematocrit should not delay initiation of hydration [31].
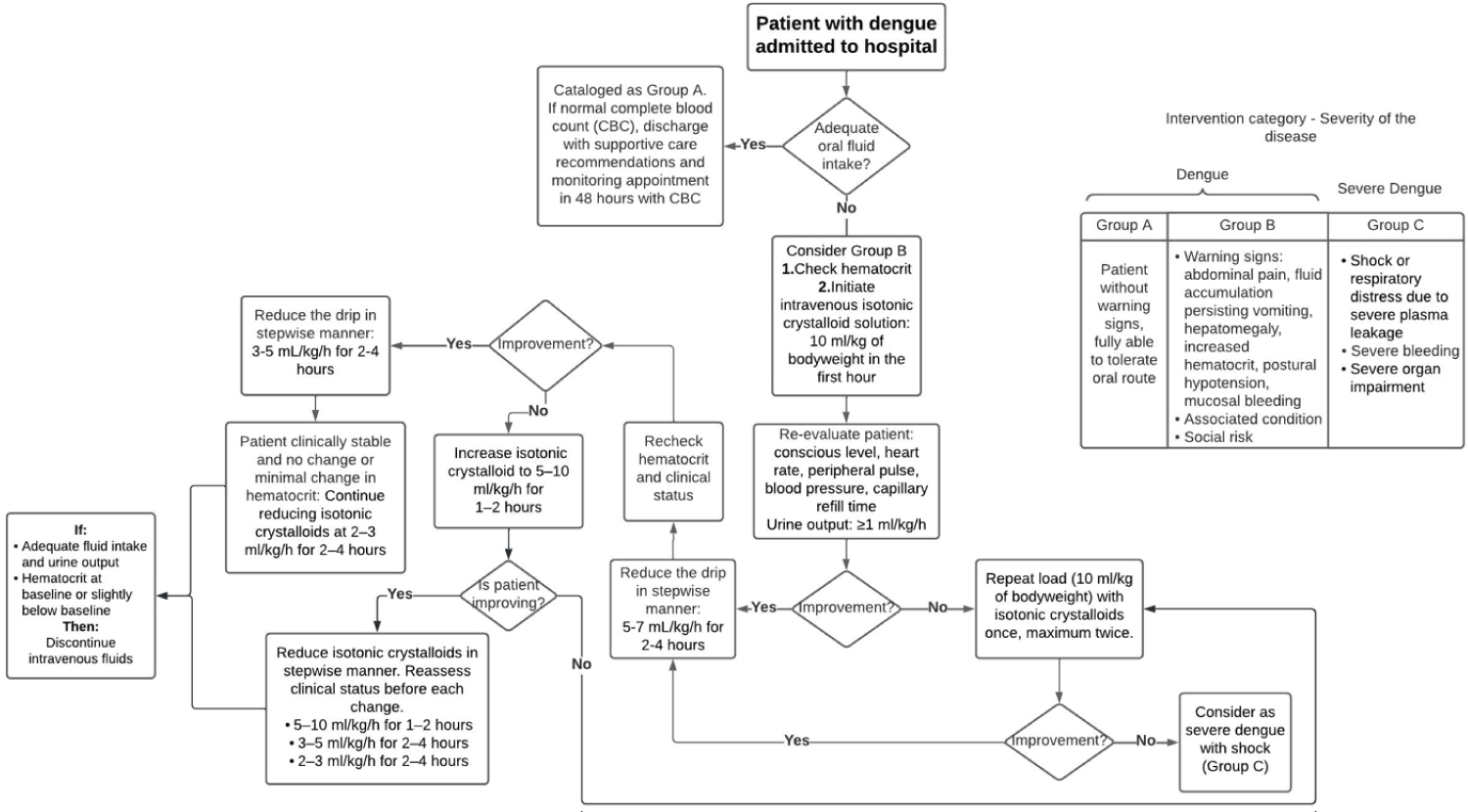 Figure 2: IVF management for patients with warning signs.
View Figure 2
Figure 2: IVF management for patients with warning signs.
View Figure 2
Re-evaluate the patient, if clinical improvement is observed and urine output is ≥ 1 ml/kg/h, reducing IVF rate to 5-7 ml/kg/h, maintaining this dose for the following 2-4 hours. If clinical status allows continue tapering the drip at a rate of 3-5 ml/kg/h for 2-4 more hours. Reassess patient's condition, if improvement continues, reduce the dose to 2-4 ml/kg/h [12].
If vital signs deteriorate or hematocrit rapidly rises, increase rate to 5-10 mL/kg/h for 1-2 hours. If condition continues worsening after three loads of 10 ml/kg/h, the case will be managed as if it were severe dengue with shock [31].
In patients with dengue shock, figure 3, it is recommended to initiate aggressive fluid resuscitation with a crystalloid fluid at a rate of 20 ml/kg of body weight infused in 15-30 minutes. Afterwards, reassess clinical status and determine if there is improvement [12]. If shock signs disappear, reduce fluid volume to 10 ml/kg/h, for 1-2 hours, constantly monitoring the patient's hemodynamic condition and hematocrit. If clinical evolution is satisfactory, continue tapering the drip at a rate of 5-7 ml/kg/h for 4-6 hours. From then on, reduce IVF in a stepwise manner to 3-5 ml/kg/h for 2-4 hours, continue tapering to maintain hydration at a rate of 2-4 ml/kg/h for 24-48 h.
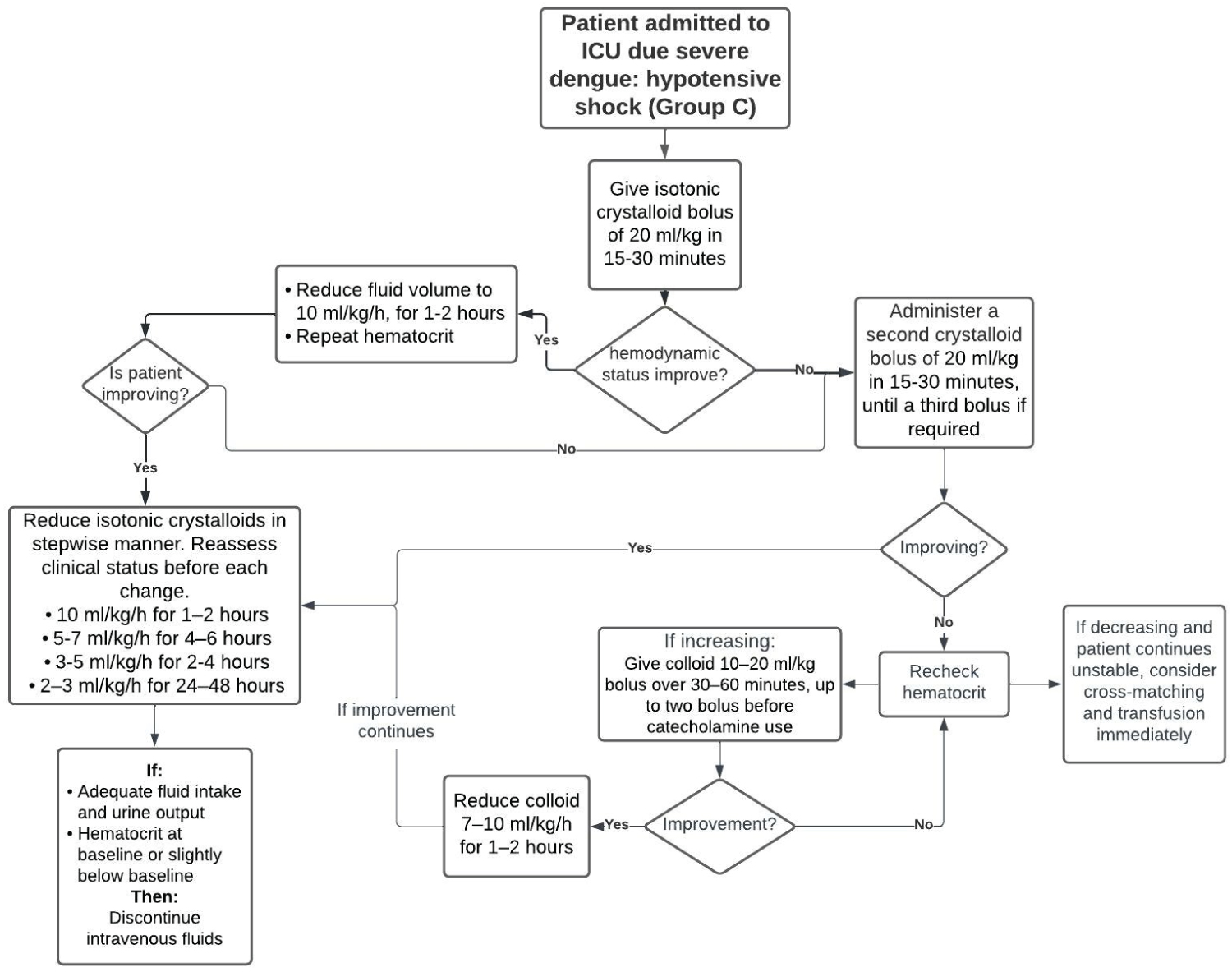 Figure 3: IVF management for patients with dengue shock.
View Figure 3
Figure 3: IVF management for patients with dengue shock.
View Figure 3
It's necessary to reassess clinical status and hematocrit before each change [12]. If the patient does not improve, a second rehydration bolus should be administered, at a rate of 20 ml/kg in 15-30 minutes, with a maximum of three bolus if required. If after the third administration the patient continues unstable an exceptional dose of colloid solution is needed at a rate of 10-20 ml/kg infused in 30-60 minutes. Up to two colloid boluses may be given before determining pumping function and catecholamine use [12].
If the patient's condition improves, IVF should be gradually diminished, crystalloids should be started with a reduction in a stepwise manner [5].
There's an increasing interest in this area. A study by Kularatne, et al. revealed approximately 3000 ml fluid per 24 h being required in dengue patients to maintain vital parameters [32]. A recent approach to fluid management in dengue is pointed out by Madanayake, et al. who suggest IVF replacement of the maintenance fluid and a 5% deficit during the critical phase of 48 hours [6]. Normal maintenance fluid per hour can be calculated based on Holliday-Segar formula, published in 1957, which described the 100/50/20 rule according to the body weight [33]. Finally, the total fluid requirement during the 48-h critical phase for an average adult, weighting 50 kg or more is 4600 ml [1,6].
The volume and quality of fluid infused should be dictated by clinical judgement and changes in clinical variables [21,31]. Restricting the amount of fluid in fear of fluid overload may lead to impaired organ perfusion and tissue hypoxia, but clinicians need to be cautious when exceeding fluid amount due the risk of overload [6, 21].
IVF are usually needed during the critical phase for no more than 24 to 36 hours after resuscitation [12]. However, patients identified very early in the critical period will require more frequent clinical evaluations to determine the need to increase the infusion rate [31,34]. Accordingly, these patients may require longer IVF administration, for more than 60 to 72 hours unless other complications occur [20,34].
Patients should be closely monitored throughout the critical phase until risk period is over [12,21]. Observe patient for signs of plasma leakage, early signs of shock, and occult bleeding [31]. Provide supervised care hourly, monitoring vital signs and peripheral perfusion, urine output up to 4 hours after critical phase ends. Hematocrit needs to be checked before and after fluid resuscitation, then every 12-24 hours. Blood glucose every 6-12 hours. Other organ functions (electrolytes, liver function tests, arterial blood gases, creatinine, blood urea nitrogen, cardiac enzymes, and coagulation profile) are indicated by clinical status [12].
Once patients begin to respond to the initial fluid infusion, the infusion rate is reduced at scheduled intervals for the next 24 hours [12,21]. Limiting the duration of IVF therapy to the minimum necessary is essential to reduce the occurrence of intravascular fluid overload during the recovery phase, which typically begins 12 to 24 hours after resolution of the vascular leakage [7,20,31].
Patients with severe dengue can deteriorate quickly during defervescence, with rapid onset of shock due to increase in vascular permeability during the critical phase. The severity of plasma leakage dictates a dynamic nature of the level of management. Supportive care, appropriate fluid therapy guided by vital signs, hematocrit, and urine output keep being the mainstay management. Less is more, standardizing IVF management should be a priority research topic in public health.