Facial cellulitis is a diffuse non fluctuant inflammation of soft tissue that is not confined and tends to spread, and can be life-threatening.
A 14-years-old girl suffering from facial cellulitis; trismus and dysphagia was admitted to hospital; assuming that facial cellulitis was caused by ophthalmic infection.
Oral examination and orthopantomogram revealed odontogenic infection; caused by buccaly mal-aligned left maxillary third molar. The patient was treated by intra-oral incision at maxillary premolar region, antibiotic and warm saline mouthwash every 1 hour. Drainage of pus happened after two day through the incision. The offending tooth was extracted with local anesthesia after complete resolution of swelling and trismus.
Oral examination and Orthopantomogram are essential in diagnosis of facial cellulitis. Incision is mandatory and life-saving, even if there is no fluctuation of pus to allow relief of gases, also, immediate warm saline mouthwash help localization and drainage of pus.
Facial cellulitis, Fluctuation, Incision
A 14-years-old girl was admitted to the emergency department of Alexandria university hospital, suffering from facial cellulitis, closing her left eye, without fluctuation trismus, dysphagia and fever for 2 days. It was assumed by the physicians who examined her that the cause of facial cellulitis is ophthalmic infection, and was given antibiotic therapy and eye-drops for 3 days with no improvement (Figure 1). Then, the patient was referred for maxillofacial consultation. By taking history, there was no previous dental pain, and severe facial swelling occurred suddenly. Oral examination was done with difficulty due to trismus; and there was no caries or calculus in all her teeth. Orthopantomogram have shown buccaly inclined maxillary left third molar (Figure 2). Diagnosis was made that the facial cellulitis was caused by pericoronitis related to partially erupted buccaly mal-aligned left maxillary third molar tooth, causing abscess in buccal space, canine fossa space, and parapharyngeal space.
 Figure 1: A) Facial Cellulitis in left side of the face; B) Incision made in buccal sulcus at left maxillary premolar region. View Figure 1
Figure 1: A) Facial Cellulitis in left side of the face; B) Incision made in buccal sulcus at left maxillary premolar region. View Figure 1
 Figure 2: O.P.G. showing disto-bucco-angular left maxillary third molar tooth. View Figure 2
Figure 2: O.P.G. showing disto-bucco-angular left maxillary third molar tooth. View Figure 2
Informed written consent was obtained from the patient to be treated by intra-oral incision at the maxillary premolar region, not in the buccal side of posterior maxilla, due to limitation of mouth opening, to allow relief of gases, followed by antibiotic treatment (Hibiotic 625 mg) every 8 hours for 3 days only, and the patient was instructed to do warm saline mouthwash every 1 hour for at least 3 days.
Drainage of pus through the incision occurred after one day through the incision that was made, and complete resolution occurred after two days. Then, extraction of the offending tooth was done with regular local anesthesia (posterior superior alveolar infiltration & greater palatine infiltration) after complete resolution of swelling and trismus (Figure 3). Complete resolution of facial cellulitis occurred two day after offending tooth extraction (Figure 4).
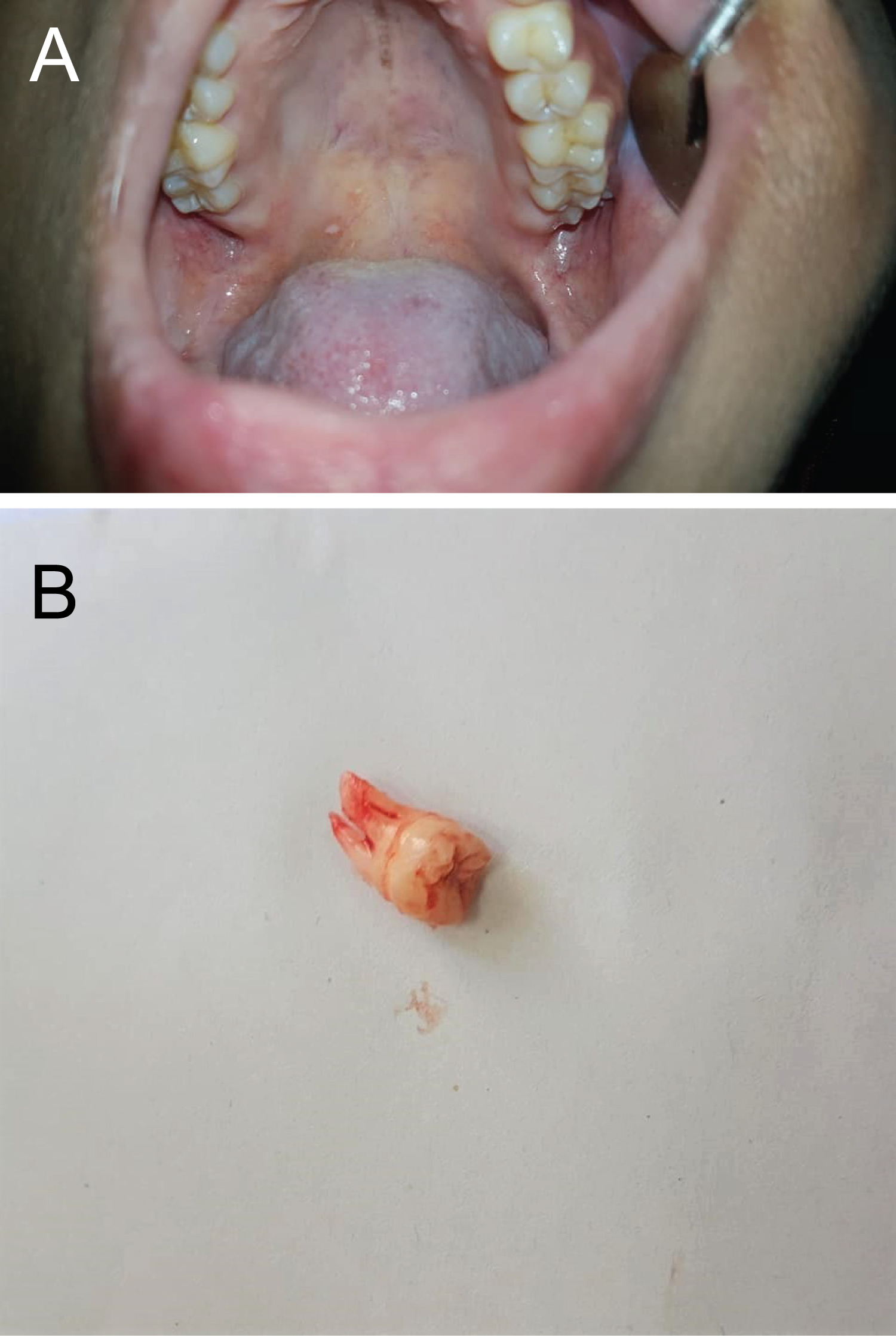 Figure 3: A) Clinical examination showing mal-aligned bucco-angular left maxillary third molar; B) Left maxillary third molar tooth extracted, and post-op antibiotic prescribed. View Figure 3
Figure 3: A) Clinical examination showing mal-aligned bucco-angular left maxillary third molar; B) Left maxillary third molar tooth extracted, and post-op antibiotic prescribed. View Figure 3
 Figure 4: Complete resolution of swelling two days after tooth extraction. View Figure 4
Figure 4: Complete resolution of swelling two days after tooth extraction. View Figure 4
About 62 % of oral and maxillofacial space infections are odontogenic in origin [1]. Sever odontogenic infections are generally secondary to pulp necrosis, periodontal disease, pericoronitis, or per-apical lesions. Dissemination of odontogenic infections causing facial cellulitis is a common problem in the field of oral and maxillofacial surgery [2]. Patients with facial cellulitis are usually hospitalized due to the perceived risk for complications. Odontogenic infection can cause serious multi-space infections in the head and neck regions, which can result in life-threatening complications [3]. When facial cellulitis is detected, there are causes to consider in diagnosis; ophthalmic infection, ENT infection, or odontogenic infection [4]. In the present case, intra-oral examination was not performed, because the patient had no dental pain, and no previous attacks of pericoronitis. CT was not performed, as it is not routinely used for diagnosis of facial cellulitis due to its high cost.
The authors recommend multidisciplinary clinical examination by ophthalmic, ENT and maxillofacial clinicians for proper diagnosis and management of facial space infection. Orthopantomogram is an affordable diagnostic tool, and intra-oral examination is essential during routine physical examination of patients suffering facial cellulitis for proper diagnosis and management. In addition, immediate incision is mandatory and life-saving in facial cellulitis, even if there is no fluctuation to allow relief of gases and the warm saline mouthwash help localization of pus and drainage through the incision.
The authors report no conflict of interest.
Consent for publication of images was obtained.
No funding needed for this work.