Background: Vulvovaginal candidiasis is a gynecological condition that is a frequent reason for consultation among pregnant women caused by yeast of the genus Candida. The present study aimed to determine the prevalence and antifungal resistance profile of vulvovaginal candidiasis infections among pregnant women in the city of Maroua.
Method: A cross-sectional study was conducted including pregnant women who came for routine antenatal visits (ANV) in two health centers: The Maroua Regional Hospital and the Domayo Catholic Private Integrated Health Centre. Cervical vagina swabs were collected from 243 patients for direct examination, gram staining, and cell culture on Sabouraud chloramphenicol medium. The plates were incubated at 37 ℃ and reading was done after 48 hours. The identification of yeasts was based on the filamentatous test and the use of Candida-chromagar medium. An antifungigramme was used to evaluate the resistance profile of the isolated yeast.
Results: The direct examination and culture yielded a prevalence of vulvovaginal candidiasis (VVC) of 53.07% and 51.33%, respectively, at the Maroua Regional Hospital and the Domayo Catholic Private Integrated Health Centre. Four species of Candida were isolated with a predominance of C. albicans (63.78%), followed by C. glabrata (26.78%), C. krusei (7.87%) and C.tropicalis (1.57%). The most affected age group was 20-25 years. Nystatin, Miconazole, Econazole, Fluconazole, 5-Flucytosine, Amphotericin B, and Ketanazole demonstrated good antifungal activity. However, high cases of resistance were observed with 5-Flucytosine (55.11%) and Amphotericin B (54.33%).
Conclusion: The prevalence of vulvovaginal candidiasis is very high in pregnant women. Candida albicans is the most frequent candidiasis and presents a high resistance to antifungal drugs such as Amphotericin B and 5-Flucytosine 10. There is a need to implement continuous epidemiological studies of vulvovaginal candidiasis and to rethink the probabilistic antifungal therapy in case of vulvovaginal candidiasis in pregnant women.
Prevalence, Candida, Antifungals, Resistance profile, Vulvovaginal
Vulvovaginitis is a gynecological condition characterized by inflammation of the vulva and vagina caused by microorganisms such as yeast and bacteria. Vaginal infection is one of the most common gynecological conditions and therefore one of the most common reasons for women to seek medical attention [1]. Vulvovaginitis signs and symptoms are dysuria, dyspareunia, vaginal dryness or vulvar burning, and pruritus [2]. Vulvovaginal candidiasis (VVC) is an infectious vaginitis caused by yeasts of the genus Candida. However, its contamination is exclusively endogenous and depends on the species of yeast responsible [3]. Many women (70-75%) in normal health present at least one episode of VVC during their lifetime [4].
The prevalence of both superficial and deep candidiasis has increased considerably in recent years and is closely related to factors such as hormonal changes during pregnancy, the use of oral contraceptives, local factors (such as poor hygiene) and general factors (such as diabetes) [5]. The flora plays a protective role in preventing the proliferation of pathogenic germs through the production of lactic acid and hydrogen peroxide by lactobacillus [6]. Pregnant women are at risk because during pregnancy there is an increase in estrogen levels which favors the deposition of glycogen and other substances in the vagina. In addition, it is well established that pregnancy is associated with a slight decrease in immunity [4].
The frequency of these Candida infections and the symptoms they cause has led to the intensive use of antifungal drugs, leading to the development of resistance, and some fungal species are no more sensitive to certain antifungal drugs. In Cameroon, few data on the epidemiology of female genital tract infections and the antifungal resistance profile of VVC infections are available [4]. This study aimed to determine the prevalence and profile of resistance to antifungal drugs of VVC in pregnant women attending antenatal visits in two hospitals in the city of Maroua and to propose control strategies.
A cross-sectional descriptive study was carried out in the Regional Hospital of Maroua and a private Catholic Health Centre in the Far North region of Cameroon. The location of the different health structures in the study site is presented in Figure 1.
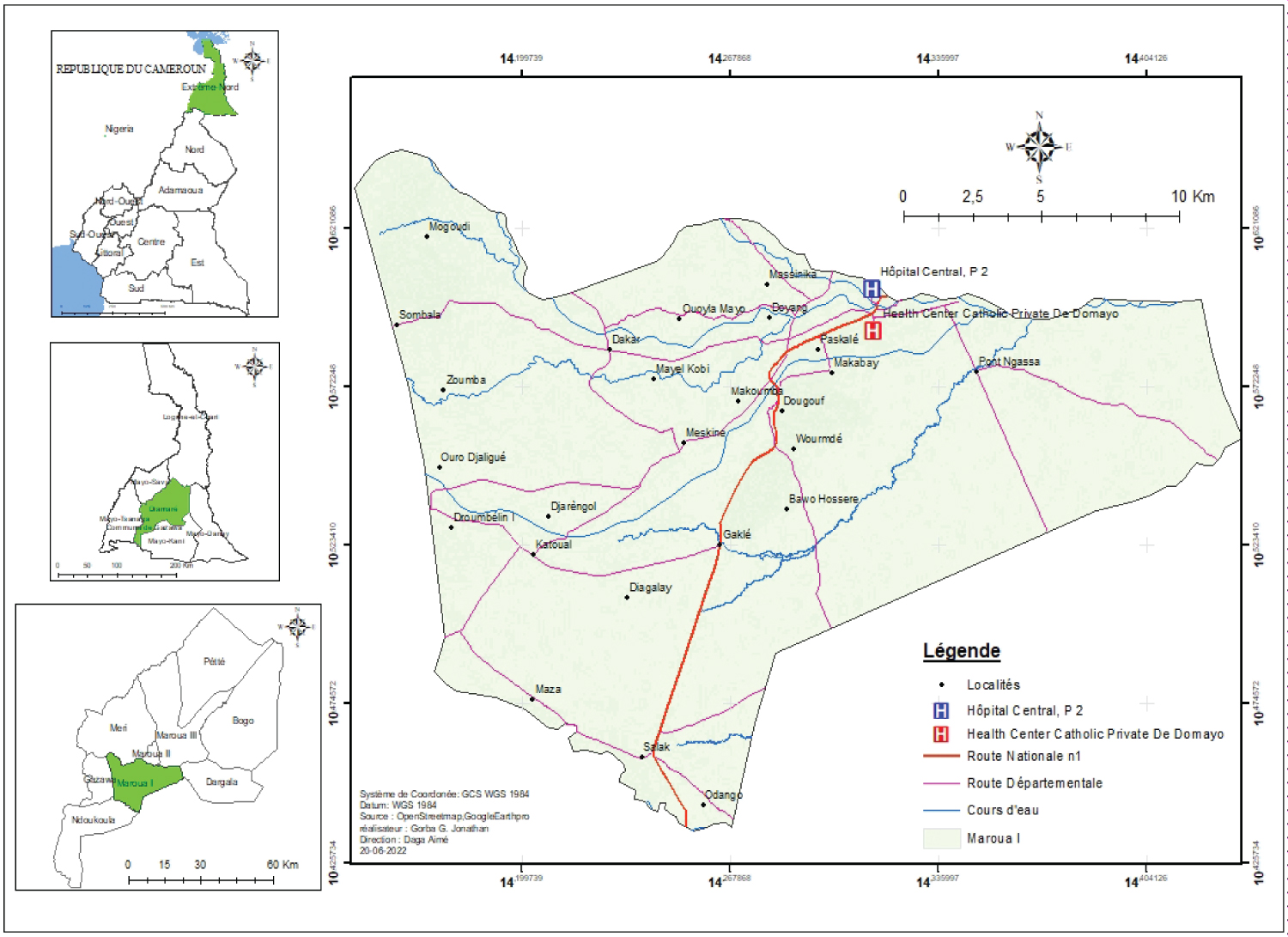 Figure 1: Location of the study sites.
View Figure 1
Figure 1: Location of the study sites.
View Figure 1
Our study population consisted of all pregnant women coming for antenatal consultations at the Maroua Regional Hospital and/or the Domayo Catholic Health Centre in Maroua.
The sample size was calculated according to the Lorentz formula [7]
With
P = Prevalence (35.52%)
Z = 95% confidence interval. It is 1.96
D = the precision of the study with a margin of error of 5% (0.05)
N = Sample size
We obtained a sample size of 351
All pregnant women aged over 20 years, attending ANC of these two hospitals and who signed the informed consent form were included. Were excluded all pregnant women on antibiotics and any pregnant woman not residing in Maroua.
A survey form was filled out by the patient. This form included information on socio-demographic data, the reason for consultation, the presence or absence of signs, and risk factors associated with the infection. Once the participant had complied with the sampling conditions, she was prepared for cervicovaginal sampling. The patient was placed on the bed in a gynecological position and gloves were worn for personal protection. A sterile disposable speculum was inserted into the vagina and tightened the screw so that the cervix is visible for macroscopic examination whose aim is to describe the appearance of the vaginal wall and then assess the abundance of leucorrhoea, its appearance, color and odor. Two swabs were labeled and one was used to collect secretions at the ectocervix and the other at the endocervix, the swabs were coded.
The pH and Potassium Hydroxide (KOH) test: The pH and the KOH test were evaluated on the speculum. In the case of infection with Gardnerella vaginalis, the pH is higher than 4.5. The test was considered positive for KOH when there was a rotten fish smell in case of bacterial vaginitis.
Direct examination of fresh samples: After dilution of the vaginal secretion in a few drops of physiological serum, a direct examination was performed. The preparation was observed with objectives 10x and 40x, to determine the presence of round or oval yeasts, budding or not and mycelial filaments. The identification of yeast cells was based on macroscopic examination of yeast colonies showing a whitish, creamy, slimy or shiny appearance on Sabouraud Chloramphenicol Agar. This was done using the filamentous blast test coupled with the use of Chromogenic Agar Candida. If the blast test is positive, the diagnosis of C. albicans infection is made; otherwise, it is Candida spp and further tests are required for identification.
Prevalence: The prevalence (P) was calculated using the formula:
Resistance profile using an antifungigram: An antifungigram was carried out to evaluate the rate of resistance of the Candida species found in the cervicovaginal samples to antifungal drugs by interpreting the minimum inhibitory concentration (MIC) values obtained. The disk agar diffusion method was used for the antifungigram.
Ethical clearance was obtained from the National Committee on Research Ethics for Human Health. This work was carried out in accordance with the Declaration of Helsinki. All ethical rules involving research with disadvantaged groups such as prisoners have been respected. Patients were free to attend the study without any outside constraints.
The results were analyzed with SPSS version 20. The data were expressed as a percentage. Quantitative data are presented as (CI), and qualitative data are presented as frequencies and percentages. Associations between dependent and independent variables were established using Chi 2 and odds ratio. Significance thresholds were set at 95% confidence intervals and at 5% significance level (thresh holds at p < 0.05).
Table 1 presents the prevalence of vaginal candidiasis among pregnant women according to the Health Centers. It follows from the analysis of this table that the Maroua Regional Hospital had a prevalence of VVC of 53.07% and the Domayo Catholic Private Integrated Health Centre 51.33%.
Table 1: Prevalence of VVC according to Health Centre. View Table 1
Figure 2 presents the prevalence of Candida species isolated according to health centers. It can be seen that 04 species of Candida were isolated from pregnant women attending antenatal clinics, i.e., Candida albicans, Candida glabrata, Candida krusei and Candida tropicalis. Candida albicans had a prevalence of 34.62% and 31.85%, respectively, at the Maroua Regional Hospital and the Domayo Catholic Private Integrated Health Centre.
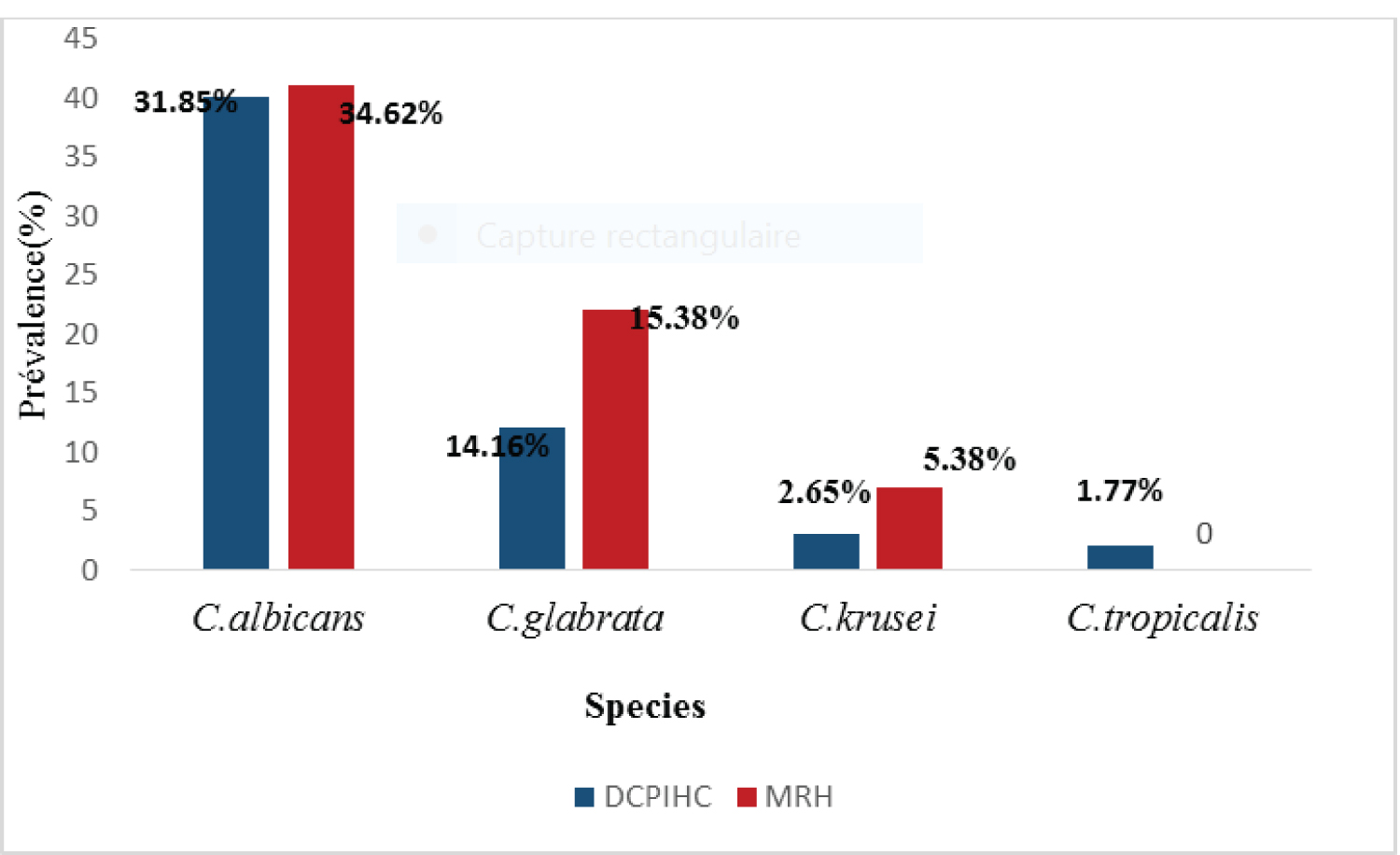 Figure 2: Prevalence of Candida species isolated according to health centre.
View Figure 2
Figure 2: Prevalence of Candida species isolated according to health centre.
View Figure 2
Table 2 shows the prevalence of VVC according to socio-demographic factors. It appears from this table that the most infected (60.49%) age group was 25-30 years. Follow by the age group 30-35 with a prevalence of 50. As far as the religion is concerned Christians where the most infected (52.33). Patients with secondary level education where the most infected (55.75) followed by those with a university level of education (53.88). Those who were married and cohabiting had a prevalence of 50.56 and 55.66, respectively.
Table 2: Prevalence of VVC according to socio-demographic factors. View Table 2
Several clinical signs were associated with the presence of VVC in pregnant women. Table 3 shows the prevalence of VVC according to clinical signs. From this table, the main clinical signs are Painful Urination (57.57%) and vulvovaginal pruritus (54.93%), although there was no statistically significant association (p > 0.05).
Table 3: Prevalence of VVC according to clinical signs. View Table 3
Table 4 shows the Prevalence of VVC with respect to hygienic habits. It follows from the analysis of this table that the hygienic habits frequently seen in this population were mainly the absence of vaginal douching (52.83%) which was not performed per day. Participants who did not use cyteal, water and soap as intimate shower product had high prevalence rate of 52%, 50%, and 53%, respectively.
Table 4: Prevalence of VVC with respect to hygienic habits. View Table 4
Table 5 shows the prevalence of VVC according to obstetrical history. It follows from the analysis of Table 5 that VVCs were mostly seen in nulliparous (42/78) and primiparous (36/66). The first semester and third semester presented high prevalence; however, there was no statistical association between obstetrical history and VVC.
Table 5: Prevalence of VVC according to obstetrical history. View Table 5
The isolated Candida species were tested for resistance to different antifungal drugs and their resistance profile of these Candida species is presented in Figure 3. Contrary to what we could have expected, C. albicans species showed a low resistance rate to Nystatine 100 (0.78%) and higher resistance rate to FLU10 (55.11%), AMB20 (54.33%). Candida glabrata showed variable resistance effects to AMB (25.2%) and KCA10 (24.4%).
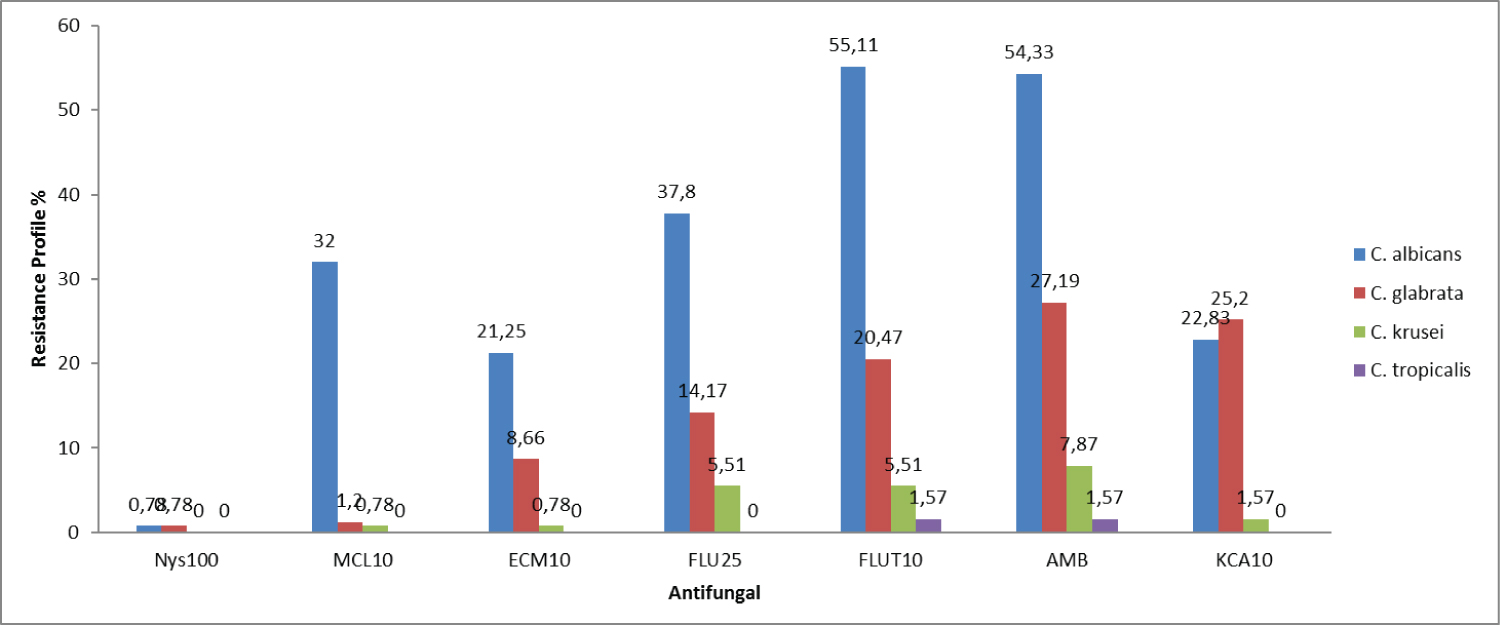 Figure 3: Resistance profile of Candida species to the seven antifungals used. Nys100: Nystatine100; MCL10: Miconazole10; ECM10: Econazole10; FLU25: Fluconazole25; FLU10: 5-Flourocytosine10; AMB: Amphotéricine B.
View Figure 3
Figure 3: Resistance profile of Candida species to the seven antifungals used. Nys100: Nystatine100; MCL10: Miconazole10; ECM10: Econazole10; FLU25: Fluconazole25; FLU10: 5-Flourocytosine10; AMB: Amphotéricine B.
View Figure 3
Table 6 shows the risk factors related to level of education, number of partners, and religion. It follows from the analysis of this table that the main risk factor was the number of partners.
Table 6: Risk factors related to level of education, number of partners, and religion. View Table 6
This descriptive cross-sectional study aimed to determine the prevalence and antifungal resistance profile of Vulvovaginal Candidiasis infections in pregnant women in the city of Maroua. The mycological analysis revealed a prevalence of vulvovaginal candidiasis (VVC) of 53.07% and 51.33%, respectively, at the Maroua Regional Hospital and the Domayo Catholic Private Integrated Health Centre. These results are similar to those of Vroumssia, et al. [8] who obtained a prevalence of 55.4% in the Far-North Region of Cameroon. This result shows that pregnant women in the city of Maroua in particular and in Cameroon, in general, are prompt to mycotic infections, On the other hand, Sylla, et al. [9] presented a slightly lower prevalence (32.6%) than in the present study on their work on vaginal candidiasis in Senegal. This difference could be due to their low sample size and the difference in population and habits.
In the present study, pregnant women of the age group 20-25 years had the highest incidence of VVC (60.49%). Similar results were found by Sylla, et al. [9] and Seema, et al. [10] who showed that VVC affects young women of middle age [20-35]. This age group could be explained by the fact that middle-aged women have a high level of sexual activity. However, during this period of activity, there is a strong discharge of estrogen which favors the acidity of the vaginal environment and leads to a significant deposit of glycogen in the vagina. Our results are in contradiction with those of Hoffman, et al . [11], who showed that VVC affects menopausal women in the USA. This difference may be explained by the fact that their immune system is deficient.
Pregnant women with a secondary school level of educational had the highest prevalence of VVC (55.75%), followed by those with a university educational level (53.08%). Similar observations were reported by Kechia, et al . [4], who showed that secondary school women had more VVC than university students. Vroumsia, et al. [8], contrary to us, they showed a higher prevalence (50%) of VVC among women with a primary level of education than those of other educational levels. This may be due to the fact that they are the most vulnerable because they do not master hygienic conditions. A high prevalence of VVC in married pregnant women (50.56%) and those cohabiting (55.66) was observed. Similar observations were reported by Sylla, et al . [9], showing a high prevalence of married pregnant women. This high rate in married women is considered due to the fact that they are much more sexually active than unmarried pregnant women in this environment.
Vulvovaginal pruritus was the most frequent sign (54.93%), followed by Leucorrhoea (52.81%), associated with a whitish and creamy color. Similar observations were reported by Kechia, et al . [4] who found a higher prevalence of vulvar pruritus (61.70%) and clotted leucorrhoea (60.28%). This contrast with the study conducted by Sobel [12] with pregnant women at the Mother and Child Hospital Centre in Nouakchott (Mauritania). This difference can be justified by the difference in sample size which was low in the present study.
Women practicing frequent vaginal douching presented a prevalence of 50%. Similar studies were conducted by Ane, et al. [13], who found a high prevalence of 52.7% among female students in the South West region (Cameroon) practicing frequent vaginal douching. This high rate among pregnant women who practiced frequent vaginal douching could be due to a change in the vaginal flora and a decrease in pH that favors the growth of yeasts of the genus Candida and the use of aseptic soaps that contribute to the destruction of the vaginal flora.
A prevalence of 54% of VVC among primiparous pregnant women was observed. This result is in agreement with Okonkwo, et al. [14], who obtained high prevalence in primiparous pregnant women.
The highest frequency of VVC in the 3 rd semester of pregnancy compared to the 1 st semester of pregnancy with a prevalence of 65% and 52%, respectively. Our results are in agreement with Sayanika, et al. [15] who showed a prevalence of 57.4% of VVC in the 3 rd semester of pregnancy. This could be explained by the change in vaginal pH and the increase in the level of hormones (estrogen) which provide a source of carbon for the growth of Candida spp.
Yeast of the genus Candida has been incriminated in most of the VVC in pregnant women. In the present study, the most isolated species were Candida albicans followed by Candida. glabrata, Candida krusei, and Candida tropicalis . The species C. albicans was the most predominant with a prevalence of 63.78%. Our results are similar to those of Ogouyémi, et al. [16] in Benin (96.1%) and Kechia, et al. [4] showed a predominance of C. albicans species (80.52%) followed by C. glabrata , This predominance of C. albicans could be explained by its important ability to adhere to the vaginal mucosa thanks to the presence of cell receptors and its virulence The present results, however, contradict the work of Okungbowa, et al . [17], who reported C. glabrata as the most common species among asymptomatic pregnant women in a city in Nigeria. This may probably be due to a significant increase in the incidence of Candida species infections compared to Cameroon and the fact that non-albicans Candida species especially C. glabata continue to replace C. albicans in causing vaginal candidiasis in pregnant women.
In the present study, C. albicans species presented a very high resistance to Amphotericin B (69/54.33%). This is contrary to the study of Kouadio, et al. [18] which shows that no resistance was observed to amphotericin B. This resistance is explained by a decrease in the ability of Amphotericine B (AMB) to bind to ergosterone in plasma membranes. Candida glabrata presented resistance to AMB20 of 27.19%. Contrary to what could have been expected, there was no resistance to nystatin in our study. This efficiency recovery of nystatin could be due to the fact that it has been abandoned for a long period of time and the preference given to other drugs, hence regaining its efficacy. A study conducted in 2011 in Abidjan by Bonouman, et al. [19] showed very high resistance to nystatin and AMB of 92.5% and 98.5%. respectively to C. tropicalis and C. krusei . They equally demonstrated no resistance to nystatin100 and a low rate of resistance to AMB of about 1.57% and 7.87%, respectively, for C. tropicalis and C. krusei .
A resistance profile of 37.80% (FLU25), 32.28% (MCL10) for C. albicans ; 25.20% (KCA10) for C. glabrata was recorded. These results are similar to those of Kouadio, et al. [18]. However, 5-FC presents a very high variability of resistance rates against different species of Candida isolated i.e., C. albicans (55.11%), C. glabrata (20.47%). These results are in line with the study conducted by Kouadio, et al. [18] who presented a resistance of 33.3% to 5-FC.
This study revealed that Nystatin presented no resistance. Which is a drug that is no longer used. This efficacy of Nystatin could be because it has been abandoned for a long period of time and the preference given to other drugs, hence regaining its efficacy. Therefore, there is an urgent need for continuous therapeutic surveillance of VVC in pregnant women.
All data generated and analysed are included in this research article.
The authors declare that no conflicts of interest exist.
The study received no funding from any source or organization.
NDA, NACN, YC, KB conceived the idea and designed the study. SNSR, DDE, LGN, GNGA and NNAS performed the experiments. NDA and LGN analysed and interpreted the data. NACN and YC drafted the manuscript. All authors read and approved the final manuscript.