Blindness is a complication of midfacial trauma and the cause of it may be retrobulbar or intraorbital hematoma, which could be responsible for a direct or indirect damage to the optic nerve, traumatic loss or rupture of the orbital globe. In the international literature, the reported incidence of blindness subsequent to craniofacial injuries, particularly in orbito-frontal, orbito-naso-ethmoidal, zygomatico-orbital and Le Fort II and III fractures ranges from 1-5%.
A retrospective study investigating the etiology, mechanism of trauma that led to visual loss and frequency of blindness due to lesions of midfacial trauma.
A 3-year study of 128 patients with fractures of the midface in which the orbit was involved, who were hospitalized at the University department of Oral and Maxillofacial Surgery at General Hospital of Athens "Evangelismos". 88 fractures were related to the zygomatic complex, 4 were pure blow out, 11 were related to the orbito-naso-ethomidal complex, 17 were Le Fort II and III type and 8 were located exclusively to the orbit. The causes and mechanism of injury that led to blindness were also investigated.
Twelve patients (9.4%) were blinded as a result of the injuries, while in 2 cases (1.6%) the blindness was bilateral. Regarding the mechanism in 10 cases (7.8%) blindness was due to injury to the orbital globe, in one case (0.8%) due to intraorbital hematoma and in one case (0.8%) due to neurotmesis of the optic nerve. In 11 cases (8.6%) blindness was immediate post-traumatic and in one case it was progressive due to development of an intraorbital hematoma.
Midfacial fractures can cause blindness which in most of the cases eventuates simultaneously with the injury. The rupture of the orbital globe is the main cause leading to blindness.
Blindness, Maxillofacial trauma, Midfacial fracture
Patients with a fracture of the middle third of the face have an increased probability of eye injury with initial or subsequent blindness [1-3]. In the orbit the strong bony walls which enclose the eyeball, as well as the muscle cone of the extraocular muscles, protect, facilitate and restrict the excessive mobility of the orbital globe. Furthermore, the long and short posterior ciliary arteries enter the eye around the optic nerve and lie unprotected in the muscle cone, so may be more susceptible to injury than the optic nerve itself and produce anterior ischemic neuropathy, which is a mechanism of visual loss [2,4]. Also, the fat muscle mass of the orbit protects the eyeball from a sudden impact or compression leading to a possible blindness which is an uncommon, but documented complication of facial trauma. The intracranial part of the optic nerve is steadily connected to the bone, so the nerve is immovable and take bleed by a thin capillary net, which can easily destroyed under compression as a result of the increased pressure to the optic foramen after trans-ethmoidal fracture. The intraorbital part of the optic nerve which is approximately 50 mm from the optical cruciate ligament up to the retina has a helical course, thus having a high resistance to pressure, dislocation and generally indirect injuries [5,6]. Fractures that causes blindness originate mainly only from the orbit (like the orbital floor fractures) or from more extensive fractures, such as orbito-frontal, orbito-naso-ethmoidal, zygomatico-orbital and many time Le Fort III fractures [3,7,8].
The causes that lead to blindness due to injury to the midface may be the following: [1,2,9]
• Retrobulbar or intraorbital hematoma
• Traumatic loss or rupture of the orbital globe
• Direct or indirect damage of the optic nerve
• Detachment of the retina
• Hemorrhage of the vitreous body
• Rupture of the sclera
• Damage of the lens
The purpose of this retrospective study is to investigate the etiology, mechanism of trauma that led to visual loss and the frequency of blindness\following facial trauma in patients who were hospitalized at the University department of Oral and Maxillofacial Surgery at General Hospital of Athens "Evangelismos".
128 cases of midface fracture were collected over a 3 year period, in order to investigate the potentiality of posttraumatic blindness. Among them, 88 were zygomatic complex fractures, 4 were pure blow out, 11 were related to orbito-naso-ethmoidal complex, 17 were Le Fort type II and III fractures and 8 were restricted exclusively to the orbit. In patients whose posttraumatic blindness was reported, the causes and the mechanism of trauma that led to the blindness were investigated and detailed medical history, plain X-rays and CT scan were taken. Also, the gender, age, etiology of trauma, type and site of fracture, mechanism, location (left, right or bilateral eye) and time of onset (immediate or delayed) of blindness were recorded (Table 1).
Table 1: Record of 12 patients with posttraumatic blindness and associated orbital injuries. View Table 1
As soon as the ophthalmologic signs and symptoms were recognized, the examination was immediate and included observation of the eyeball according to the shape and color, subconjunctival hemorrhage, movement, ptosis and pain of the globe and corneal reflex. The complete ophthalmologic examination also included visual field, visual acuity and fundoscopy examination in order to exclude edema of the retina and optic disc, iris prolapse, intra-vitreous hemorrhage and presence of foreign body.
Zygomatico-orbital bone fractures were the most frequent type of injury cause blindness followed by Le Fort III-type fractures, while postoperative blindness did not occur in our cases. In a total of 128 cases, 12 patients (9.4% of the facial skeleton fractures) sustained blindness due to trauma (10 due to car accident and 2 from other causes). In two out of these patients (rate of 16.5%) the blindness was bilateral. Concerning the mechanism of blindness, 8 cases (rate of 66.6%) were due to complete globe perforation and rupture (Figure 1), one case (rate of 8.3%) was due to globe rupture and optic nerve compression, one case (rate of 8.3%) was due to retrobulbar hematoma (Figure 2), one case (rate of 8.3%) was due to intraorbital hematoma and vitreoretinal hemorrhage and one case (rate of 8.3%) was due to optic nerve laceration and neurotmesis (Figure 3).
 Figure 1: Oribital globe rupture due to frontal and zygomatic bone fracture.
View Figure 1
Figure 1: Oribital globe rupture due to frontal and zygomatic bone fracture.
View Figure 1
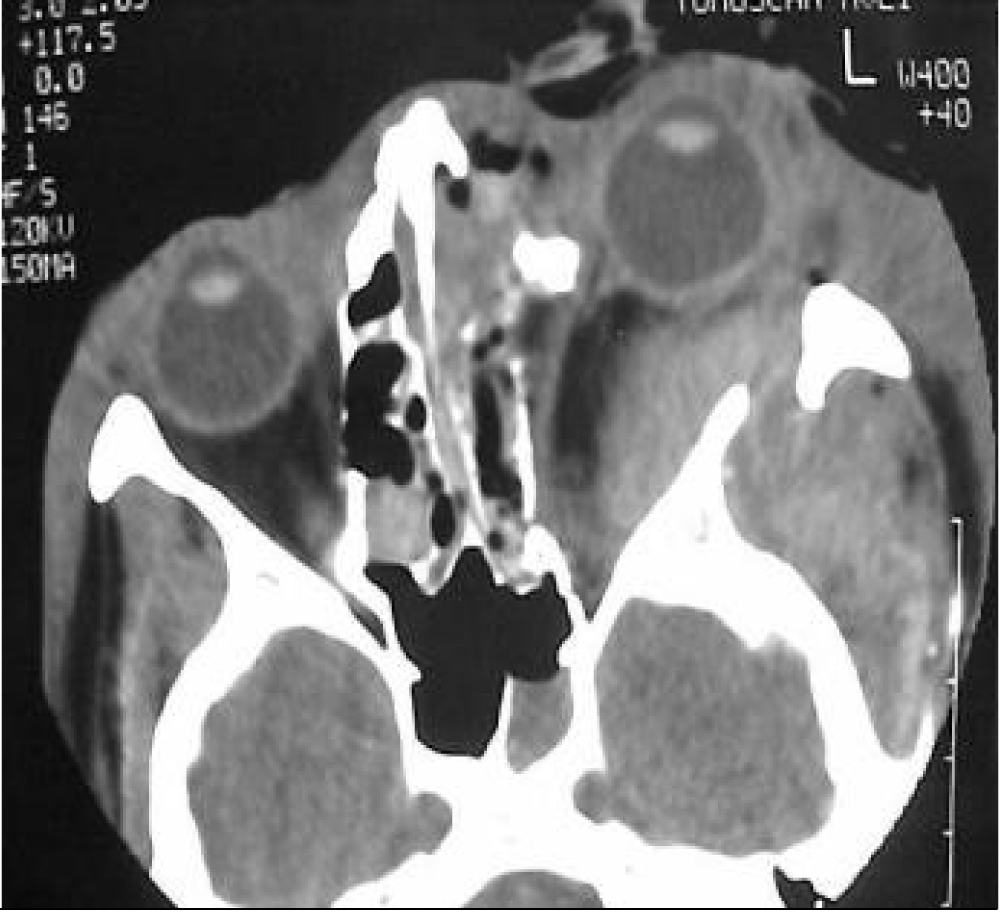 Figure 2: Left retrobulbar hematoma causing indirect injury to the optic nerve (Radiographic examination of CT-scan).
View Figure 2
Figure 2: Left retrobulbar hematoma causing indirect injury to the optic nerve (Radiographic examination of CT-scan).
View Figure 2
 Figure 3: Optic nerve neurotmesis.
View Figure 3
Figure 3: Optic nerve neurotmesis.
View Figure 3
In 11 cases (8.6%) the blindness was immediate posttraumatic and in only one case the progress was delayed due to gradual dilatation of retrobulbar hematoma. In almost all cases, blindness occurred at the time of trauma and the most common cause was orbital globe rupture, while the vision of the patients didn't recover after treatment.
Association between maxillofacial trauma and blindness was first described by Hippocrates, but in modern times the first who discovered that facial trauma may directly lead to fracturing of the optic canal and described that the optic nerve damage was a consequence of orbital bones fracture was Berlin in 1881 [10,11]. Other traumatic causes of blindness are orbital globe rupture, direct or indirect trauma to the optic nerve and ischemic optic neuropathy due to vascular rupture (because of retrobulbar or subconjuctival hematoma, spasm of terminal arterioles and capillary vessels of choroid as a result of compression of the globe) [12-15].
A trauma of the eyeball may lead to blindness according to the number οf fractured bony walls of the orbit [16,17]. So, after an orbital floor fracture and secondary orbital cellulitis can cause transient or permanent complete blindness [18]. Injury to the optic nerve itself is the most common cause of blindness following traumatic fracture. Direct optic nerve damage can happen from the segments of the fractured orbit or even foreign bodies [1,11,12,15]. When the fracture line passes through the optic canal and foramen, the nerve fibers are crushed and splited [11,14,19]. Also, fractures of the anterior cranial fossa may cause elevation of the orbit's roof by their turn and as a result the downward movement of the clinoid processes can crush the optic nerve [11,15]. Indirect damage of the optic nerve can happen by decrease of the orbital volume or by increased pressure to the intraorbital content due to retrobulbar hematoma, edema or hemorrhage of the optic nerve into the optic canal, while can rarely happen after fractures of frontal bone and post-operatively during their fixation [11,15,20]. In these cases, optic nerve compression will follow, which leads to its' ischemia [15]. In contrast, cases with comminuted orbital fractures carry the risk that the subsequent movement of the globe can also cause movement of the intraorbital segment of the optic nerve, while the intrabony segment by its turn can lead to strangulation, blood supply discontinuation and upcoming blindness [14]. Blindness also occurs from insufficient blood supply due to crushing, secondary vascular spasm or thrombosis of vessels supplying blood to the optic nerve and these could have as a result ischemic optic neuropathy [2,8,14]. The globe may suffer reciprocating movements or twist, therefore the forces that are created from the percussion transmitted to the unfractured site of the orbit may lead to the rupture of the intrabony blood supply of the optic nerve. This mechanism leads to optic nerve necrosis after 2 to 3 weeks which can cause blindness. It is also possible, the reciprocating movement of the globe to cause pressure to the optic canal and as a result the rupture of the thin trichoid plexus by its turn evokes damage to optic nerve axons [13,14].
Clinically, closed orbital fractures can decrease the volume of the orbit and cause exophthalmos, which can block the drainage of the hematoma or posttraumatic edema [14]. Retrobulbar hematoma (which demands immediate intervention) in most cases is drained through the fractured floor of the orbit into the maxillary sinus and recognized by the presence of epistaxis. When the hematoma cannot be automatically drained due to clotting or extensive hemorrhage, can take big dimensions and cause pressure to the optic nerve, which leads to interruption of blood supply and ischemia by blocking its corresponding vessels [12,20,21]. Additionally, retrobulbar hematoma can cause ischemia of the central retinal artery [7,8].
The diagnostic examination of patients with midfacial trauma starts with plain x-rays in conjunction with computed tomography, which should include the area of the optic foramen in order not only to get detailed information concerning the type and size of the fractures, but also the potential injury of the optic nerve. Therefore, important information are given for the evaluation of the soft tissue in the area and the extent of the hematoma possibly developed due to trauma [12,19]. Ultrasound of the orbit and 3D-CT can also give important informations [11,20]. The further examination of the optic nerve and its course can be completed with the use of MRI, electro-retinography and electrical stimulation of occipital lobe, which can test the function of the optic nerve [6]. Concerning the prognosis a detailed medical history should be included, which will also give information about the exact time of visual loss [15,22]. Ophthalmologic examination is important in its full aspect and it should be immediate, but often repeated despite the fact that in most cases fails to give sufficient diagnostic and prognostic evidence [8,15]. Clinical ophthalmologic characteristics for possible trauma of the globe which lead to visual loss and viteous body hemorrhage include: [8,12,15,23].
• Opthalmoplegia associated with pain
• Enlarged and tight globe with mydriatic pupil
• Prolapse of globe
• Decreased visual acuity and visual field defects
• Subconjuctival hemorrhage
• Absence of direct light reflex
• Edema of the optic disc
• Diplopia and decreased visual acquity if blindness did not occured
In the international literature, the corresponding average rate of blindness as a result of craniofacial trauma is reported between 1-5 % [9,13,17], while other researchers showing lower rates ranging from 0.04-3.5% [8,14]. However, higher rates of permanent blindness (till 22%) secondary to traumatic midfacial fractures involving the orbit have been published [3,24]. Regarding the mechanism of blindness, direct trauma to the orbital globe corresponds to 1% of blindness, while retrobulbar hematoma is rare and the rate is ranging around 0.3 % [20]. The high rate of blindness that is reported in our study is maybe due to the fact that most of our patients were victims of car accidents and almost all of our cases were not wearing safety belts or protective helmets.
Treatment modalities can be pharmaceutic, surgical or combination with no significant difference in post-treatment visual acuities [1,3,13,25,26]. By clinical experience it is distinguished that if the patients preserve their vision after trauma but eventually lost it, they have greater chances of retrieving it with immediate pharmacologic or surgical intervention, while patients who lost their vision immediate after trauma the blindness usually becomes permanent [8,11]. Nevertheless, when the retrobulbar hemorrhage becomes evident immediately after the trauma, massage to the globe can be applied in order to decrease the intrabulbar pressure and restrict the hematoma [12,22]. The head of the patient should be elevates and anxiolytic medication is provided in order to reduce arterial pressure [8,12]. Mannitol and high doses of corticosteroids are administered immediately and decrease microvascular spasm and edema of small supplying vessels, so the optic nerve necrosis and its indirect injury is avoided [3,12,26]. For drainage of hematoma, if there are soft tissue trauma to the region and the orbital diaphragm is dissected, then can be accomplished through the soft tissue lacerations. Differently it can be achieved with a small incision sideways to the eyelid over or under from the inner canthus or after a canthotomy of lateral palpebral ligament [8,9,12]. Many clinicians prefer the drainage of the hematoma with a Caldwell-Luc approach through the sinus, but the fractured segments of the orbital floor should not be pushed violently upwards in order to avoid damage to the optic nerve, while if the hematoma remains after the sinus packing this should be removed [20]. Immediate decompression of the optic nerve is indicated in cases of retrobulbar hemorrhage (which possibly can lead to the strangulation of the nerve) and drainage of the hematoma in conjunction with the immediate fixation of the fractured bony segments must be completed, while has even better results in patients with gradual visual loss and should be done as soon as possible [6,19]. In contrast, other clinicians believe that the surgical decompression of the optic nerve can be achieved even 7 days after trauma [5], whereas in traumatic optic neuropathy observation seems to be enough [9]. The surgical approaches for optic nerve decompression differ and the method of choice is the trans-ethmoidal approach, although requires enough experience [1,3]. The aspiration with a needle is not applied, because it is known that the volume of the retrobulbar hematoma should be at least 30-50 ml in order to cause nerve damage, while with aspiration the volume is slightly decreased [12]. Finally, if the line of fracture passes through the optic foramen and the blood supply to the optic nerve is possibly blocked, then any of the interventions, immediate or delayed, has doubtful results [19].
Blindness following facial fracture is a rare documented complication of injury in the orbital region [3]. It is usually caused during the trauma, while orbital globe rupture and optic nerve neurotmesis are the main causes that lead to visual loss. The assessment of intrabony course of optic nerve inside the optic canal with the use of computed tomography is important. In the case of permanent blindness which happens during injury, the surgical intervention does not usually help in the retrieval of the vision, while when the blindness is gradual the nerve decompression is indicated. The decision for surgical intervention should be selected individually taking into consideration all the parameters. Furthermore, the trans-ethmoidal approach for nerve decompression remains the method of choice compared to the transfrontal approach. However, the appropriate treatment modality for patients suffering blindness secondary to blunt head trauma continues to be debated [1,3].