Osteoradionecrosis treatment is challenging for clinicians. Throughout history, the study of osteoradionecrosis and its pathophysiological understanding has given the guidelines for managing this pathology. Currently, osteoradionecrosis is understood as a radiation-induced fibro-degenerative process, so its management focuses on reducing the molecular mediators involved during the process. We present the case of a 61-year-old male patient with multiple comorbidities and medical history of the floor of mouth cancer treated with radiotherapy. After extracting a mandibular tooth, osteoradionecrosis with pathologic fracture and orocutaneous fistula developed in the mandibular body. Due to multiple advanced inferior extremities atheromatosis and comorbidities, a fibula microvascular free flap was contraindicated.
Thereby, long-term combination therapy of Pentoxifylline and Tocopherol was established, followed by a sequestrectomy with Advance Platelet Rich Fibrin membranes application. After 16 months of treatment and periodic check-ups, symptoms resolved completely with complete healing of the orocutaneous fistula and preservation of the alveolar and mandibular bones. Multiple guidelines have been proposed to treat osteoradionecrosis. However, the vast majority are based on radical treatments that generate physical and psychological consequences for patients. Therefore, conservative surgical management combined with PENTO and A-PRF could play a role in managing advanced-stage ORN in cases that showcase contraindications for mandibular microvascular reconstruction.
Osteoradionecrosis, Pentoxifylline, Alpha-Tocopherol, A-PRF, Mouth neoplasms
Osteoradionecrosis (ORN) of jaws corresponds to one of the most severe and debilitating radiation therapy complications for treating malignant head and neck pathologies [1]. Currently, ORN is defined as the exposure of necrotic bone that persists for more than three months in a previously irradiated area at a dose greater than 50 Gy and that is not caused by recurrence of a tumor [2]. The reported incidence of ORN ranges from 2.6 to 15%, and it occurs between 22 and 47 months after radiation treatment [3].
Regarding the pathophysiology of ORN, Delanian, et al. [4] postulated that ionizing radiation induces a fibroatrophic process, which through tissue damage and the consequent release of reactive oxygen species, generates a non-regulation of fibroblast activity.
Among the risk factors associated with ORN development are the location of the primary tumor, the stage of cancer (III, IV), acritical radiation dose > 50 Gy, previous surgery on the primary tumor (mandibulectomies or osteotomies before radiation), poor oral hygiene, dental extractions or bone trauma after radiotherapy (RT), tobacco and alcohol consumption, and diabetes mellitus [3]. On the other hand, different ORN classifications exist. The most accepted classification corresponds to the stages of Notani, et al. [5], who through the clinical and radiographic description of the mandibular bone, divided the ORN into three stages (I, II, III) ascending in gravity.
ORN management is controversial. Small areas of exposed bone have traditionally been treated by conservative management consisting of mouthwashes, analgesia, and antibiotic therapy for acute infections. Local debridement and sequestrectomy have been suggested for grade II ORN, while for advanced ORN stages, such as grade III, wide resection with immediate microvascular reconstruction has been used [1,4,5].
This report aims to present the clinical management of a long-standing ORN patient with a posterior pathological fracture due to floor of mouth cancer based on Pentoxifylline- Tocopherol (PENTO), Advanced Platelet Rich Fibrin (A-PRF) and conservative surgical treatment.
A 61-year-old male patient diagnosed with ORN with one year of development posterior to the extraction of tooth 3.6, which was treated at another medical center, consulted to our Oral and Maxillofacial surgery department.
Within the morbid antecedents, a history of a squamous cell carcinoma on the mouth floor (T1, N0) was diagnosed in 2010, treated by local removal surgery and post-surgical radiation with a total radiation dose of 60 Gy. Also, the patient has insulin-requiring type II diabetes mellitus (IRDM), severe arterial hypertension, heart failure, rheumatoid arthritis, bronchial asthma, and a history of acute myocardial infarction. Among the drugs consumed were NPH insulin (am/pm), metformin, acetylsalicylic acid, losartan, hydrochlorothiazide, and salbutamol. Concerning habits, tobacco consumption for more than 30 years, which was not suspended after oral cancer treatment.
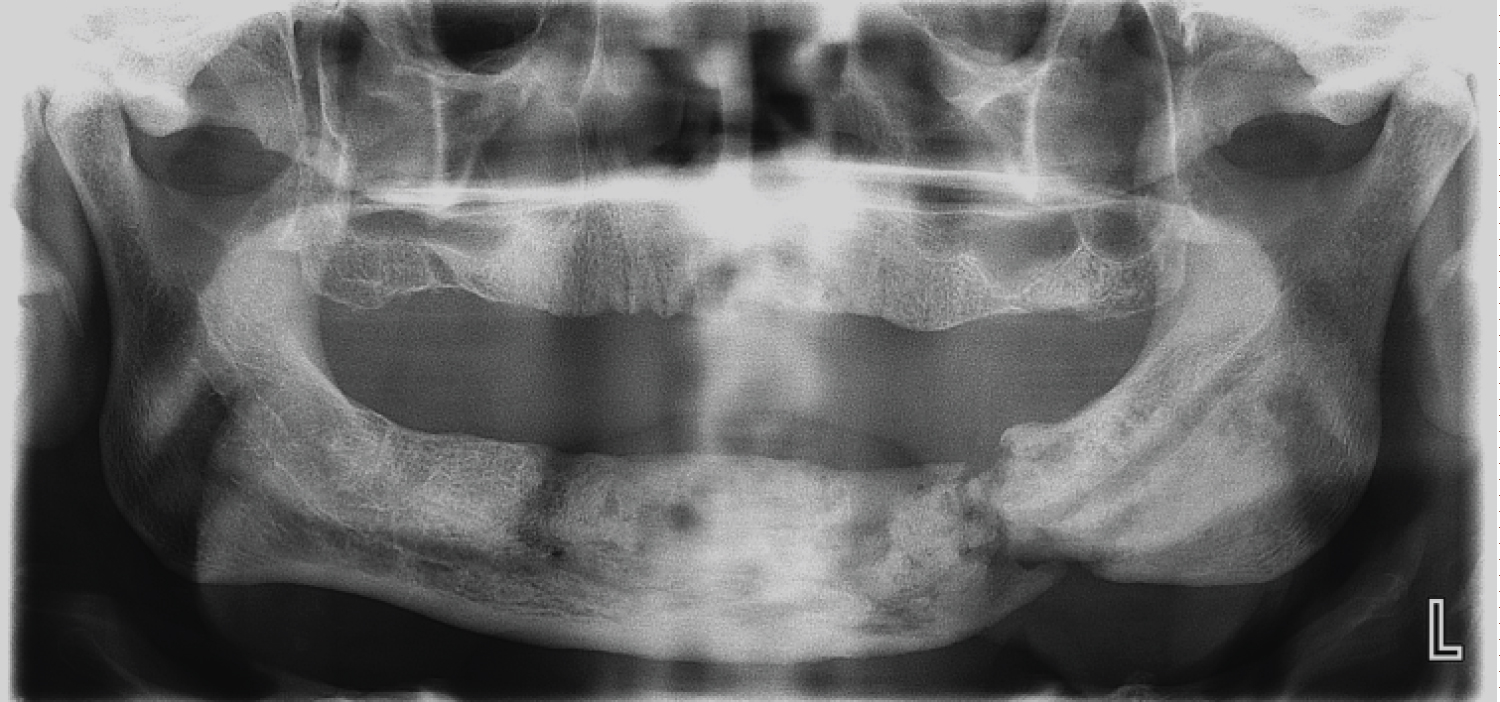
The extraoral examination revealed a volume increase and a cutaneous fistula with purulent drainage in the left submandibular area. On intraoral examination, an upper partial edentulism with multiple cervical caries, and a mandibular edentulism with an increase in volume in the left alveolar ridge, with bone exposure in the tooth area 3.6. Also, a 3 mm mobile bone sequestration was observed in the lower lingual area, and a vestibular bone exposure of 2 mm. The patient was hospitalized for decompensated IRDM and intravenous antibiotic therapy with Ceftriaxone 2 gr/day and Clindamycin 600 mg every 8 hours. An Orthopantomography (OPG) was requested, which revealed diffuse radiolucent areas compatible with pathological mandibular fracture and basilar bone sequestration (Figure 1). A computerized axial tomography (CT) revealed diffuse hypo and hyperdense areas with destruction processes and multiple bone sequestration that reached the basilar border. Besides confirming ORN diagnosis and ruling out tumor recurrence at the affected site, a positron emission tomography (PET-CT) was requested, which showed isolated bone fragments compatible with sequestration and bone metabolic hyperactivity suggestive of osteomyelitis, confirming the diagnosis of ORN Notani stage III (Supplementary Figure 1B, Supplementary Figure 1C and Supplementary Figure 1D). An angio-CT of inferior extremities was requested to evaluate the eventual mandibular reconstruction with fibula free flap. The images showed advanced multiple atheromatosis, which within the context of the multiple comorbidities of the patient contraindicated this procedure.
 Figure 1: Diagnostic OPG where a fracture in the pathological bone and the presence of multiple bone sequestration are observed. View Figure 1
Figure 1: Diagnostic OPG where a fracture in the pathological bone and the presence of multiple bone sequestration are observed. View Figure 1
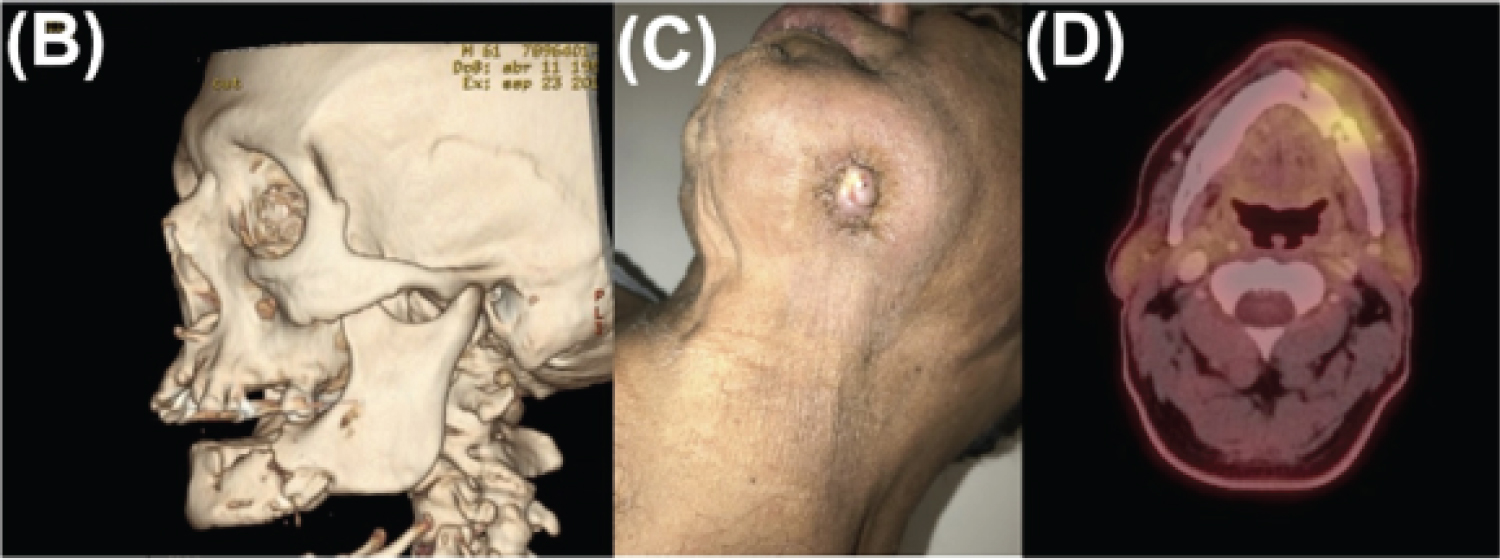 Supplementary Figure 1: B) CT-Scan showing a pathological fracture in the left mandibular body, with the presence of multiple bone sequestration; C) Active orocutaneous fistula in the skin of the left submandibular region associated with refractory ORN and D) PET-CT with areas of mandibular bone metabolic hyperactivity. View Supplementary Figure 1
Supplementary Figure 1: B) CT-Scan showing a pathological fracture in the left mandibular body, with the presence of multiple bone sequestration; C) Active orocutaneous fistula in the skin of the left submandibular region associated with refractory ORN and D) PET-CT with areas of mandibular bone metabolic hyperactivity. View Supplementary Figure 1
After stabilizing IRDM and a favorable response to antibiotic therapy with decreased inflammatory parameters and local clinical improvement, hospital discharge was granted. Conservative treatment was started with Amoxicillin 875 mg + Clavulanic Acid 125 mg every 12 hours × 14 days, plus mouthwashes with 0.12% chlorhexidine and fistular irrigation. A pap-like regimen, smoking cessation, and optimization of hyperglycemia management were indicated.
After the initial treatment, PENTO therapy (Pentoxifylline 400 mg and Tocopherol 400 IU, both every 12 hours) was established on a permanent basis. It was planned that three months after starting PENTO, a basilar fragment sequestrectomy, surgical cleaning, and eventual mandibular stabilization with external devices would be performed; however, due to the COVID-19 pandemic, it could not be performed on the estimated time. Thereby, PENTO was kept for approximately ten months. During this period, clinical improvement was observed on the oral mucosa level without areas of bone communication and minimum purulent secretion.
The remaining maxillary teeth extractions were performed in two surgical stages using atraumatic technique and socket filling with Advanced Platelet Rich Fibrin (A-PRF) plugs due to decreased local trauma in the affected area. Once elective surgical procedures were allowed during the pandemic period, we started with injections of liquid fibrin-rich plasma before lifting the intraoral mucoperiosteal flap to expose the affected site on the left mandible. Then, a surgical cleaning was performed to remove basilar bone sequestration, necrotic tissue, washing with injectable Clindamycin directly into the affected site, filling with A-PRF membranes [6] and fistulectomy. Notably, during intraoral exposure of the mandibular alveolar ridge, the presence of a fibrous callus was observed on the affected area without mobility in the margins, for which it was decided intraoperatively not to stabilize the bone fragments (Figure 2).
 Figure 2: Intraoperative view showing fibrous callus formation in a site previously affected by ORN. View Figure 2
Figure 2: Intraoperative view showing fibrous callus formation in a site previously affected by ORN. View Figure 2
A favorable clinical evolution was observed in the post-surgical controls with the oral mucosa's healing (Supplementary Figure 2). Also, there was an absence of inflammatory-infectious signs, and complete remission of the cutaneous fistula was seen (Supplementary Figure 3). As of this report's date, the patient remains with PENTO therapy, completing a total period of 16 months with monthly clinical and radiographic controls. Radiographically, initial signs of ossification in the alveolar area of the compromised region, and an absence of osteolysis and of new bone sequestration have been observed (Supplementary Figure 4).
 Supplementary Figure 2: Post-operative control 6 months after the sequestrectomy plus the application of A-PRF membranes, which shows a healthy mucosa without signs of inflammation and suppuration. View Supplementary Figure 2
Supplementary Figure 2: Post-operative control 6 months after the sequestrectomy plus the application of A-PRF membranes, which shows a healthy mucosa without signs of inflammation and suppuration. View Supplementary Figure 2
 Supplementary Figure 3: Lower view of the jaw showing complete healing of the orocutaneous fistula. View Supplementary Figure 3
Supplementary Figure 3: Lower view of the jaw showing complete healing of the orocutaneous fistula. View Supplementary Figure 3
 Supplementary Figure 4: OPG control at 16 months after PENTO. Radiopaque areas are observed between fractured strands suggestive of initial ossification stages. View Supplementary Figure 4
Supplementary Figure 4: OPG control at 16 months after PENTO. Radiopaque areas are observed between fractured strands suggestive of initial ossification stages. View Supplementary Figure 4
This case presented a favorable response to conservative management of a Notani III stage ORN, where surgical resection and subsequent microvascular graft are the conventional choice therapies. To our knowledge, this report is one of the few that combined conservative surgical management and drug therapy in a patient with multiple comorbidities [1-3,5].
When radical surgery with microsurgical reconstruction is not possible, conservative pharmacological therapy has been proposed on the basis of the pathophysiological mechanisms of ORN with a long-term regimen [1,4,7]. The use of PENTO has been proposed in order to counteract the effects of ORN-associated fibroatrophy phenomena. Pentoxifylline corresponds to a drug that has been shown to have vasodilator, TNF-a suppressing, inhibition of inflammatory reactions and platelet aggregation, along with an increase in erythrocyte flexibility [4-7]. Moreover, Tocopherol is a potent antioxidant effective in inhibiting free radicals. The use of PENTO has been reported, in patients with advanced ORN, not suitable for resection due to comorbidities. Delanian, et al. [4] described the treatment of 6 patients with pathological fractures, where 5 showed clinical improvement with resolution of the fracture. Breik, et al. [7] reported two patients with pathological fractures and orocutaneous fistulas successfully treated with PENTO. A systematic review that included patients with advanced-stage ORN or refractory to other treatments suggested considering the administration of PENTO for a minimum of 6 months and until regression of the condition is observed. Also, a proportion estimate of 60% recovery was obtained in patients treated on a PENTO basis [8].
Another complementary technique is the use of A-PRF [6]. This fibrin network obtained from blood seeks to accumulate platelets, cytokines, and growth factors to optimize local angiogenesis, an essential process to achieve adequate tissue restoration. Other studies have shown that A-PRF acts as a reservoir of bioactive molecules that promote tissue repair and bone regeneration, induced by cell proliferation, migration, and differentiation in conjunction with anti-inflammatory properties. It is imperative that the affected area is free of malignant neoplasia and that there is no metastasis within the area where A-PRF will be applied, since the growth factors contained therein also play a key role in tumor angiogenesis [9].
Reasonable control of oral hygiene translates into a 1/3 reduction in ORN appearances. Otherwise, patients with a history of addictions show an increase in the incidence of ORN. Diabetes mellitus is considered the most determining systemic factor for the appearance of ORN (Hazard Ratio: 2.99), being also the most frequent systemic pathological condition among these patients, considering that such population is more susceptible to development of infections [2,10].
Finally, conservative surgical management combined with PENTO and A-PRF could play a role in advanced-stage ORN development in cases in which a contraindication for microvascular mandibular reconstruction exists. In the case presented, the patient showed a union of the pathological fracture, remission of the orocutaneous fistula, and healing signs. Although randomized clinical trials are lacking, this management could be a minimally invasive surgical treatment.
None.
The authors report no competing interests.
An exemption statement was obtained from the ethics board.
Written consent was obtained for publication.
No funding was received for this study.